 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 67-73 Prevalence of Low Sperm Count and Abnormal Semen Parameters in Male Partners of Women Consulting at Infertility Clinic in Abakaliki, Nigeria Prévalence du paludisme au moment de se présenter pour la première fois chez les clientes anténatales dans un établissement de santé secondaire à Ibadan, Nigeria *Ugwuja EI1, Ugwu NC1 and Ejikeme BN2 1Department of Chemical Pathology, Faculty of Clinical Medicine, Ebonyi State University, P.M.B. 053, Abakaliki, Nigeria. Code Number: rh08010 ABSTRACT In order to provide an insight to the prevalence of low sperm count and abnormal semen parameters in suspected subfertile/infertile men in our environment, semen samples collected from one hundred and seventy (170) men aged 21-50 years, whose wives were seen at a private fertility clinic in Abakaliki, Nigeria with diagnosis of primary and secondary infertility (78 and 92 respectively) were analysed in accordance with World Health Organization guidelines. Significantly high proportion (70%) of the study population had low sperm count (p < 0.05) with significantly high defective parameters (64%). Asthenozoospermia and teratozoospermia were the major abnormal parameters recorded. Higher prevalence of oligospermia was found in the civil servants and age-group 31-40 years (74% and 75% respectively). Using 105 cfu/ml as a significant level of bacteria growth, the prevalence of bacteria growth was found to be 56% of which 18% were from normospermic semen d 38% from oligospermic semen. KEY WORDS: Abnormal semen parameters, male partners, genital infection, infertility. RÉSUMÉ La prévalence de la parasitémie du paludisme au moment de se présenter pour la première fois a été étudiée chez 1,848 femmes enceintes dans un hôpital secondaire à Ibadan, Nigeria. Les principales issues variables étaient la parasitémie persistante et la fièvre 8,4% (155) avaient la parasitémie du paludisme persistant. La majorité (89%) des participantes qui avaient la parasitémie étaient asymptomatiques. Les participantes fébriles se sont inscrites à un âge gestationnel plus tôt (22,7 par opposition à 24, 2 semaines) plus que les patientes afébriles (p = 0,0052). L’anémie était plus prévalente parmi les patientes qui avaient la parasitémie persistante (58,1%) que chez celle qui n’en avaient pas (58,1% par opposition à 22,6% p < 0,0001). La parasitémie du paludisme était plus élevée chez les femmes nullipares que chez les autres groupes de parité (p < 0, 0001). La prévalence de la parasitemie du paludisme dans cette étude est beaucoup plus basse que dans les rapports précédents. Le paludisme symptomatique a été lié à l’inscription faite tôt pout l’hygiène de la grossesse et la parasitémie du paludisme était un déterminent important de l’anémie. Introduction Infertility of couples affects 19% of the general population. The problem of infertility of pathological origin is so high in sub-Saharan Africa that it has become a public health problem 1. The prevalent rate varies from one region to the other 2. In America, it is estimated that about six million (10% of the reproductive age population) couples are infertile. In rural Nigerian community, an overall prevalence of 30% was reported, of which 9.2% and 21.1% represent primary and secondary infertility respectively3. In a similar study in southestern Nigeria, 65% and 35% prevalent rate were reported for primary and secondary infertility respectively4. While genital infections (post-abortal and puerperal) have been identified as the major contributory factors for high prevalent rate of infertility in females4, oligospermia and asthenozoospermia were common aetiological factors responsible for male infertility3. Although conventional semen analysis has been criticized as not a true test of sperm function based on its poor prediction of fertility when compared to more sophisticated tests such as sperm penetration, capacitation, acrosome reaction and, more recently, by sperm chromatin structure assay (SCSA) for the detection of DNA integrity 5, it remains the single most useful and fundamental investigation in the assessment of male6 as all clues to whatever problem (hormonal or structural) of infertility are found within the semen. Semen parameters (e.g., appearance, volume, pH, motility, morphology, viability, concentration, liquefaction and presence of wbc or/rbc) have been found to be important determinant of functional competence of the spermatozoa 7,8. Increased sperm abnormalities have been suggested as a possible cause of decreased fertility in men, yet the incidence is not known in men with suspected sub-fertility/ infertility in Abakaliki. This study aims to document the prevalence of low sperm count and abnormal semen parameters in male partners of women consulting at fertility clinic in Abakaliki, Nigeria. Materials and Methods Subjects: One hundred and seventy (170) consecutively consenting male partners of women attending fertility clinic (age range, 21-50 years) whose wives were seen by gynaecologists at a private specialist Hospital in Abakaliki, Ebonyi State, Nigeria between October 2004 and May 2006 were recruited for enrolment in the study. These men were referred for semen analysis with diagnosis of primary and secondary infertility (78 and 92 respectively). Those excluded from the study were those who found method of sample collection inconvenient, or on antibiotic prophylaxis and those who did not consent or/ withdrew their consent. Sample collection: Sociodemographic data such as age of couples, occupation, duration of involuntary childlessness, and obstetric history were obtained by structured questionnaire. Instructions on how to collect acceptable samples were given as follows:
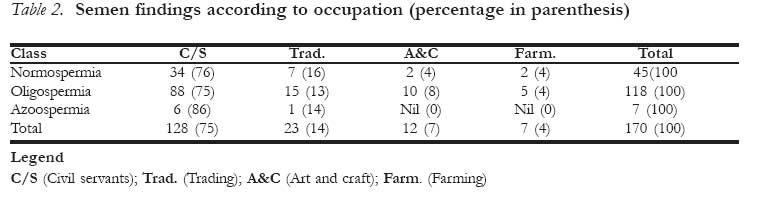
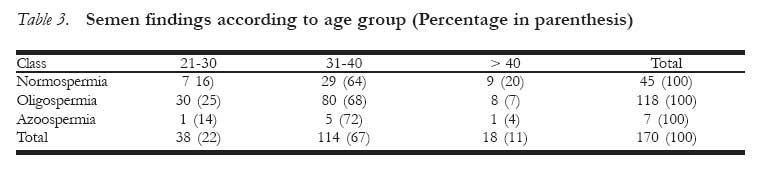
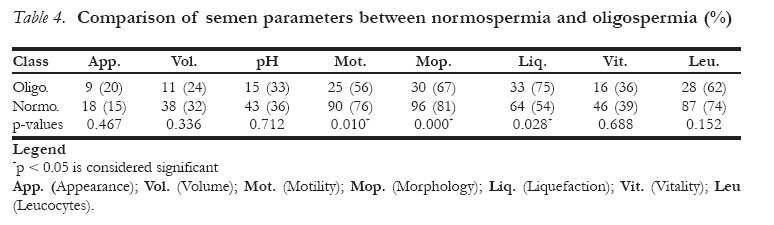
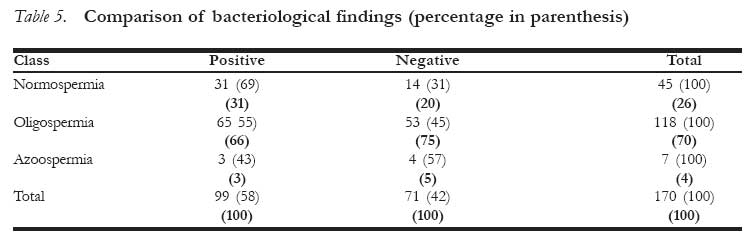
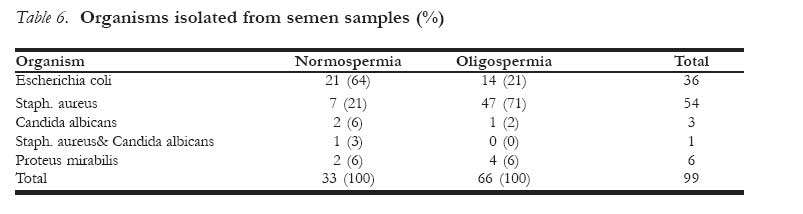
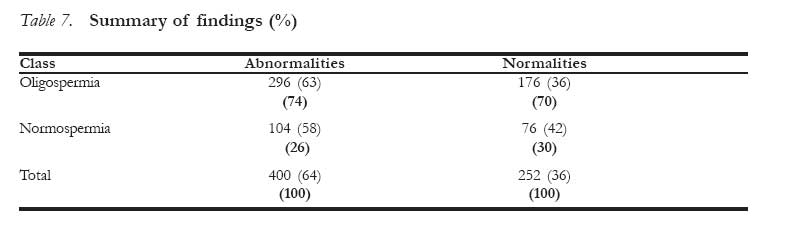
All samples were collected into sterile screw capped plastic universal containers. Two samples were collected from each patient at 3-4 weeks interval. Sample analysis: The samples were analysed at Unic Biomedical Laboratories, No 8 Ukwansi Street Abakaliki, Ebonyi State and Department of Chemical Pathology, Ebonyi State University, Abakaliki, Nigeria. The entire sample analyses were done by the same Medical Laboratory Scientist to avoid inter-laboratory variation. Semen analysis was done in accordance with WHO guidelines9. Semen was examined within 60 minutes of their collection for volume, appearance, pH, liquefaction, concentration, motility, morphology, viability, and the presence of wbc/rbc. Results from two analyses were compared and the mean determined for quantitative parameters. For the purpose of this study, semen was classified based on sperm count per millilitre (count/ml) of semen in accordance with WHO normal and pathological ranges. Bacteriological study was carried out as in a standard microbiology textbook 10. Semen was inoculated after complete liquefaction on blood and chocolate agar using calibrated (0.001ml) platinum loop. The plates were incubated at 370C for 24-48 hours and examined for the evidence of growth. Growth was regarded significant in the presence of 105cfu/ml. Samples were regarded contaminated if more than two organisms isolated. All positive samples were subcultured and the organisms appropriately identified by biochemical tests 10. Data Analysis The data generated was analysed using EPI-INFO 6.2 Statistical package. Data were analysed for mean and Chi-square (X2) with level of significant set at less than 0.05 (p < 0.05). Results The women aged 18-40 years were ovulating based on obstetric history from case files. The duration of involuntary childlessness ranged between 2-5 years (median, 4 years). Out of the one hundred and seventy (170) semen samples analysed, 45 (26%) were normospermic and 118 (70%) oligospermic while 7 (4%) were azoospermic (Table 1). Table 2 shows the distribution of semen findings according to occupations, with highest abnormalities (oligospermia and azoospermia) found among the civil servants (75% and 86% respectively) and the least in the farmers (4%). Table 3 compares semen findings according to age group. The age group 31-40 years had the highest abnormalities (68% and 72%) for oligospermia and azoospermia respectively, and the lowest abnormalities were found in older age groups (7% and 14% for oligo- and azoospermia). Interestingly, 30 (25%) of the semen from 21-30 years age group were abnormal (oligospermic). Table 4 compares the abnormal parameters in normospermia and oligospermia. The oligospermia has statistically significant higher abnormal motility (76% vs. 56%, p = 0.01) and morphology (81% vs. 67%, p = 0.01), than the normospermia. However, the normospermic semen has significantly higher abnormal liquefaction (75% vs. 54%, p = 0.02) than the oligospermia. Although there were higher abnormalities in volume (32% vs. 24%), appearance (20% vs. 15%), pH (36% vs. 33%, vitality (39% vs. 36%) and wbc (74% vs. 62%) in the oligospermia than the normospermia, these were not statistically significant (p > 0.05). None of the samples had the growth of more than two organisms. According to Table 5, pathogenic organisms were isolated from 99 (56%) samples of which 68 (38%) were from oligospermia and 31 (18%) were from normospermia respectively, however, the difference was not statistically significant (69% vs. 55%, p > 0.05). While Staphylococcus aureus was the major organism isolated from oligospermic semen, Escherichia coli was the most frequent organism pathogen in normospermic semen (47% and 21% respectively). Other organisms isolated include Candida albicans and Proteus mirabilis. Candida albicans and Staphylococcus aureus were isolated from one semen sample (Table 6). In general, oligospermic semen has 296 (63%) abnormalities against 104 (58%) in normospermic semen. However, the difference was not statistically significant (p > 0.05). In both the normo- and oligospermic semen, abnormal parameters were the major findings with 400 (64%) abnormalities recorded against 252 (36%) normalities (Table 7). Discussion The high incidence (70%) of oligospermia in the present study corroborates earlier report 3, which identified oligospermia/azoospermia as the major contributory factors in sub-fertile/infertile Nigerian couples. Other causes of male infertility include, (1) abnormalities of spermatozoa which may be pre- testicular (hormonal), testicular (chromosomal), or post-testicular (disorder in sperm transportation), (2) abnormalities in seminal plasma (infection, auto- or isoimmunisation), (3) abnormalities of ejaculation (pathogenic or iatrogenic retrograde ejaculation) and (4) unknown cause11. Among our patients 26% had normal sperm count. The implication of this is that the infertility in these couples may not be associated with low sperm count, but rather defective semen parameters or other aetiological factors such as environment or female factor. However, it could not be established if female factor was responsible as evaluation of female partners to determine their contribution was not in the original design of this study. This would be an interesting area to explore in future studies. Environmental factors such as heat, chemical and lifestyle including diet, frequency of intercourse, smoking and alcohol are known to have adverse effects on sperm parameters5,12. Other causes of semen abnormalities are stress (emotional and physical), insomnia, tight brief, and hot tubs e.t.c. More semen abnormalities identified in civil servants than other professionals in this study are curious, as no association has been found between semen qualities and occupation13. Although there was no history of occupational exposure of our patients to environmental factors that can adversely affect semen quality and quantity, the high prevalence of abnormal semen in civil servants could be explained away, considering the fact that they are elite group who are socially active and could be involved in some social activities such as smoking, excessive alcohol consumption e.t.c that may interfere with semen qualities. Nonetheless, the present study show that genital infections seem to be the most appropriate explanation for the high incidence of abnormal semen parameters as evidenced by high leucocytospermia and bacteria infections in both the normospermic and oligospermic semen (69% and 55% respectively). While the relationship is yet to be found between the types of bacteria infection and sperm count, the inhibiting effect of some bacteria (e.g. Escherichia coli) on spermatozoa has been demonstrated14. Although leucocytospermia appears to be of little prognostic value with regards to male fertilizing potential15, it has been found that percentage sperm motility is significantly and negatively correlated with leucocyte concentration in semen and represents an essential or an additional risk factor for decreased sperm functional competence16,17. Inflammation due to infection of accessory glands either by functional impairment and/or partial occlusion of seminal tract may be responsible for the high prevalence of oligospermia in this study8. Another possibility is that higher proportions of our patients were civil servants. The reason for this high turnout is not far fetched. Civil servants in addition to being aware of the possible potential role of male factor in fertility problem are financially empowered to seek medical intervention. This ha implication for resource limited countries like Nigeria where the literate level is very low with majority living below poverty line. The negative influence of illiteracy and poverty is demonstrated by the low turn out in other professions in seeking medical care for their fertility problem. The lack of specific pattern of sperm abnormalities among the age groups is in accord with previous studies 11,18, which did not show evidence of sperm deterioration with aging. However, it contrasts the age-dependent decline in sperm qualities reported by other researchers 19-21. It is not surprising that higher percentage (68%) of semen abnormalities were found in the age group 31-40 years, because this represents the active reproductive age group who may be harbouring residual infections acquired prior to marital life. The significantly higher incidence of asthenozoospermia and teratozoospermia in oligospermic semen than the normospermia also corroborates previous study elsewhere 22, where the incidence of defective spermatozoa were highest in semen with the lowest sperm count. Although there was no significant difference in the bacteriological findings between the oligospermia and normospermia, infection was generally high in the former than the latter. In conclusion, male partners of women consulting at infertility clinic in Abakaliki have high prevalence of low sperm count and abnormal semen parameters, which is associated with bacteria infections. In addition to suspected infertile men, annual semen analysis is advocated for adult residents above the age of twenty (20) years and those identified with abnormal semen be appropriately evaluated and treated. Acknowledgement We are grateful to the management of Unic Biomedical Laboratories for allowing us to use their facilities. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08010t2.jpg] [rh08010t6.jpg] [rh08010t7.jpg] [rh08010t5.jpg] [rh08010t4.jpg] [rh08010t3.jpg] [rh08010t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}