 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
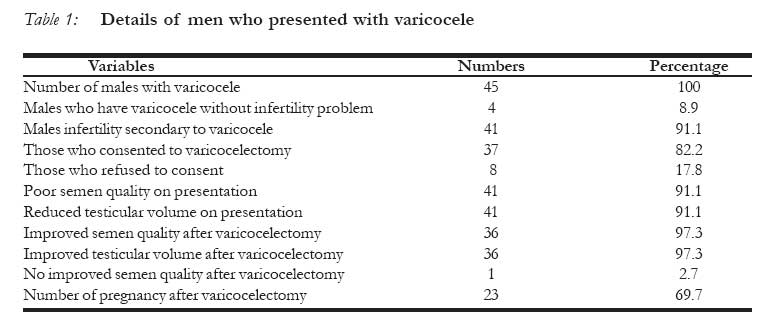
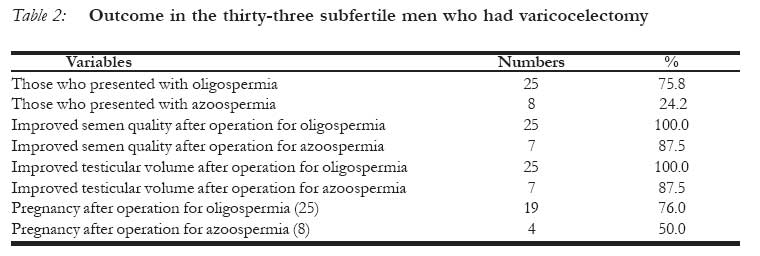
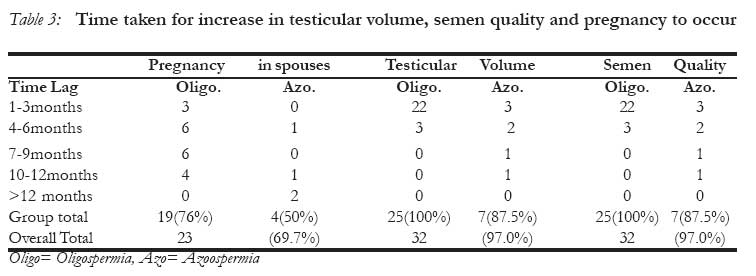
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 54-59 Male Infertility Secondary to Varicocele: A Study of the Management of 45 Patients Stérilité masculine secondaire à la varicocèle : une étude du traitement des 45 patients Osifo O.D 1 Agbugui J.O 2 Affiliation: Paediatric Surgery Unit1 And Urology Unit2 Department of Surgery, University of Benin Teaching Hospital, Benin City- Nigeria. Code Number: rh08008 ABSTRACT Varicocele is a common condition worldwide. The aim of this five-year prospective study is to examine the effect of varicocelectomy on the fertility profile of affected men in a male infertility clinic in Benin City, Edo State. A total of 45 men aged 16-65 years were diagnosed with varicocele during the period. Forty one (91.1%) had infertility while 4 (8.9%) were unmarried boys with third degree varicocele. Thirty seven (82.2%) consented to varicocelectomy; thirty three had infertility. Varicocelectomy was done through an open subinguinal approach. Restored testicular volume and semen quality were achieved within the first 12 months in all but one. Among the 33 men who had infertility, the spouses of 23 (69.7%) achieved pregnancy during the period of follow-up after varicocelectomy while the spouses of 10 (30.3%) had not. No major complication was recorded after operation. It is recommended that in subtropical Africa where there are no facilities for microscopic varicocelectomy and embolization, open varicocelectomy should be used. It is safe, effective and has much to offer. KEY WORDS: Varicocele, male Infertility, Varicocelectomy, Pregnancy RÉSUMÉ La varicocèle est un état pathologique commune partout dans le monde. Cette étude perspective de cinq ans a pour but d’examiner l’effet de la varicoceletomie sur le profil de la fécondité des hommes affectés, dans une clinique pour le traitement de la stérilité masculine à Bénin City, Etat d’ Edo. Au total 45 hommes âgés de 16 – 65 ont été diagnostiqué comme étant affectés par la varicocèle au cours de la période. Quarante et un (91,1%) étaient stériles alors que 4 (8,9%) étaient des garçons célibataires qui étaient touchés de varicocèle de troisième degré. Trente-sept (82,2%) ont accepté la varicocelectomie à travers une approche de sous-inquinal ouvert. La restauration du volume testiculaire et la qualité du sperme ont été accomplies au cours des douze premiers mois chez tous à l’exception d’un. Parmi les 33 hommes qui étaient stériles, les épouses des 23 (69,7%) étaient devenues enceintes au cours de la période de l’observation post-thérapeutique alors que les épouses de 10 (30,3%) n’étaient pas devenues enceintes. Il n’y a eu aucune complication importante après l’opération. Nous préconisons qu’en Afrique subtropicale où les facilités ne sont pas disponibles peur faire une varicocelectomie microscopique et l’embolisation, on utilise la varicocelectomie ouverte. Elle n’est pas dangereuse, elle est effective et promet beaucoup. Introduction Varicocele is the dilatation, elongation and tortuosity of the pampiniform plexus due to venous stasis. It is more common on the left than right because the left testicular vein enters the left renal vein at right angle. The erect posture of man, obstruction by left renal artery, prolong venous congestion due to unrelieved sexual excitement and obstruction by tumours are some other implicated aetiological factors 1. Varicocele is quite common and is said to affect 8-22% male in the general population but rises to 21-39% in men attending infertility clinic2,3. Unrelieved venous stasis interferes with testicular temperature regulation which is usually maintained at 2-3ºC less than core body temperature4. Continuous exposure to high temperature causes subfertility by decreasing testicular volume, spermatogenesis, semen quality and an increase in immature sperm in the ejaculate 1. The surgical treatment is varicocelectomy which involves ligation of testicular veins. Access to the veins can be gained through subinguinal, transinguinal or suprainguinal incision. This operation can be done either by open, laparoscopic, microscopic or embolization unilaterally or bilaterally5-7. The effect of varicocelectomy on male fertility is contentious.4,8,9. Earlier studies on the use of varicocelectomy for the treatment of varicocele induced infertility indicated a remarkable improvement in fertility profile8,9. Fowler4 is, however, of the opinion that there is little evidence to show that varicocelec-tomy improves semen quality or conception rate. Reasons for these varied opinions on the effectiveness of varicocelectomy are not clear. The purpose of this 5-year prospective study done between January, 2001 and December, 2005 is to evaluate the effectiveness of varicocelectomy in the treatment of male infertility due to varicocele. PATIENTS AND METHOD Study Area This is a five-year prospective study done at Leadeks Medical Centre in Evbuomore community between January, 2001 and December, 2005. The community is located along Benin-Lagos expressway in Ovia North-East local government Area, about two kilometers from University of Benin Teaching Hospital, Benin City, Edo State, Nigeria. The community is suburban with a population of approximately 600,000. There are five private health institutions which serve the people. Patients were referred to our facility from these institutions while a large number of them presented to us directly. Advocacy/Ethical considerations The patients who were diagnosed to have varicocele were adequately counselled for varicocelectomy and the subsequent follow up. Only those who gave consent for operation and willingly filled the administered questionnaire were enlisted for the study. Method All the men who presented themselves in the male infertility unit at the Centre during the period had semen analysis and were studied using a standardized questionnaire that contained data such as age, year of marriage, use of hormonal drugs, primary or secondary infertility, testicular volume, azoospermia, oligospermia and infertility problem in the spouses. Thereafter those who had varicocele were counselled for varicocelectomy. Those whose infertility were not due to varicocele and those who refused to give consent for varicocelectomy (n=18) were excluded from the study. Testicular volume was assessed by digital palpation (no facility for punched-out orchidometer). Azoospermia was defined as absence of spermatozoa in the semen, oligospermia as a count less than 20million/ml, (asthenospermia as motility less than 50%, teratospermia as abnormal morphology more than 50% and necrospermia as dead spermatozoa). The above data recorded in the questionnaire pre-operatively were used as baseline. The patients were assessed at 3-monthly interval for 2 years after the operation and the time taken for improvement in pre-operative parameters and pregnancy to occur were recorded. The data was analyzed using SPSS and presented as count, frequency and percentage. Results Fifty-five men were seen in the clinic during the period for suspected varicocele out of which ten were excluded because of lack of clinical and laboratory evidence of varicocele. The remaining forty-five had various grades of varicocele and were studied. The results of semen analysis on presentation showed poor semen quality in fortyone (91.1%). All those with varicocele also had reduced testicular volume. Eight (17.8%) refused to consent, while thirty-seven (82.2%) consented and had varicocelectomy. Thirty-three (89.2%) varicocelectomy were for infertility and four (10.8%) for third degree varicocele in unmarried boys. Thirty-six (97.3%) after varicocelectomy had improved testicular volume and semen quality while one (2.7%) had not during the period of follow-up. The spouses of twenty-three (69.7%) who had varicocelectomy for infertility achieved pregnancy after operation, while ten (30.3%) could not because their spouses were also being treated for infertility (Table 1). Two patients (5.4%) developed vaginal hydrocele during follow-up after operation. The patients were aged 16 and 65 years (mean 37 ± 7.4years). The highest numbers were those aged 31 and 40 years (67.7%). A detailed analysis of the thirty-three men who had infertility, revealed that they were married for between 1 and 18 years. Twenty-five had primary and eight had secondary infertility. Thirty two (97.0%) of them were aware they had abnormal semen quality while only 30.3% of them knew the cause was varicocele. Hormonal drugs were used by 81.8% without benefit, whereas 6.1% had deterioration in semen quality after prolonged usage. Pre-operatively, twenty-five (75.8%) had oligospermia and all of them achieved normal testicular volume and semen quality after operation (100% success), while the eight (24.2%) of them in azoospermia group recorded 87.5% success (Table2). Pregnancy was achieved by the spouses of 76.0% of those who recovered in oligospermia group and 50% of those in azoospermia group. Table 3 depicts the increase in semen quality which occurred simultaneously with the increase in testicular volume. Maximum increments were recorded during the first 3 months and remained steady thereafter. The highest number of pregnancy took place during the first 6 months, and taper down until the end of the 2-year follow up. Discussion The results of this study indicate that varicocelectomy improves testicular volume and semen quality. This resulted in higher chances of pregnancy among the spouses of men who were subfertile prior to varicocelectomy. Varicocele has been reported to be very common especially among men attending infertility clinic2,3 accounting for 81.8% in this series. The incidence appears low in this subregion perhaps due to lack of awareness because only 30.3% of those who had varicocele in this study were aware of it before presentation. Unrelieved venous stasis culminates in decrease testicular volume and poor semen quality 1 as recorded in all the patients. When neglected, the testes become atrophic with absence of spermatozoa in the seminal fluid (azoospermia)2. This was seen in 24.2% and oligospermia seen in 75.8% of the thirty-three subfertile men. The onset of symptoms and subsequent presentation to the health facility were mainly in the middle age, with a peak among those aged marriage before presentation in this series was 31 and 40 years. Although many patients present between 1 and 18 years. Those who had within the reproductive age group,6-10 varicocele secondary infertility were most reluctant. The eight may also affect children as seen in this study. Many patients in this category delayed most in this study.patients did not present early as was also The diagnosis of varicocele is mainly clinical, highlighted in previous reports11,12. The length of although the use of sophisticated facility such as Doppler ultrasound scan enhances accuracy especially for the subclinical types13. Digital palpation with patient in standing position and Valsalva’s maneuver were used to diagnose all the cases1, 4. Even in the absence of orchidometer, a careful digital palpation can detect reduced testicular volume as was done in our study and others8,9. Combining these with seminal fluid analysis almost always confirm the diagnosis, testicular biopsy being added if doubt still persists14, 15. Varicocele has been considered the most costeffective treatable cause of male infertility 3. The standard treatment is varicocelectomy which involves ligation of testicular veins. There are divergent views in the literatures1-21 as to whether the testicular artery should be preserved or not, whether the infra, trans or suprainguinal approach is the best and whether unilateral or bilateral ligations should be done. We, however, did bilateral subinguinal ligation of both vessels without complication, except two who developed vaginal hydrocele during follow-up. This tallies with what occurs in the most selective microscopic ligation as reported by Al-kandari et al 5 in a comparative study on all the types of varicocelectomy. There is unanimous opinion in the literatures5-21, however, that the use of hormonal drugs such as mesterolone (proviron) to improve semen quality in varicocele patients do not have effect and infact can lead to deterioration in semen quality after prolonged usage as seen in our series. Irrespective of the method of ligation there is rapid improvement in testicular volume and semen parameters1-3, 5-21. These became noticeable during the first 6 months after operation in this report. Neither the age nor azoospermia should preclude a patient from being offered varicocelectomy. All our patients but one recovered after operation as also recorded in similar reports 12,20. Pregnancy should occur as semen quality improves but causes of infertility in spouses reduced the chance to 69.7% pregnancies as against 97.0% restoration in semen quality 2,6,21. There is, therefore, a need to encourage both couple to seek early medical attention so that gynaecological problems in the spouses can be handled by a Gynaecologist simultaneously. Conclussion This prospective study evaluated the outcome of varicocelectomy for the management of thirtyseven among the forty-five men who presented with varicocele. Semen quality and testicular volume increased considerably in the patients, and pregnancy was achieved in a good proportion of the spouses of men who had varicocelectomy for infertility. Open infrainguinal, transinguinal or suprainguinal ligation is satisfactory and this has much to offer in this subregion where there are no facilities for microsurgical varicocelectomy. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08008t1.jpg] [rh08008t3.jpg] [rh08008t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}