 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
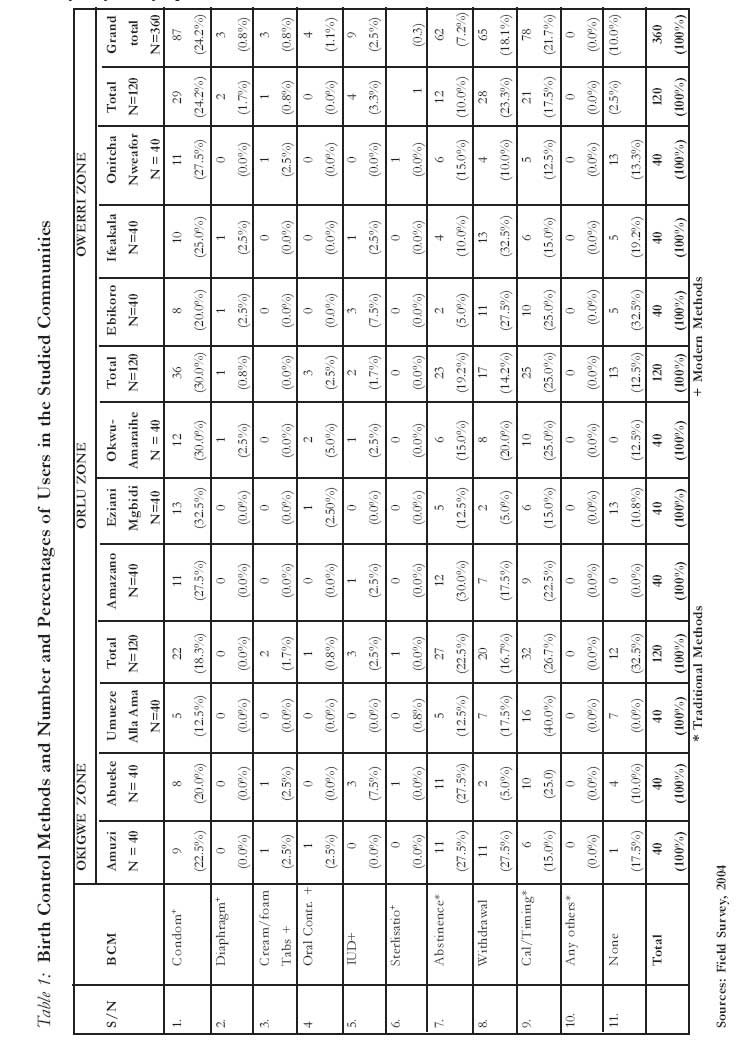
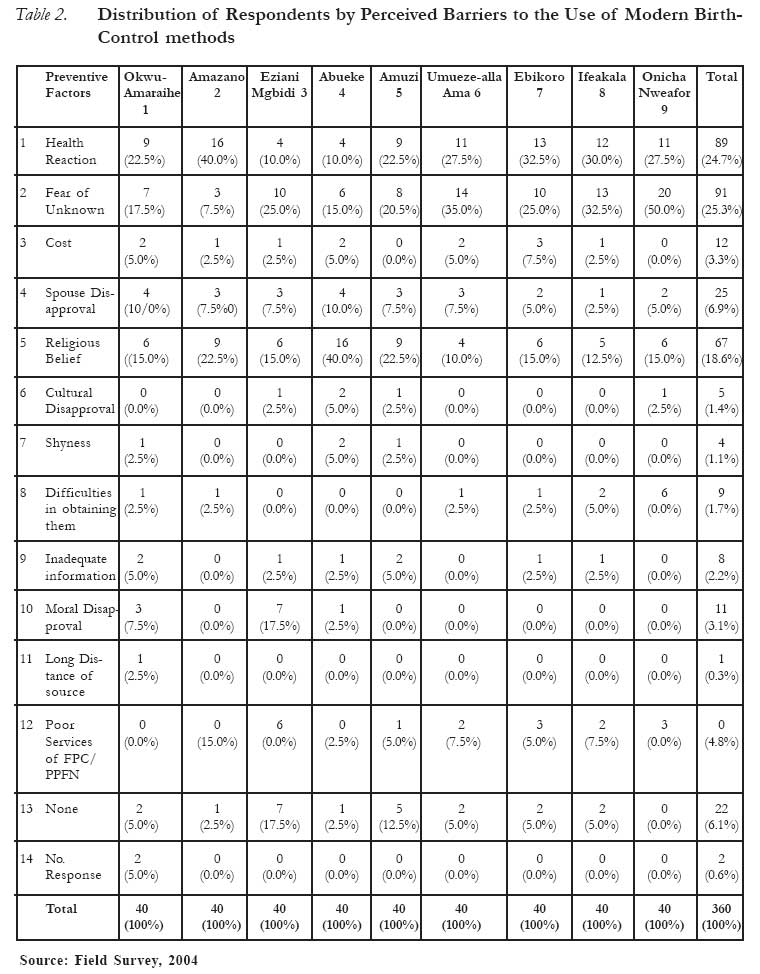
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 101-108 Use of Modern Birth Control Methods Among Rural Communities in Imo State, Nigeria L’utilisation des méthodes modernes de contrôle des naissances au sein des communautés rurales dans l’état d’Imo, Nigéria Ike Nwachukwu and O.O. Obasi Nwachukwu, IKE Ph.D Nwachukwu, IKE Ph.D Michael Okpara University of Agriculture Umudike, Nigeria nwaike3@yahoo.com OBASI, O.O. Ph.D Federal Polytechnic Nekede, Nigeria Code Number: rh08015 ABSTRACT This paper studied the extent of utilization of Modern Birth Control Methods (MBCM) among rural dwellers in Imo State Nigeria. Three hundred and sixty households were randomly selected and data were obtained from them with the use of questionnaires and Focus Group Discussion. The results showed that only 30% of the respondents used MBCM while 57% of them used the traditional birth control methods. The most popular modern method was the condom (24.2%). This was followed by the IUD, used by only 2.5% of the respondents. Some of the identified factors that hindered the use of MBCM included perceived negative health reaction, fear of the unknown effects, cost, spouse’s disapproval, religious belief and inadequate information. For a better understanding and utilization of MBCM, it is recommended that adequate educational campaign should be mounted in the rural areas on the advantages of MBCM. This campaign should target the men the more because they make the major decisions on MBCM use. KEY WORDS: Birth control. Rural communities. Utilization. Methods RÉSUMÉ L’article a étudié l’ampleur de l’utilisation des méthodes modernes de contrôle des naissances (MMCN) au sein des villageois dans l’Etat d’Imo, Nigeria. Trois-cent-soixante familles ont été sélectionnées au hasard et des données ont été obtenues à l’aide des questionnaires et des Discussions en Groupes Cible. Les résultats ont montré que seuls 30% des gens interroges utilisaient les MMCN alors que 57% d’eux utilisaient les méthodes traditionnelles de contrôle des naissances. La méthode moderne la plus populaire était le préservatif (24,2%). Le DIU venait après, utilisé par seuls 2,5% des personnes interrogées. Quelques facteurs identifies qui ont entravé l’utilisation des MMCN ont compris une réaction médicale négative perçue, la crainte des effets inconnus, le coût, la désapprobation de l’époux, la croyance religieuse et l’information insuffisante. Pour une meilleure compréhension et utilisation des MMCN, nous proposons qu’une campagne éducative adéquate soit montée dans les régions rurales sur les avantages des MMCN. Cette campagne devrait avoir comme cibles les hommes plus que les femmes parce qu’ils prennent les décisions principales sur l’utilisation des MMCN. Introduction The population of any society depends primarily on its territory or physical environment for sustenance. Most of its food and other needs largely derive directly or indirectly from the environment, which consists essentially of land and its derivatives. Unfortunately, while populations of nations increase overtime, the various land masses on which these populations depend for sustenance are relatively fixed. Herein lays the general concern about population size and growth rate. However, the key to understanding over population is not population density, but the number of people in an area relative to its resources and the capacity of the environment to sustain human activities 1 It was Malthus 2 who first raised the alarm that a stage would reach in the world population when food supply would not match population growth. Many authors have since reiterated the concern of Malthus 3, 4, 5. While the developed countries have managed to overcome the Malthusian prophecy, the same is being fulfilled in developing countries. In Africa, the problem of food shortage in feeding the population is overwhelming 6, 7. The end result of this food shortage is associated with social problems ranging from poverty, scarcity of land, hunger and environmental degradation, to political and social instability8, 9, 10, 11 . Nigeria, with a population of 140 million 12 has become the largest country in Africa in terms of population. According to Khurfeld 13, Nigeria is already facing a population explosion. The result of the population explosion is that food production cannot match the growing population, and there is inadequate water supply. In Nigeria today, the birth rates are higher than the world averages. (Encyclopedia Britannica). Many developing countries like Korea, Brazil, Columbia, China, India and Bangladesh have successfully applied family planning programs as a panacea for overpopulation14, 15. Nigeria has also adopted family planning as a strategy to curb the high rate of population growth that it is presently experiencing. However, the adoption rate of the family planning method is still low 16, 17 About 70% of Nigeria’s population live and work in the rural communities with a very high fertility rate 18. The introduction and acceptance of Modern Birth Control Methods (MBCM) are of great importance in controlling the population growth in Nigeria. Reports from Federal Office of Statistics (FOS) 19 indicated that the adoption of MBCM rose from 1% in 1981 to 11% in 1994 and declined to 7.1% in 1995. Another report in 1998 indicated that only 5.1% of all women in the country were using family planning methods 20. This low adoption rate of MBCM has been variously reported21- 24. Adopting MBCM is a very complex sociological issue in Africa. Johnson-Hanks 25 indicated that African women draw on a complex social repertoire in making contraceptive choices. This does not depend on modern or traditional methods. Indeed, there are many other aspects of the use of MBCM apart from population control. As has been pointed out by UNFPA26, about 201 million women around the world do not have access to effective Family Planning Methods. Meeting their needs would prevent 23 million unplanned births, 22 million abortions, 1.4 infant deaths, 142,000 pregnancy related deaths and 505,000 children losing their mothers due to pregnancy related deaths. There is therefore the need to continuously research into this issue with the view to finding the best method of increasing the use of MBCM among the adult population, especially in the rural areas where the majority of Nigerian live but lack the basic facilities. The objective of this paper is to determine the level of use of MBCM among rural communities and identify the factors affecting their use in Imo State, Nigeria. Methodology Nigeria is a Federation of 36 states, and the capital territory of Abuja. These states are divided into six geo-political zones of North East, North West, Middle Belt, South East, South West and South South. This study was conducted in 2005 Imo State which is one the nine states in the Eastern part of Nigeria. The state with a population of 3 million is made up of twenty-seven Local Government Areas (LGA) and divided into 3 zones of Okigwe, Orlu, and Owerri. From each of the three agricultural zones of the state, three communities were randomly selected from nine LGAs. From each of the nine communities, 40 households were randomly selected. Therefore, 360 households were involved in the study. The village heads provided the names of households; these names were written on little pieces of papers and put in a bag, from where 40 were drawn. Though the communities were not of equal population, but the same size of respondents were drawn from each community. This was not expected to affect the results because of the homogeneous nature of the communities. Data were collected with the use of questionnaire and Focus-Group Discussions (FGD). For data collection, the household heads were selected for interview. This was determined in two ways. Where the husband and wife were present, they both decided who responded to the interview. Second, where one of the spouses was not present, the one present responded to the questions. For the FGD, a community was selected from each of the three zones. In each community, four couples were randomly selected for discussion. The result of the FGD provided more insight to the and validated the responses from the interview. The data generated were descriptively analyzed. Modern birth-control methods were defined as the scientific and artificial measures and devices used to prevent unwanted pregnancies. These included condom, diaphragm, cream/foam tablets, oral contraceptives, IUD, injectables, sterilization. Use of MBCM was defined as the acceptance and continual use of the methods as at the time of the study. It was simply measured in terms of whether or not a respondent was using or had adopted the method(s) to prevent unwanted pregnancies or limit their number of children. Based on this, the respondents were grouped into two categories of users and non-users of MBCM. Results and Discussion Socio-economic characteristics of respondents Out of the total sample of 360 respondents, 45% were males, while 55% were females. Two-third of them was married and a vast majority of them were educated (i.e. had post primary education). All the respondents were religiously inclined with 67% of them as Catholics and the rest, Protestants. A majority of them were between 40 and 49 years of age while the average annual income was N120, 000 ($857). The average family size was 6.8. Almost all the respondents were aware of one type of MBCM or the other Use of Modern Birth-Control Methods The modern birth control methods studied were the use of condom, diaphragm, vaginal cream/ foaming tablets, oral contraceptives or pills, Intrauterine Device (IUD), inplant, injectables and sterilization. Results from Table 1 showed that only 29.7% of the respondents were using modern methods. The most popular method (used by 24.2% of the respondents) was the condom. This was followed by the IUD, used by only 2.5% of those using the modern method. Oral contraceptives were used by only 1.1% of them. Other modern methods did not have significant usage by respondents. In contrast to the use of modern birth control methods, the majority of the respondents (57%) used the traditional birth control methods, while 13.3% of the respondents did not use any form of birth control methods. For the traditional birth control methods used, abstinence was used by 17.2% of the respondents. Here, couples abstained from sex for the period they want to avoid pregnancy. Usually, during the period of abstinence, the husband had other spouses to continue sexual relationship with. Other methods used were, timing, which was the most popular method used (21.7%). Withdrawal method was used by 18% of them and prolonged breastfeeding (14.4%). What has emerged from these results is that first, the level of modern birth control usage was very low in the communities studied. There was however, a concomitant high rate of traditional birth control usage, in spite of their high failure rates. The low usage of condom by communities was likely to increase the spread of HIV/AIDS in such communities. The most interesting part of the findings was the fact that 80% of those who used the modern birth control methods were men. This is interesting because the vast majority of this methods target the women audience. Perceived Barriers to the Use of Modern Birth Control The study also found out the factors that militated against the use of modern birth-control methods in the communities. Table 2 indicates twelve barriers mentioned by the respondents, and these included health reaction, fear of the unknown effects, cost, spouse’s disapproval, religious belief, cultural disapproval, shyness, procurement difficulties, ignorance or inadequate information, moral disapproval, long distances of sources, and poor service of Family Planning Clinics and Planned Parenthood Federation of Nigeria. Fear of unknown effects ranked highest as a factor that militated against the use of modern birth-control methods in the area of study. It was identified as such by 25.3% of the respondents. This finding was in consonance with the report in Baron27, to the effect that low prevalence of the use of modern birth-control methods in Gambia and Kenya was “apparently due to fear of side effects…” However, the perceived fear might have derived more from unfounded rumours relating to the methods and the people’s ignorance of the workings of the methods than from their actual experiences. This ignorance was manifested in the view expressed by a female participant in the focus-group discussion held at Onicha, Ezinihite Mbaise. She said:
While there is no denying the fact that some of the modern birth-control methods may engender unpleasant consequences, especially if abused or misused, there had been no scientific proof of such grave consequences as alleged in the above report. Thus, the fears expressed by majority of the respondents were animated by ignorance and superstition, and sustained by malignant and pervasive rumours. Ranking next to “fear of the unknown effects’, as a likely barrier to the use or adoption of modern birth-control methods, was the factor of ‘health reaction’. A total of 89 respondents, or 24.7% of the total sample, identified this factor as a likely barrier. An intriguing fact here was that some of those who mentioned this factor had never used modern birth-control methods. This factor is closely related to the first factor of fear of unknown effects. Health reaction had been highlighted as a barrier to the use of modern birth-control methods. However, the nature and magnitude of reactions would naturally vary with the types, the individual users, the conditions under which the methods were used and, the skills of the providers. Religious beliefs were another factor identified by a relatively significant number of respondents as a barrier to the use of modern birth-control methods. Sixty-seven respondents, or 18.6%, identified it as such. Quite a few research works have reported religious opposition to family planning, with Roman Catholicism said to be the most vehement in this direction. Highlighting the relationship between religion and artificial birth control, Imo28 noted that Catholicism prohibited all artificial means of birth control but advocated the natural methods. Contrary to speculations, the data on Table 2 revealed that modern birth control or clinics and services were available in varied numbers and degrees in the communities’ studied. Although the respondents claimed that the clinics were non-functional. Conclusion and Recommendation The results of this study concluded that the use of Modern Birth Control Methods was still very low in the study area. Only 30% of the respondents used MBCM while the majority of them relied on the traditional methods for birth control. It is therefore recommended that governments and NGOs should provide more educational opportunities in the rural areas for the purpose of teaching birth control methods. More primary health centers, with strong family planning facilities should be made available in the rural areas. Religion and religious leaders play very strong roles in the decision to use contraceptives among the people. It is therefore necessary for religious leaders to be targeted for more education on the benefits of MBCM use. Since the majority of the rural people still rely on the traditional birth control methods, it would be necessary for researchers to study these methods with the view to improving on their success rate. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08015t2.jpg] [rh08015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}