 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
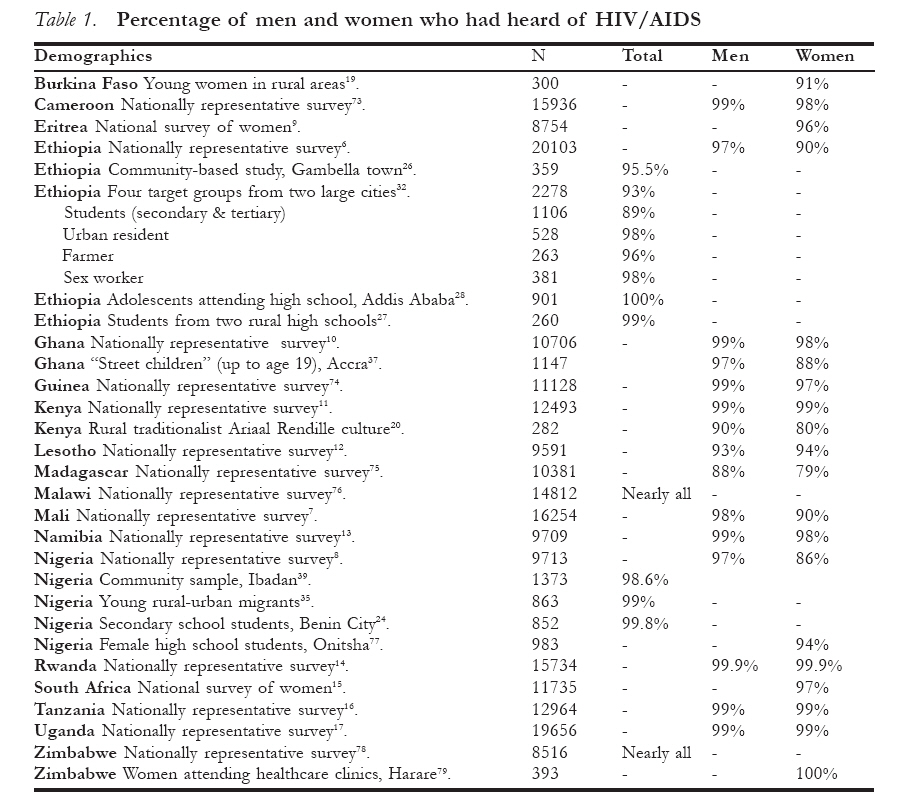
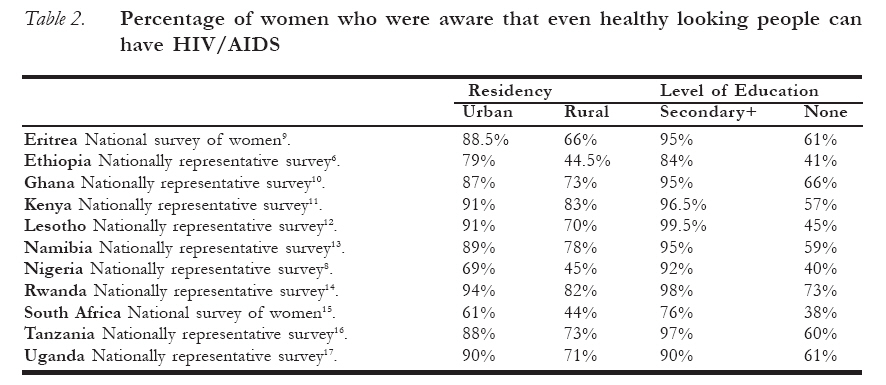
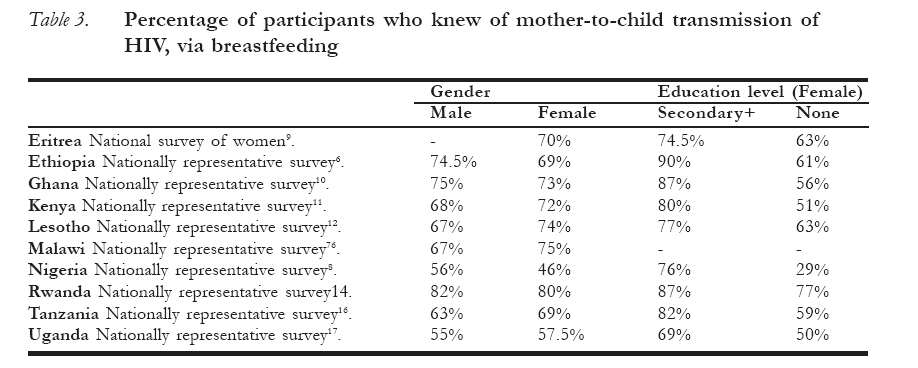
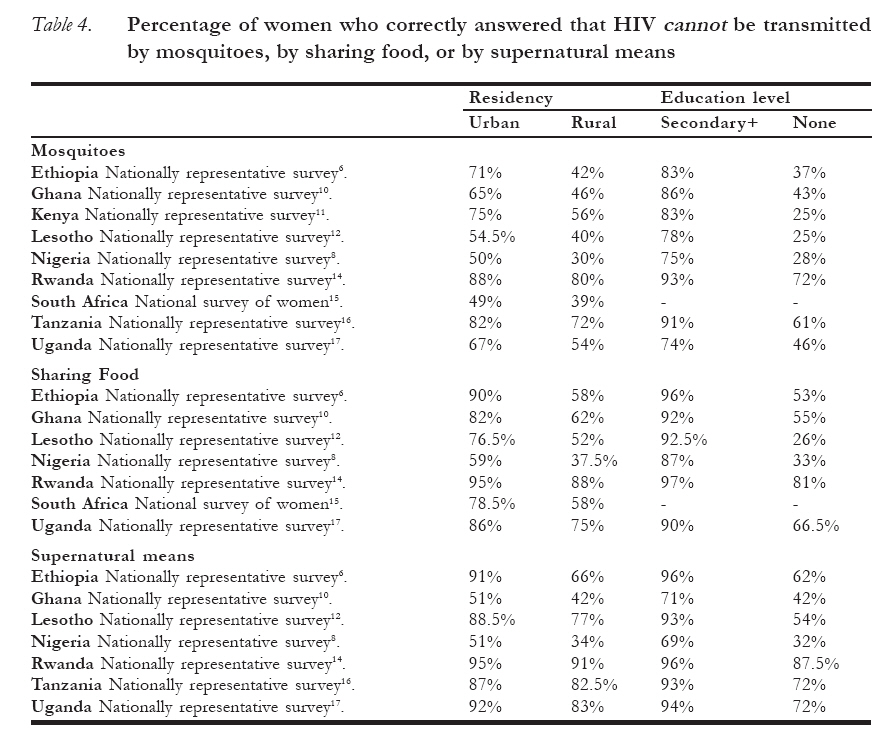
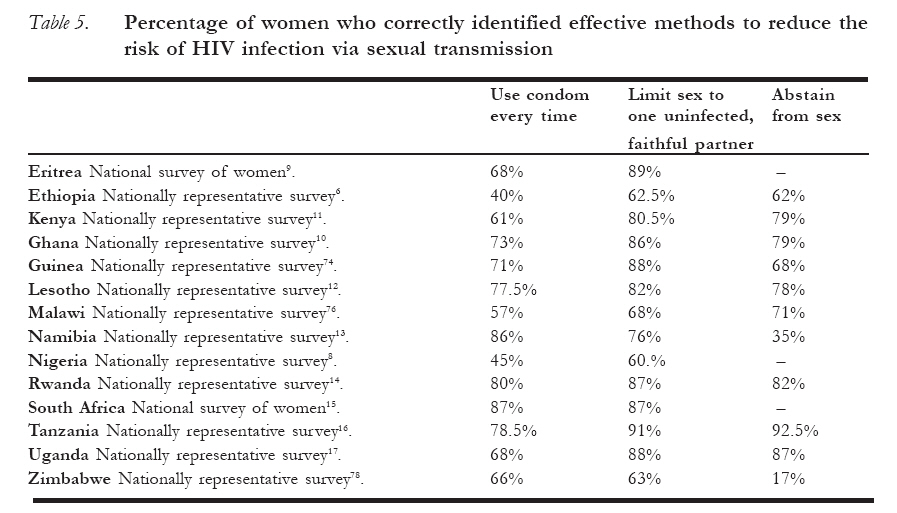
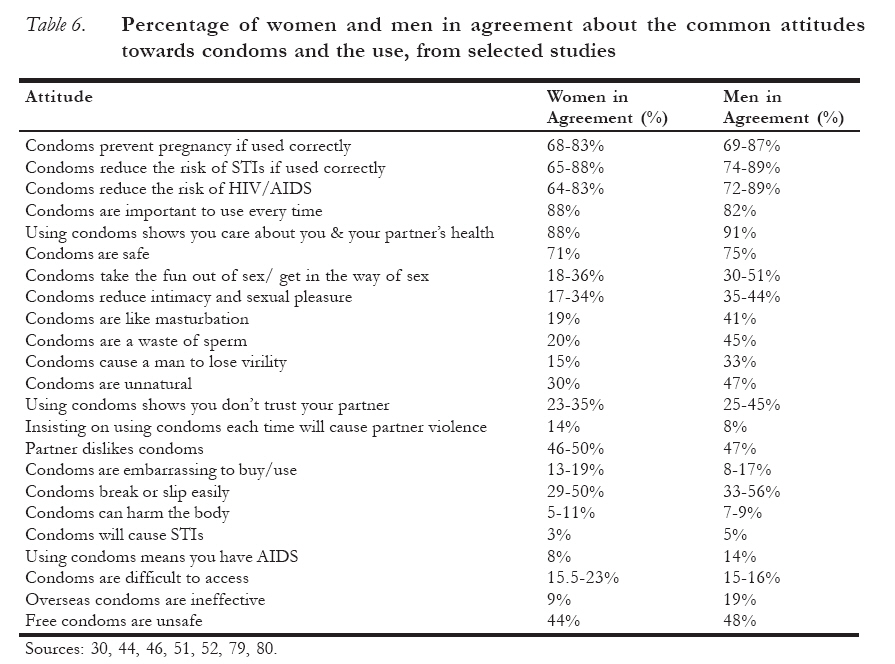
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 14-31 ORIGINAL RESEARCH ARTICLES Knowledge of HIV and AIDS in women in sub-Saharan Africa Connaissance du VIH/SIDA chez les femmes en Afrique sub-saharienne Amy D. Burgoyne and Peter D. Drummond Amy D. Burgoyne and Peter D. Drummond, School of Psychology, Murdoch University, Perth, Western Australia Code Number: rh08020 ABSTRACT Although most African people have heard of HIV and AIDS, there is still widespread misunderstanding about how HIV is spread, the consequences of infection, and how to protect against infection. The most vulnerable groups are poorly educated women, those from rural backgrounds, and women who are economically dependent on men. Lower levels of education, taboos associated with the discussion of sexuality and sexual health, the submissive role of women in a relationship, and male control of decision-making regarding sexual relations might explain why African women are less knowledgeable about HIV/AIDS than men. Although most African men and women are aware of the protective benefits of condoms, negative attitudes towards the acceptability and safety of condom use are widespread. More sexual health campaigns tailored to women, especially those with low education levels and those from rural areas, are needed to reduce the spread of HIV in Africa. RÉSUMÉ Bien que la plupart des Africains aient entendu parler du VIH et du SIDA, il existe toujours une malconception répandue concernant la manière dont le VIH est propagé, la conséquence d´ une infection et comment empêcher l‘infection. Les groupes les plus vulnérables sont les femmes peu instruites, celles qui viennent des milieux ruraux et les femmes qui dépendent économiquement des homes. Les niveaux bas d‘ instruction, les tabous liés à la discussion de la sexualité et de la santé sexuelle, le rôle soumis des femmes dans une relation et la domination de l´homme par rapport à la prise de décision concernant les relations sexuelles peuvent expliquer pourquoi les femmes africaines s´y connaissent mieux en VIH/SIDA que les hommes. Bien que la plupart des hommes et des femmes africaines soient au courant des avantages protecteurs des préservatifs, il existe un peu partout des attitudes négatives envers l´acceptabilité et la sécurité de l´ usage du préservatif. Pour réduire la propagation du VIH en Afrique, il faut davantage des campagnes en faveur de la santé qui viseront les femmes, surtout celles qui ne sont pas bien instruites et celles des milieux ruraux. KEY WORDS: HIV/AIDS awareness; HIV myths; attitudes toward condom use Introduction Women in sub-Saharan countries are considered to be one of the most vulnerable populations in the world for HIV. Three quarters (76%, or 13.2 million) of all HIV positive women live in this part of the world1. While women in many parts of the world have a longer life expectancy than men, in four countries of sub-Saharan Africa – Kenya, Malawi, Zambia and Zimbabwe – the life expectancy of women has been driven lower than that of men as a result of AIDS1. A wide range of biological, economic, and socio-cultural factors increase vulnerability of African women to HIV infection. African women and girls typically have poor access to education and health information, suffer inequality in marriage and sexual relations, are economically dependent on their male partners, and are part of cultural traditions that reinforce gender inequalities2, 3 . Additionally, women are physiologically more vulnerable to HIV infection than men4, particularly women with sexually transmitted infections5. Therefore, it is vital that all African women know about HIV and AIDS3. Women not only need to know about the disease but also about methods of transmission, to understand and reject misconceptions regarding HIV/AIDS, and know how to protect them-selves from infection. The literature reviewed below provides a snapshot of the current state of knowledge about HIV/AIDS in women in sub-Saharan Africa. Although most African women have heard of HIV and AIDS, less is known about how HIV is spread or how to protect against infection. In the nationally representative surveys conducted in Ethiopia, Mali, and Nigeria, 97-98% of the men had heard of AIDS compared with only 86-90% of women6,8. The gender difference was also present in a national survey conducted in Madagascar, and in a study of the rural traditionalist Ariaal Rendille culture in Northern Kenya (Table 1). Both studies recorded levels of awareness at or below 90% but, in both studies, a higher percentage of men than women had heard of AIDS. Urban-rural differences. Nation-wide surveys from Nigeria and Ethiopia revealed strong differences between women living in urban and rural areas. In Nigeria, 95% of women living in urban areas were aware of AIDS, compared with only 82% of women living in rural areas8. In Ethiopia, women in urban areas had an almost universal awareness of AIDS compared with only 88% of women in rural areas6. Ethiopia also showed some of the strongest differences in awareness of AIDS across its regions. There was a striking lack of knowledge in the Somali, Gambela, and Benishangul-Gumuz regions of Ethiopia. The Somali region had the lowest levels of awareness, as only 50% of women and 64% of men had heard of AIDS – and this lack of knowledge was obvious across all HIV/AIDS knowledge domains. In the Gambella region, 63% of women and 88% of men had heard of AIDS, and in the Benishangul-Gumuz region, 68% of women and 95% of men knew about AIDS. The massive difference between the awareness levels of men and women in these areas obviously needs to be addressed6. Fortunately, however, some countries (Eritrea ,Ghana, Kenya, Lesotho, Namibia, Rwanda, South Africa, Tanzania, and Uganda) have high levels of awareness (at least 90%) amongst women both in urban and rural locations9-17. Education. In the studies reviewed, HIV/AIDS awareness varied across levels of education for women in Lesotho, Nigeria, and Ethiopia. In Lesotho, all women with secondary education and above had heard of AIDS whereas only 80% of women without any education knew about AIDS12. Similar trends were identified in Ethiopia6 and Nigeria8. Basic Knowledge about HIV/AIDS Basic knowledge about HIV/AIDS appears to be quite limited in some African communities. For instance, in a survey of 1200 women of reproductive age in Bida Emirate of Niger State, Nigeria, only 15% were able to describe HIV/AIDS as a deadly disease18. Over 90% of these women had no or only rudimentary levels of education. Only 69% of young women surveyed in the rural areas of Burkina Faso were aware that AIDS was deadly19, and a study of the rural traditionalist Ariaal Rendille culture in Northern Kenya found that significantly fewer women (64%) than men (84%) named ‘wasting’ as a symptom of AIDS20. In a survey of first year university students in Nigeria, 93% were aware that HIV causes AIDS21. Similar studies of Nigerian high school students showed varying results, with only half the students in one study aware that HIV was the cause of AIDS22 and 69% in another were aware that HIV was caused by a virus23; however 74% of students in a third study claimed to be unaware of the cause of the disease24. A high percentage of women (93%) in a study in South Africa were aware than even a healthy looking person could have HIV/AIDS25. In a community-based study in Gambella, Ethiopia, 84% of participants knew that even healthy-looking people can have HIV/ AIDS26. Similarly, 93% of adolescents surveyed in two rural high schools in north western Ethiopia were aware of this27. However, this compared with only 31% of 300 women from rural areas in Burkina Faso19. (Further details from nationallyrepresentative samples are shown in (Table 2). Many African women incorrectly believe that AIDS can be cured21, 22, 28-30. For instance, in a survey of adolescents attending high schools in Addis Ababa, Ethiopia, one-third thought there was a vaccine for AIDS28, and in a study of secondary students in Nigeria, 72% believed AIDS could be cured23. Moreover, the myth that having sex with a virgin can cure AIDS is widespread30, 31. Knowledge about correct modes of transmission Most African people are now aware that HIV can be transmitted through unsafe sex. More than 95% of urban residents, farmers, and sex workers from around two cities in Ethiopia were aware of this32, as were the students from two rural high schools in Ethiopia27, and 100% of urban residents and 99% of rural residents from Tanzania33. The majority of secondary students in studies from Nigeria (90%)23 and Ethiopia (85%)34 were aware that HIV could be transmi-tted via unprotected sex. However, young ruralurban migrants in Nigeria (85-88%)35, community-based samples from Tanzania (81%)36 and Gambella town, Ethiopia (80%)26, and young women from rural areas in Burkina Faso (77%)19 had lower levels of knowledge. Only 68% of secondary students in Benin City, Nigeria, were aware that HIV can be transmitted via unsafe sex24. In a study of “street children” in Accra, Ghana, only 10% of females, compared to 56% of males, knew that HIV was transmitted this way37. Knowledge about other modes of transmission is more variable. Most urban residents (96%), sex workers (96%) and students (92%) and farmers (87.5%) from around two Ethiopian cities32, students from an urban high school in Ethiopia (79%)34, and students from two rural high schools in Ethiopia (92%)27, were aware that HIV can be transmitted through unsterilised injecting equipment. Similar percentages were aware that unscreened blood transfusion could transmit HIV32. Just over 60% of urban residents in a study from Tanzania were aware that HIV/AIDS could be transmitted by blood transfusion, contaminated instruments, and mother to child transmission, however only just over 40% of rural residents were aware of this33. First year university students in Nigeria correctly reported that contact with bodily fluids (98%) and sharing injection needles (84%) were methods of transmission21. Knowledge was much lower among secondary school students in Benin City, Nigeria, where less than half of the students were aware that HIV could be transmitted via blood transfusion (44%) and sharing injection needles (21%)24. However, less than two thirds of young rural-urban migrants in Nigeria35, 28% of people from a community sample in Tanzania36, and 13% of people from a community based study in Ethiopia26 knew that unsterilized injecting equipment or sharp instruments were possible modes of transmission. Overall levels of awareness of correct modes of transmission varied across three South African studies. Men and women in a black South African township had fairly good HIV/AIDS knowledge overall, with 83% of participants giving correct answers on a test on the methods of HIV/AIDS transmission29. Youths living in a black South African township had similar levels of HIV/AIDSrelated knowledge30. However, very low levels of HIV knowledge were found amongst rural residents in South Africa after they had received a diagnosis of AIDS38. The participants (N=13) were attending support groups for HIV/AIDS, and were unemployed, had minimal education (none had completed high school), and were diagnosed because they were already showing signs of AIDS. They knew little about HIV/AIDS except for the information they had received from the mass media and word of mouth. All had heard of HIV/AIDS before their diagnosis, but knew little else about HIV/ AIDS until they attended support group meetings38. Mother-to-child transmission is the major means of HIV infection in children, as up to 40% of children born to HIV positive women will become infected themselves unless the mother is undergoing preventative treatment4. Of the children infected via mother-to-child transmission, two thirds of children are thought to be infected during pregnancy and delivery, and one third during breastfeeding. Knowledge of mother-tochild transmission was very inconsistent across the studies reviewed (Table 3). More than three quarters of women from Rwanda and Malawi, and men from Ghana and Rwanda, were aware of mother-to-child transmission of HIV. More than six in ten females from Ghana and Eritrea, males from Malawi, and males and females from Kenya, Ethiopia, Lesotho, and Tanzania, knew of mother-to-child transmission. But less than six in ten men and women from Uganda and Nigeria had heard of this form of transmission. Between 69-90% of women with secondary education and above had heard of mother-to-child transmission, but only 29-77% of women with no education had heard of it. Just over two-thirds of students from a study in Ethiopia were aware of mother-to-child transmission of HIV34. Other studies revealed quite low levels of mother-to-child transmission knowledge. In Nigeria, only 32% of first year university students21 and 20% of secondary school students24 knew of mother-to-child transmission. In community-based studies in Nigeria (8.2%)39, Ethiopia (0.9%)26, and Tanzania (0.8%)36, knowledge of this mode of transmission was extremely low. This high variation in knowledge of mother-to-child transmission needs to be addressed in education programs aimed at both sexes. Myths about the spread of HIV Three common misconceptions are that HIV can be transmitted by mosquito bites, by sharing food with another person who has HIV, or by supernatural means. Overall, a high proportion of women had misconceptions about methods of HIV transmission (Table 4). As might be expected, women from rural areas and women with no education had more misconceptions than those from urban areas and with at least secondary education. Female “street children” from Accra, Ghana, believed many myths about the transmission of HIV, with nearly one in ten suggesting misconceptions like witchcraft, use of a toilet, women travellers, eating bad food, flies, dirt, and eating, touching, or talking with someone with AIDS; in addition, 56% did not know at all how HIV is transmitted37. However, women from Rwanda appear to be an exception, as their knowledge levels were high across all demo-graphics when compared with other countries14. Three separate studies conducted in black South African townships showed quite high levels of misconceptions. Eleven percent of participants from one community sample40 and 43% of participants from another29 incorrectly believed that AIDS was caused by supernatural means. In a sample of youth from South African townships, over one-third of participants (39%) believed that spirits and supernatural forces cause AIDS30. Three different studies of different population groups in Ethiopia also revealed quite high levels of misconceptions about methods of HIV transmission. Nearly one quarter of students attending high schools in Addis Ababa, Ethiopia, had misconceptions about methods of transmission. These miscon-ceptions included transmission by mosquito bites, and wearing clothes, sharing food, eating, shaking hands, and sharing toilets with people with HIV/ AIDS. No major differences were reported between the responses of the male and female students28. One quarter of the participants in a study from rural high schools in Ethiopia believed that mosquitoes can carry the virus27. Many participants reported incorrect modes of transmission, such as by mosquitoes (37.5%), kissing (26%) and saliva transfer (33%), sharing toothbrushes (88%), sharing property (24%) and sharing toilets (22%), from the study of four different target groups living around two large cities in Ethiopia. Farmers in particular, followed by sex workers, had many misconceptions32. The protective value of washing after sex is another common misconception. Approximately one quarter of participants in two different studies in black townships in South Africa believed that washing after sex can prevent and protect against AIDS29, 30. Methods of Prevention A greater percentage of men than women in each nation-wide study (Table 5) were aware that using condoms every time (64-92% of men compared to 40-86% of women), limiting sex to one faithful, uninfected partner (76-90% versus 60-91%), and abstaining from sex (30-90% versus 1792.5%) were all methods to reduce the risk of HIV infection. In general, a much higher proportion of secondary-educated women knew that condoms (60-97% of secondary educated women compared to 30-74% of women with no education), limiting sex to a faithful, uninfected partner (72-98% versus 39.5-85%), and abstinence (46.5-96% versus 8-87%) could reduce the risk of HIV infection. However, in Rwanda, 2% more women with no education compared to women with secondary education knew that abstaining from sex could reduce the risk of HIV. The most commonly reported HIV prevention methods among 285 first year university students in Nigeria were safe sex with condoms (77.2%), abstinence (38.6%), and not sharing personal instruments, such as razors (36.8%)21. Sexually active adolescents had more information about prevention behaviours for HIV, such as condom use for casual sex (66% vs. 47%), monogamy (63% vs. 44%), and avoiding causal sex (53% vs. 39%). However, the overall percentage of adolescents who knew about these methods was low22. The knowledge of preventative measures such as abstinence (37-44%), using condoms (29-41%), and limiting sex to one partner (9-10%) was also quite low in young rural-urban migrants in Nigeria41, 42 . Attitudes about condom use Condoms are promoted as one of the primary prevention methods for HIV infection because they can prevent pregnancy and reduce the risk of HIV and other sexually transmitted infections. While there are both male and female condoms, female condoms are typically more expensive and have not been promoted as extensively as male condoms3, 4. Because attitudes towards female condoms have not been examined as extensively as attitudes towards male condoms, this review will be concerned with attitudes towards male condoms unless otherwise stated. Attitudes towards condoms and reasons why they are not used are listed in Table 6. Based on their conversations with sex workers, their clients, and other men in the Mombasa district of Kenya (which has important port, rail, trucking, and tourism industries), field workers compiled a list of over 50 reasons why men do not use a condom43. These were organised into six main categories: condoms are not pleasurable, condoms are defective, condoms are harmful, condoms are unnecessary, condoms are too hard to use, and external forces prevent their use. Many respondents, particularly men, thought that condoms decreased pleasure during sex30, 43-53 . Similarly, respondents thought that condoms took the fun out of sex, got in the way of sex, prevented fleshto-flesh contact, and reduced intimacy. They also thought that condoms were unnatural30, that they were a waste of sperm49, 52, and they cause a man to become impotent and lose his virility49, 52. Some respondents also thought that condoms were unsafe. A minority of men and women thought that condoms were harmful and can cause health problems43, 44, 52, 53 and that they can get caught in a woman’s vagina and make her sick or die49, 54. Both men than women thought that condoms could slip or break easily (so using them is pointless)43, 46, 51 (Table 6). There was also the common attitude that free condoms are unsafe and unpleasant30, 48 held by almost half of the men and women surveyed, and that the safety of condoms was actually misleading, because of the misconception that condoms have tiny holes in them that HIV/AIDS can slip through43, 49. In addition, some men and women thought that condoms were dangerous, because white people introduced condoms laced with HIV/AIDS to Africa to reduce the population43, 48, 49. Many respondents thought that women and girls who carried condoms were promiscuous, and those who insisted on their use were too experienced. This attitude was present both in women and men, and prevented many women from attempting to use condoms35, 43, 45-47, 49, 50, 55, 56 . For example, in focus group discussions with 94 Akamba girls aged 15–19 years from secondary schools in rural Kenya57, girls who carried condoms or insisted on their use were often labelled as promiscuous or prostitutes (especially by the boys), whereas boys were seen as responsible. The girls who were interviewed explained that premarital sex was highly disapproved of (especially for young women), so carrying condoms was like an admission of having had sex57. There was also the concern from women that asking to use condoms during sex would lead to violence or abandonment55. The financial implications of this abandonment may cause many women to conclude that they cannot use condoms55,58. Another common attitude was that using condoms, or suggesting the use of condoms, shows that you do not trust your partner35, 44, 47, 51, 52, 56. Some women were also concerned that men may deliberately sabotage the effectiveness of condoms by putting holes in them or slipping them off during sex so that they may impregnate the woman or infect her 48, 54, 55. Many men confirmed that they actually did this54. One of the reasons not to use a condom reported by several men was that “if you are infected, having unprotected sex with as many other people as possible will allow you to pass the disease onto them and eliminate it from yourself ”43 (p. 432). Despite quite high levels of agreement with some of the negative attitudes towards condoms, it is important to note that the highest levels of agreement in African men and women concerned positive attitudes towards condoms (Table 6). In particular, the majority of men and women surveyed believed that condoms can protect against pregnancy, sexually transmitted infections and HIV/AIDS. Most men and women also believed that condoms are important to use every time, and using them shows that you care about your own and your partner’s health. Over 70% of men and women also agreed that condoms are safe to use. Negative attitudes and beliefs about the acceptability and safety of condoms, however, must be addressed if condom use is to increase. Discussion Across all the studies, African men usually had greater knowledge of HIV/AIDS and related topics than African women although in a few studies a large number of men and women had an equally good knowledge of HIV/AIDS. Rwanda’s nation-wide study, for example, identified large numbers of knowledgeable people, regardless of gender, location, or education level14. Knowledge of mother-to-child-transmission of HIV (via breastfeeding specifically) was an exception – in half of the studies examined, a greater percentage of men were aware of motherto-child transmission, but in the other half, a greater percentage of women were aware. Aside from these few exceptions, it was clear that a smaller proportion of African women than men were aware of HIV/AIDS, how it is spread and how to avoid being infected. Taboos associated with the discussion of sexuality and sexual health, the submissive role of women in a relationship, lower levels of education, and the male control of decision-making regarding sexual relations might explain why African women are not as exposed to HIV/AIDS messages as men. Many African women and men have misconceptions about the transmission of HIV. These misconceptions can lead to discrimination and stigmatisation against people with HIV/AIDS. Fear about infecting others may also prevent those infected from getting the care and help they need4. Discrimination against people living with HIV/AIDS can lead to violations of human rights, such as denial of health care, work, and education59. Sexual health programs in Africa are often aimed at adolescents and are conducted through schools31. Understandably, the gap in knowledge levels is greatest between illiterate women with no education and women with secondary education and above. Urban women have better knowledge about HIV/AIDS than their rural counterparts, due to the difficulty in running education campaigns in remote areas. The most common prevention programmes and activities in Africa include HIV/AIDS education in schools, peer education for high risk groups (e.g., out-of-school youth, commercial sex workers, drug users), widespread communication campaigns (via the radio, pamphlets, posters, etc) against risky behaviour, HIV testing for pregnant women (plus counselling and treatment if the HIV test result is positive), and free condom distribution31. More programmes tailored to women, especially those with low education levels and those from rural areas, are required. However, these programmes also need to address socio-cultural influences on sexuality, and violence against women. Lack of control over sexuality As many African societies have social and cultural taboos about discussing sex, women often do not feel comfortable seeking information about HIV/AIDS, sexually transmitted infections and condoms, even among health-care professionals60. This lack of knowledge, and an inability to comfortably access knowledge about sexual and reproductive health, puts African women at greater risk for HIV infection. “Sex continues to be defined in terms of male desire with women being relatively passive recipients of male passions”2. In many African societies, men traditionally are permitted to have multiple partners and sex outside the relationship, whereas even a suspected affair on the woman’s part may result in ostracism and abandonment4, 58. Although women may be aware that their partner is not monogamous, they may feel powerless to change the situation or insist on condom use. This puts the women at even greater risk of HIV infection 19. Many African women lack control in sexual matters, and are expected to be submissive and leave the initiative and decision making in sexual relations to men4. They have little opportunity to negotiate safe sex, to control when and how sex occurs, or to control the sexual lives of their partners4, 58. Married women and adolescent girls have been identified as populations at risk3. For married adolescent girls and young women in Kenya and Zambia, marriage increases the frequency of sexual intercourse, decreases condom use, and minimises their ability to abstain from sex in comparison to their unmarried peers61. Unfortunately, these married adolescent girls and young women also have higher rates of HIV infection than their peers. Although discussing condom use is becoming more acceptable outside marriage, this is not yet acceptable inside marriage62. Married women are often neglected in HIV/AIDS education campaigns, but they clearly are a group at risk61. Violence against Women Physical and sexual violence from a partner seems to be accepted to a certain degree in many African cultures3, 58. In the year prior to a nation-wide study of women in South Africa, one in ten women had experienced physical assault, 6% by a current or expartner and 4% by someone who was not a partner15. In many cases violence against women is seen as a private matter and a normal part of a relationship, so women are often without a chance of legal recourse3. Intimate partner violence is associated with increased levels of HIV risk behaviour, such as multiple partners, having a non-primary partner, bartering sex for goods or money, and problems with substance use3. But even after their own risk behaviour is taken into account, women who have experienced partner violence or are currently involved with an aggressive partner are at increased risk of HIV infection63. For example, in a study of women attending a voluntary counselling and testing clinic in Dar es Salaam, Tanzania, women infected with HIV were significantly more likely to have had a physically violent partner at some point in their life than those without HIV64. Women infected with HIV were also significantly more likely to have experienced physical violence, sexual violence, or both, with their current partner. One in five women attending prenatal and paediatric clinics in Kigali, Rwanda, revealed that they had experienced physical violence from their regular partner65. Additionally, one third of the women reported sexual coercion, and one third reported that their partner would get angry at their refusal to have sex. The presence of physical violence may also hinder condom negotiation and use on the part of the female partner65. In a study of men and women attending a sexual health clinic in Cape Town, South Africa, more than 40% of women and 16% of men had been victims of at least one sexual assault, and more that one in five men in the study admitted to perpetrating sexual assault against a woman66. As many as one in five men and women (in some cases, up to one in three) supported the view that rape is usually a woman’s fault and the result of what she said or did. There was little difference between the answers of men and women. They both “endorsed the view that women are subordinate to men and passive in their relationships with men and that women are often to blame for rape”66 (p. 304). The idea of rape within a marriage is not even considered by many60. As reported by one, “men also believe it is ridiculous that a husband might be regarded as having raped his wife – ‘one cannot steal what belongs to oneself ’”48 (p. 683). African women with greater economic independence may feel they have more power to negotiate safe sex and condom use, because the potential loss of their partner would not affect their capacity to support themselves or their children67. Women who had their own source of income also reported less sexual coercion or physical violence from their partner65. However, some women feel that they have to use sex as a commodity to survive. Women in a Tanzanian study with a partner more than 12 years older than themselves were at increased risk for HIV infection68. Younger women with a poor economic background sometimes seek out relationships with older men who have a stable income57. These men may provide them with gifts or money or general economic support in return for sex31, 69. Many young women may use the money towards school books, fees and uniforms, to help them stay at school where they know they will get more opportunities in life60. Older men also seek out younger girls, because they perceive them to be safer with less chance of infection58. But unfortunately for the younger girls, older men are more likely to have sexually transmitted infections, including HIV, so the chance of the girls becoming infected is greatly increased3, 49. Women are also placed in a weaker position in these relationships, diminishing their ability to negotiate safe sex69. African women may turn to prostitution as a means of survival after the loss of their husband (the source of economic support) through divorce, widowhood, or other reasons, such as the husband leaving to look for employment prospects elsewhere4, 58. For unskilled, unemployed, and minimally educated women who are in a poor economic position with a family to support, selling or bartering sex may be the only viable option to generate an income. African sex workers are often expected to reduce their rate of payment if they insist on using a condom70. Even if the sex workers are aware of the risks of not using a condom, the loss of income may be considered too great not to take the risk. Suggesting condom use may also be met with physical violence and rougher sex70. Education gives women more opportunities for employment and gender equality3, and increases the likelihood of protection against HIV infection. Unfortuna-tely, lack of money to afford education, migration of the family due to poor economic conditions, unwanted pregnancy, and marriage reduce opportunities for education60, 71. In addition, the illness of a family member due to AIDS may also force a woman or girl out of school and into the home as a caregiver 1, 72. This may reduce educational and employment opportunities, increase economic dependence on others and, in turn, increase vulnerability to HIV infection. Preventing this type of negative spiral needs to be a focus of international aid programmes. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08020t2.jpg] [rh08020t6.jpg] [rh08020t4.jpg] [rh08020t3.jpg] [rh08020t1.jpg] [rh08020t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}