 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
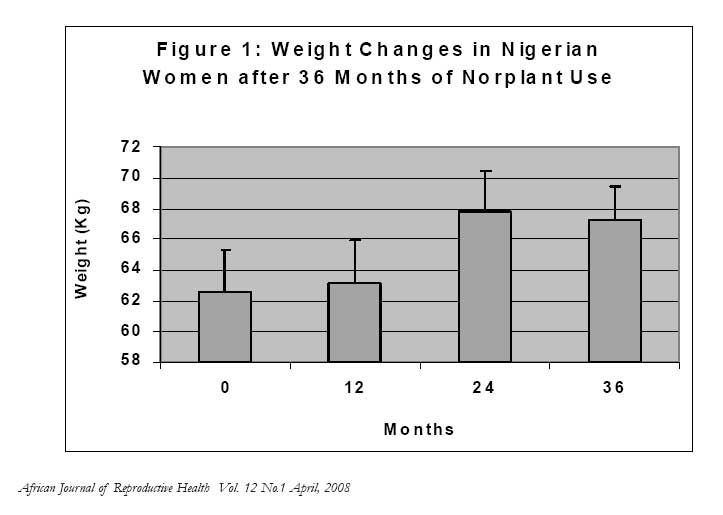
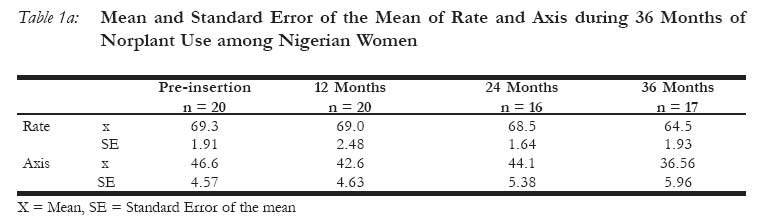
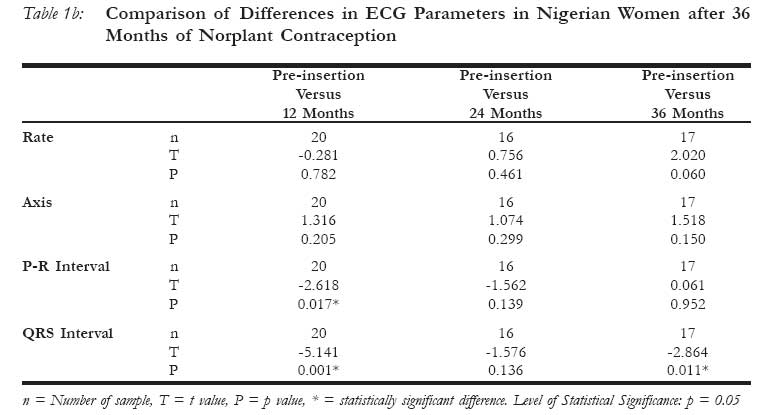
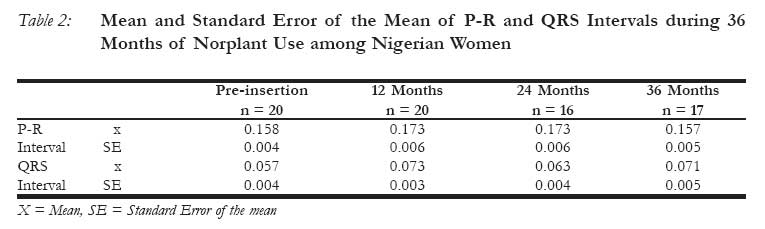
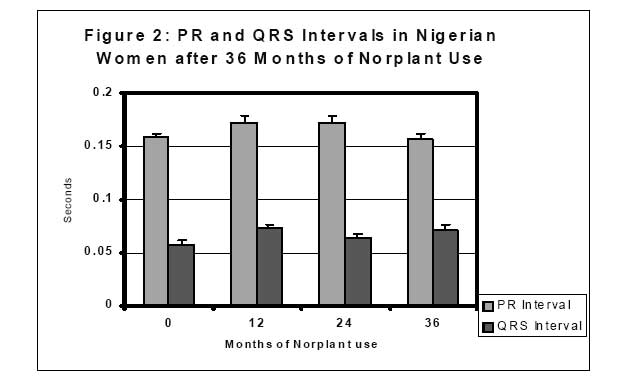
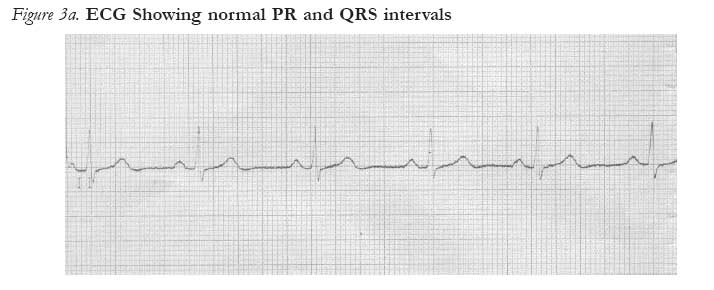
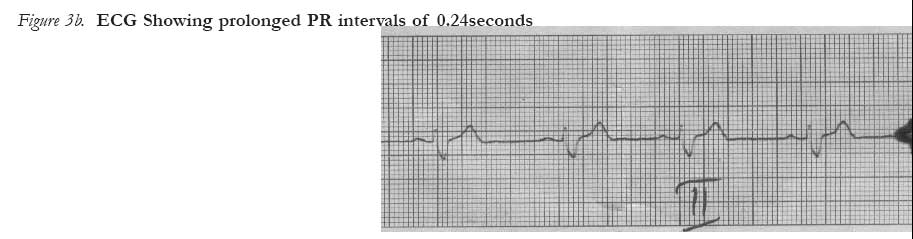
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 47-53 Evaluation of Cardiovascular Morbidity in Nigerian Women after 3 Years of Norplant® Contraception Evaluation de la morbidité cardiovasculaire chez les femmes nigérianes après trois ans de la contraception Norplant *AS Sagay1, BN Okeahialam2, GE Imade1 , AO Aisien3 1Dept. of Obstetrics and Gynaecology, 2Dept. of Medicine Faculty of Medical Sciences, University of Jos, P.M.B. 2084, Jos, Nigeria. 3Dept. of Obstetrics and Gynaecology, University of Benin Teaching Hospital, Benin City, Nigeria. Code Number: rh08007 ABSTRACT This study was conducted to determine any cardiovascular morbidity with Norplant® use by electrocardiography. Thirty Nigerian women seeking long-term reversible contraception were recruited. The clients had baseline blood pressure checks and electrocardiography (ECG) tracings. These were repeated at the 12, 24 and 36 months follow-up visits and the results were analysed. The mean age of subjects was 32.4± 3.98 years. The mean weight at pre-insertion and at the 12, 24 and 36 months follow-up visits showed a statistically significant rise after 2 years (p<0.01). The blood pressures did not show any significant changes throughout the period of study. There was statistically significant prolongation of the PR and QRS intervals at the 12 month visit; mean PR interval (seconds) pre-insertion 0.153± 0.003, and at 12 months 0.173±0.006 (P=0.019), mean QRS interval (seconds) pre-insertion 0.056±0.003 and at 12 months 0.074±0.002 (P=0.005). After 3 years of Norplant use, prolongation of the mean QRS interval remained evident (p=0.011) while mean PR interval had returned to pre-insertion levels. There is a tendency to prolongation of PR and QRS (ECG) intervals in Norplant users; accordingly, it may be prudent for clients with cardiac conditions showing longer ECG intervals, to consider alternative methods of contraception. KEY WORDS: Norplant contraception, ECG, Cardiovascular morbidity, Nigeria RÉSUMÉ Cette étude a été menée pour déterminer toute morbidité cardiovasculaire suite à l’utilisation de Norplant par l’électrocardiographie. Trente femmes nigérianes qui recherchent une contraception réversible à long terme ont été recuitées. Les clientes ont eu des contrôles de pression sanguine de départ et les tracées de la cardiographie (ECG). Ceuxci ont été répétés au cours des visites de surveillance de 12, 24 et 36 mois et les résultats ont été analysés. L’âge moyen des participantes était de 32.4 ± 3.98 ans le poids moyen au moment de la pré-insertion et pendant les visites de surveillance de 12, 24 et 36 mois a indiqué une augmentation importante statistiquement après deux ans (p < 0,01). Les tensions artérielles n’ont pas changé de manière significative pendant la période de l’étude. Statistiquement, il y avait une prolongation importante des intervalles PR et QRS au cours de la visite de 12 mois. L’intervalle PR moyen (secondes) de la pré-insertion 0,153 ± 0,003 et à 12 mois 0,074 ± 0,002 (P = 0,005). Après 3 ans de l’utilisation de Norplant, la prolongation de l’intervalle QRS moyen est restée évidente (P = 0, 011) alors que l’intervalle PR moyen était revenu aux niveaux de la préinsertion. Il y a une tendance vers la prolongation des intervalles PR et QRS (ECG) chez les personnes qui utilisent Norplant ; ainsi, il sera peut-être prudent de la part des clientes qui ont les maladies de cœur indiquant les intervalles ECG plus prolongés, de considérer d’autre méthodes de contraception. Introduction Levonogestrel subdermal implant (Norplant®) is an effective progestogen-only long term method of contraception. Over the years, it has gained acceptance world-wide.1,2,3 Our centre was involved in a multi-centre clinical trial of the safety and efficacy of this method of contraception.4 It was on the basis of studies involving mostly hard-tubing implants that regulatory agencies in 60 countries approved Norplant for five years of use. The later implants are made from soft tubing which are less dense and release hormone at a higher rate. Studies using the soft tubing implants showed that the cumulative seven-year pregnancy rates among users of Norplant are comparable to rates among women who have been surgically sterilized.10 Major depression, panic disorders and other serious adverse effects have been attributed to Norplant use.11,12 The cardiovascular effects of long term use of hormonal contraception have continued to generate interest. Studies on the cardiovascular effects of Norplant® have focused largely on the evaluation of changes in serum lipids and blood coagulation and the findings have been equivocal.5-9 Changes in the electrical activity of the heart may provide information on cardiovascular morbidity. We have studied the effects of Norplant® on electrocardiography (ECG) tracings among apparently healthy Nigerian women using this method of contraception over a 3-year period. Methods Thirty Nigerian women seeking long-term reversible contraception were recruited for the study during a Norplant® training programme at the Jos University Teaching Hospital (JUTH), Jos. They all gave informed consent and had baseline blood pressure checks and electrocardiography (ECG) tracings. None of them was hypertensive and none gave a history or had signs suggestive of heart disease. Hypertension here was defined as a blood pressure greater than 140/90 mmHg measured supine at the end of the physical examination. A table mercury sphygmomanometer was used. Korotkoff phase one was used for systolic and Korotkoff phase five was used for diastolic blood pressure. In the occasional case where phase 5 occurred at zero level, phase four was used for diastolic blood pressure. After cardiovascular disease was excluded, they had Norplant® implanted by one of the authors (ASS) assisted by other doctors and nurses in the family planning unit. Electrocardiography Methods: All subjects had base line ECG tracings using a three channel machine - Fukuda Denshi ECG/Phono system; model FD31P, made in Tokyo by Fukuda Denshi Company. The tracings were recorded at a paper speed of 25 mm/second. ECG tracings were repeated for each subject at the 12, 24 and 36month follow-up visits. From the ECG tracings, the following were measured by one of us (BNO). The PR interval was measured in seconds from the beginning of the P wave to the onset of the QRS complex. The QRS interval was measured in seconds by counting the number of small squares over a QRS complex, each small square being 0.04 seconds. The rate and axis were measured in the standard fashion. Comments were also made on the rhythm and presence of any chamber enlargement. No subject who attended less than twice was used. Data were analysed using SPSS statistical software package. P values <0.05 determine significant differences. Results Among the 30 clients who were initially recruited, only 21 (70%) attended follow-up beyond 12 months. Three (10%) of the clients discontinued Norplant before 12 months, 2 on account of irregular vaginal bleeding and one following persistent pressure from her husband to try for another pregnancy. Six clients were lost to followup. We analysed only the data of the 21 clients who attended the minimum stipulated number of visits 12 months and beyond. The mean age of subjects was 32.4±3.98 years (range 25-38 years). The mean weights at pre-insertion and at the 12, 24 and 36 months follow up visits were 63.63±10.43, 62.29±12.25, 66.53±11.15 and 67.28±10.53 kilograms respectively showing a statistically significant rise after 2 years (p<0.01). The weight changes are shown in Figure 1. The systolic and diastolic blood pressures did not show any significant changes throughout the period of study. The heart rate and cardiac axis measurements did not show any significant changes during the study period. There was no chamber enlargement or hypertrophy. Rhythm remained generally normal. The PR and QRS intervals remained within normal limits throughout the study period. However, they seemed to be significantly prolonged - mean PR interval (seconds) preinsertion 0.153± 0.003, and at 12 months 0.173±0.006 (P=0.019), mean QRS interval (seconds) pre-insertion 0.056±0.003 and at 12 months 0.74±0.002 (P=0.005). After 3 years of Norplant use, prolongation of the mean QRS interval remained evident (p=0.011) while the mean PR interval had returned to pre-insertion levels (Table 1a, 1b, 2, Figure 2, 3a, 3b and 3c). Discussion The use of oral contraceptives has long been associated with cardiovascular morbidities such as hypertension and myocardial infarction.13,14 Norplant is progestogen-only hormonal contraceptive implant with a novel delivery system. Two main findings have emanated from this study. First, QRS intervals that we have earlier reported to be prolonged after 12 months of Norplant implant contraception15 remain prolonged after 3 years of use. The QRS interval, a measure of the time taken to depolarise the cardiac ventricles, is prolonged in diseases affecting the bundle of His and the Purkinje network. This situation is referred to as bundle branch block. Apart from a small proportion of subjects in whom it may pass for normal, ischaemic heart disease and myocardial infarction intervals of 0.16 seconds are causes in most instances.16 The interval is normally less than 0.10 seconds. Although in this study, the mean QRS intervals remained within the normal range throughout the 3-year period of follow up, they were significantly longer than at pre-insertion (Table 1 and 2). The persistence of this change as innocuous as it seem, raises the need for continued surveillance of Norplant® users and portends danger for clients with cardiovascular disease, who should be offered alternative methods of contraception. The PR interval which is an index of conduction status particularly at the atrioventricular (AV) node17 increased significantly at 3, 6, and 12 months15 but returned to pre-insertion levels by the 36month visit. However, despite the increase from levels at pre-insertion, the mean PR interval was well within normal limits of 0.12 to 0.20 seconds all through the study period. Norplant implant after 3 years of use cannot therefore be said to cause first degree heart block, the clinical condition of prolonged PR interval. The second main finding in this study is the statistically significant weight gain by clients after 2 years of Norplant insertion. A widely held myth suggests that oral contraceptives cause weight gain and for this reason, many women stop using oral contraceptives early or never even start using them. A review published in the latest issue of the Cochrane Library18 examined the information on weight changes in 44 randomised controlled hormonal contraceptive trials and overall, there was no association between oral contraceptive use and weight gain. Randomised controlled trials are the ‘gold standard’ of trial designs for reducing the potential for bias. Some women gain weight over time regardless of whether they use contraception. The present study did not examine nonusers of hormonal contraception over time as controls. There is a tendency to prolongation of PR and QRS (ECG) intervals in Norplant users; accordingly, it may be prudent for clients with cardiac conditions showing longer ECG intervals, to consider alternative methods of contraception. Acknowledgement The authors wish to thank all the clients who participated in this study. We are also grateful to the staff of the family planning clinic and the ECG unit of JUTH for their cooperation and assistance during the study period. The assistance received from the Nurses and Doctors who participated in the Norplant® training programme is also appreciated. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08007t1b.jpg] [rh08007t2.jpg] [rh08007f1.jpg] [rh08007f2.jpg] [rh08007t3a.jpg] [rh08007t3b.jpg] [rh08007f3b.jpg] [rh08007t1a.jpg] [rh08007f3a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}