 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 45-63 Family planning methods among women in a vaginal microbicide feasibility study in rural Kwa Zulu-Natal, South Africa Méthodes de la planification familiale chez les femmes à travers une étude de faisabilité microbicide à Kwa Zulu-Natal rural, Afrique du-Sud Laura Subramanian1, Nuala McGrath*1,2, Hlengiwe Ndlovu1, Mitzy Gafos1 1Africa Centre for Health and Population Studies, University of KwaZulu-Natal, PO Box 198, Mtubatuba 3935, KwaZulu-Natal, South Africa 2London School of Hygiene and Tropical Medicine, Keppel St, London, England Code Number: rh08022 ABSTRACT This study investigated contraceptive use among women in rural KwaZulu-Natal, South Africa. Of 866 sexually active women not intending pregnancy and screened for a microbicide feasibility study, 466 (54%) reported currently using modern contraceptives: injectables (31%), condoms (12%), sterilization (6%) and pills (4%). Multivariable logistic regression analyses revealed statistically significantly higher odds of current contraceptive use among married vs. engaged/unmarried women (aOR 1.64), multiparous vs. nulliparous (aOR 4.45) and women who completed secondary education or above vs. primary or less (aOR 1.64). Significantly lower odds of use were observed among women aged 40+ vs. age 15-19 (aOR 0.38). Age, marital status, education level and parity were associated with different contraceptive method choices. Among 195 women followed longitudinally for 9 months, contraceptive use increased significantly from 56% to 70%, largely due to increased condom use (15% to 28%). Results highlight the importance of integrating family planning and HIV/STI prevention counseling and informing promotion of further contraceptive uptake among women not intending pregnancy. RÉSUMÉ Il a s’agit dans cette étude d’examiner l’usage du contraceptif chez les femmes à KwaZulu-Natal en Afrique du Sud. Sur les 866 femmes sexuellement actives qui ne voulaient pas être enceintes et qui ont été préselectionnées pour une étude de la faisabilité microbicide 466(54%) ont signalé qu’ils utilisent actuellement des contraceptifs modernes. Les méthodes primaries comprenaient les injectables (31%), des préservatifs (12%),la stérilisation (6%) et les pilules (4%). Les analyses multifactorielles ont montré des differences statistiques importantes en ce qui concerne l’usage moderne du contraceptif chez les femmes âgées de 40+ans(a OR 0,38 par opposition à l’âge 15-19) qui sont mariées (a OR 1,64 par opposition aux financées/ célibataires),multipares (a ORS de 2,67 à 4,45 par opposition à aucune naissance)et qui .disposent d’un diplôme secondaire ou d’un diplôme supérieur (a OR 1,64 par opposition au primaire ou moins). L’âge, l’ état civil, le niveau d’instruction et la parité sont liés aux méthodes diverses des choix. Chez les 195 femmes que nous avons suivies longitudinalement pendant 9 mois, l’usage du contraceptif a augmenté de mamière significative, de 56% à 70% dû en grande partie à l’augmentation de l’emploi. Les résultats mettent en lumière l’importance de l’intégration de la planification familale et du conseil pour la prévention du VIH/IST, et en se servant des renseignements sur les indices de l’usage pour la promotion de l’usage du contraceptif chez les femmes qui ne veulent être enceintes. KEY WORDS: Family planning, contraception, South Africa, microbicides Introduction Family planning is an important aspect of women’s health and lives. Childbearing intervals, number of children and choice of contraceptive method impact on women’s gynecological and overall health, as well as their social and economic status in society1, 2. Frequent childbearing, short birth intervals, and unsafe abortion contribute to maternal mortality and morbidity in the developing world3. In Africa, approximately 20% of all pregnancies are unintended, significantly impacting on women’s physical, social and economic well-being3. In South Africa, the severity of the HIV epidemic has resulted in an increased need for emphasis on dual protection from pregnancy and sexually transmitted infections4. Knowledge about modern contraceptives and access to family planning services are two key factors that have been shown to influence contraceptive use5-8 in sub-Saharan Africa. According to the 2003 South Africa Demo-graphic and Health Survey (SADHS), 97% of sexually active South African women know of at least one modern method of contraception. The best known methods are injectables (88%), male condoms (83%) and pills (82%)9. These findings suggest that knowledge of modern contraceptives is relatively universal among South African women and other factors such as access to services, fertility preferences, relationship dynamics and socio-demographic characteristics may influence family planning choices in this population. In order to ensure that women who want to utilize contraceptives are able to do so, it is necessary to understand the factors influencing women’s contraceptive choices in South Africa. Family planning use in rural South Africa has been investigated in prior studies. SADHS found that in 2003, 63% of sexually active women in rural areas aged 15-49 were currently using a modern method of family planning9. According to SADHS, injectables are the most popular contraceptive method in this population, with 38% of women reporting current use at the time of the survey. In contrast, relatively few women used pills (11%), condoms (8%) or female sterilization (5%). Data from rural KwaZulu-Natal indicate lowest contraceptive use among adolescents; only 20% of sexually active women aged 15-19 report ever having used contracep-tives, compared to 60% of 20-24 year-olds in this population10. Despite a relative wealth of data on contraceptive prevalence, there is little information about predictors of contraceptive use among rural South African women. Factors such as education, urban residence and perceived HIV risk have been found to predict condom use in rural KwaZulu-Natal11 12, but data are needed regarding predictors of other family planning methods. In addition, recent evidence on hormonal contraceptive use and risk of HIV infection13,14 underlines the importance of understanding contraceptive practices in high HIV prevalence areas such as rural South Africa. Some studies have evaluated the impact of service utilization on contraceptive use using national demographic and health data15, antenatal/postpartum16,17 and longitudinal data18, and found that receipt of family planning services and/or HIV counseling increased modern contraceptive use. However, few studies have investigated changes in contraceptive use among cohorts in sub-Saharan Africa engaged in regular discussions about family planning and receiving repeated safer sex counseling. A microbicide feasibility study provided the opportunity to investigate both sociodemographic predictors of, and longitudinal changes in, contraceptive use, and provided more recent contraceptive use data than currently available through the South African national surveys.1 These data were collected as part of a microbicide feasibility study in preparation for the Microbicides Development Programme phase III clinical trial to evaluate the safety and efficacy of PRO2000/5 gel in preventing vaginally acquired HIV infection19. Unintended pregnancies during microbicide trials necessitate premature cessation of product use, impacting on endpoint calculations of HIV incidence and limiting ability to demonstrate microbicide effectiveness. Improved knowledge of predictors of, and longitudinal changes in, contraceptive use could inform family planning services and microbicide clinical trials regarding the provision of counseling to reduce the risk of unintended pregnancies. METHODS Sampling and Data Collection In preparation for a Microbicides Development Programme trial, the Africa Centre for Health and Population Studies (Africa Centre) conducted a feasibility study from June 2003 to December 2004 in the Umkhanyakude District of KwaZulu-Natal20. The study aimed to assess whether the Africa Centre could recruit, follow and retain women, measure HIV incidence, and measure HIV and STI prevalence in preparation for a vaginal microbicide clinical trial, and assess the acceptability of study procedures in this population. The Africa Centre recruited women from 3 local family planning and immunization clinics. Of 888 women screened for the study, 886 provided informed consent to answer questions about demographics, health, pregnancy history and contraceptive use. Women were offered voluntary HIV counseling and testing, and HIV status was determined using Abbot Determine and Smart check rapid HIV tests (with ELISA laboratory confirmation of positive rapid tests). Women were required to meet the following eligibility criteria for enrolment: age 15 or older; sexually active; non-pregnant and not intending pregnancy in the next 12 months; willing to attend the clinic for repeat visits, receive HIV test results at screening and undergo repeat testing for HIV and sexually transmitted infections, provide urine for pregnancy testing, answer questions about sexual behavior, and provide informed consent. Of the 888 women screened, 449 met the eligibility criteria and provided informed consent to enroll in the study. The main reason for non-eligibility was HIVpositive status at screening. Enrolled women were asked to attend follow-up visits 2 weeks after enrolment and then at 3-monthly intervals for a period of 12 months. At each visit, study staff administered question-naires on sexual behavior and health, conducted clinical exams where appropriate, and asked women to undergo repeat HIV testing. Detailed information about past and current use of family planning methods was collected at each visit. At screening, women were asked, “At the moment, are you doing something or using any method to delay or avoid getting pregnant?” At follow-up visits, women were asked the same question relating to contraceptive activity since their last visit. After noting spontaneous answers, interviewers read a list of modern and traditional contraceptive methods to participants and recorded probed responses for use of each method. Methods mentioned spontaneously that were not on the list were categorized as “other” and specifics were recorded. At each follow-up visit, women were asked if they were intending to become pregnant in the next 3 months, and were followed up regardless of their pregnancy intentions. At follow-up visits, women were asked separately about condom use for pregnancy prevention (as part of above questions) and condom use for HIV/STI prevention within the context of sexual relationships. 1South Africa DHS data is available from 1998, while the dataset for the SA 2003 DHS is not yet available. Objectives This analysis of Microbicide Feasibility Study data had 3 primary aims: (1) determine prevalence of contraceptive use among women screened for the Microbicide Feasibility Study; (2) identify sociodemographic determinants of contracep-tive use and method choice; and (3) investigate changes in contraceptive use during the Micro-bicide Feasibility Study. Measures Dependent variable The primary outcome measure for this analysis was current contraceptive use, defined as reported use of a modern contraceptive method21. We modeled current contraceptive use in two stages: use of any modern contraceptives, and choice of contraceptive method. Method choice was grouped to allow direct comparison with prior studies5 7. The dependent variables were cate-gorized as follows:
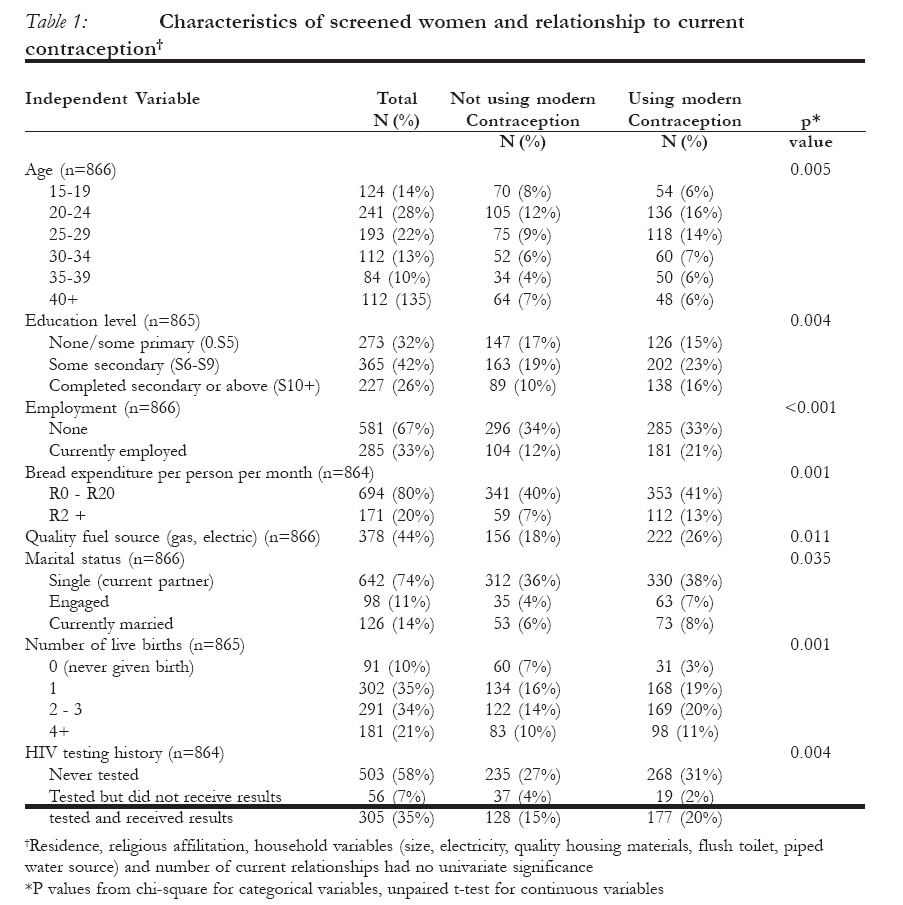
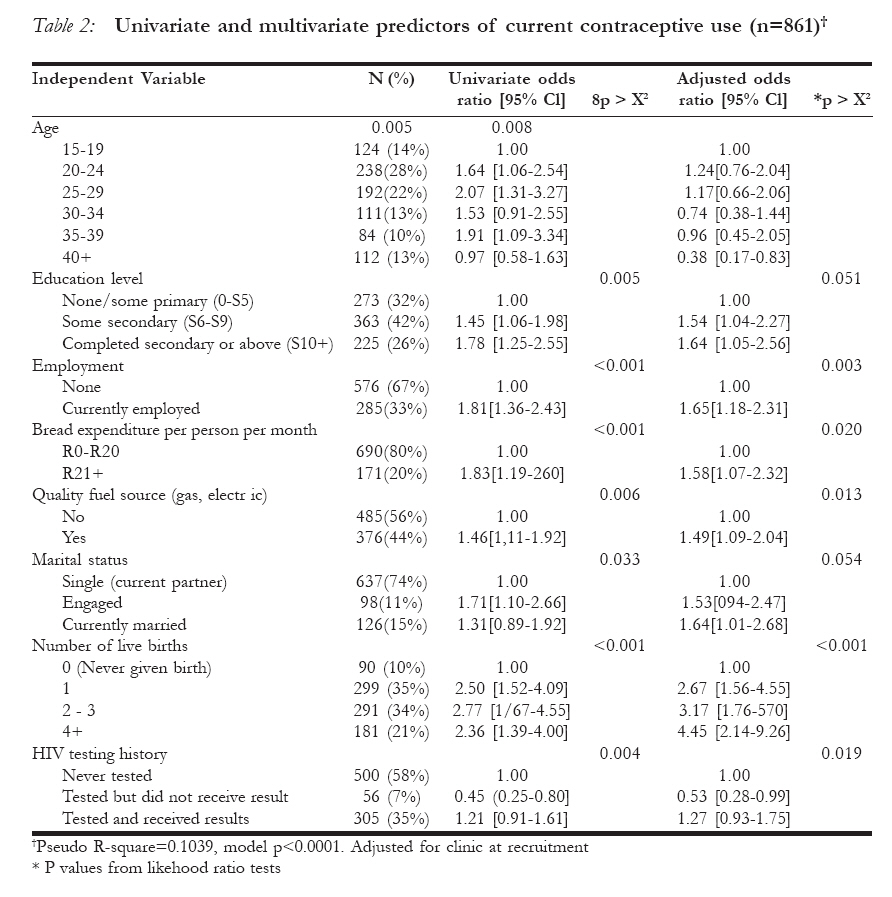
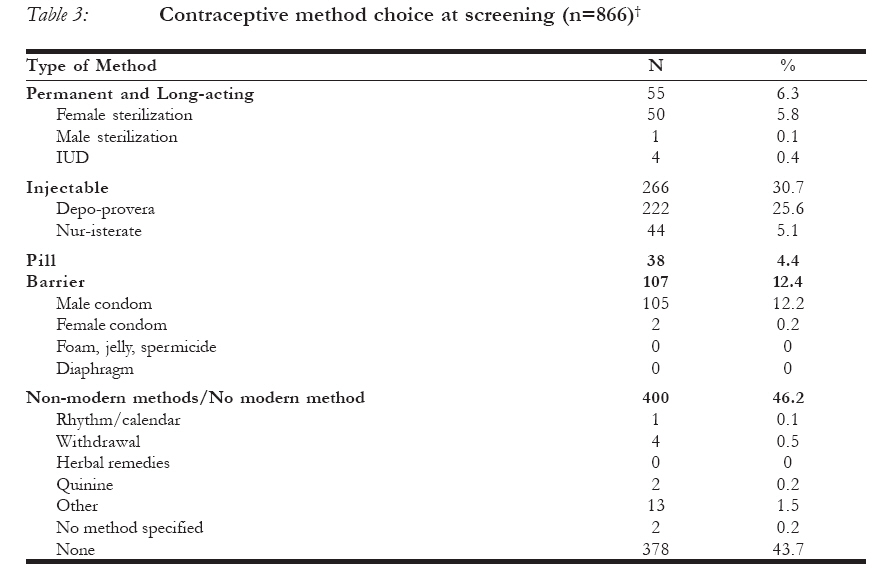
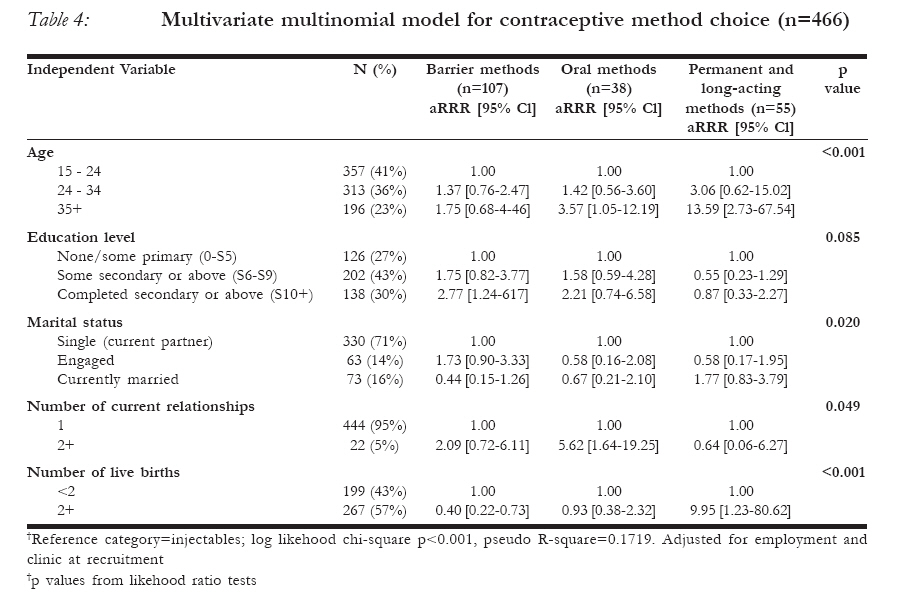
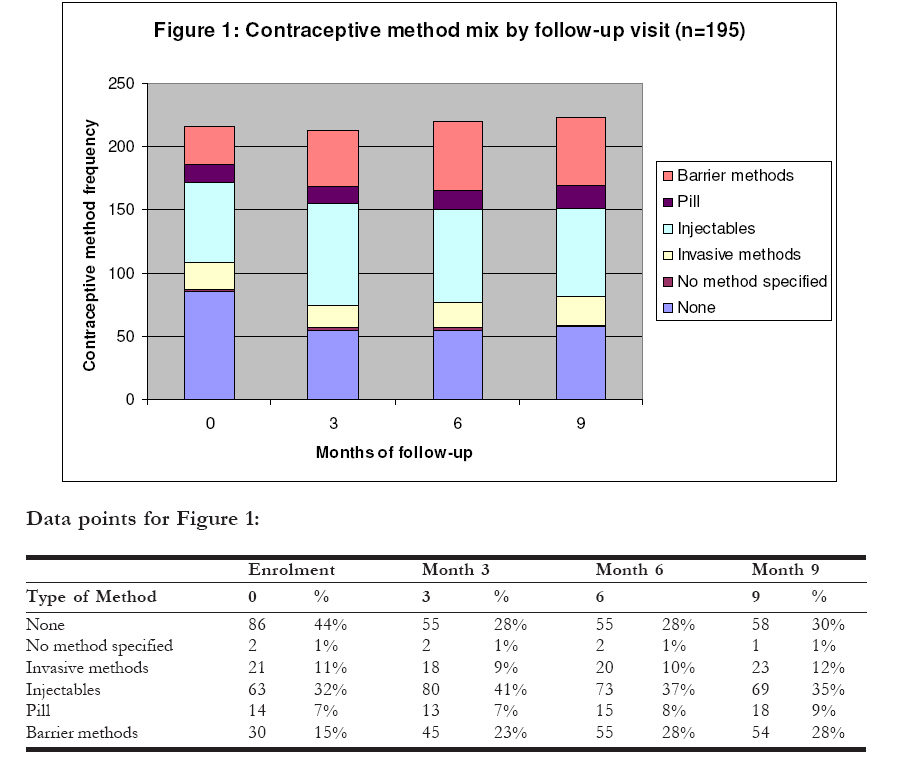
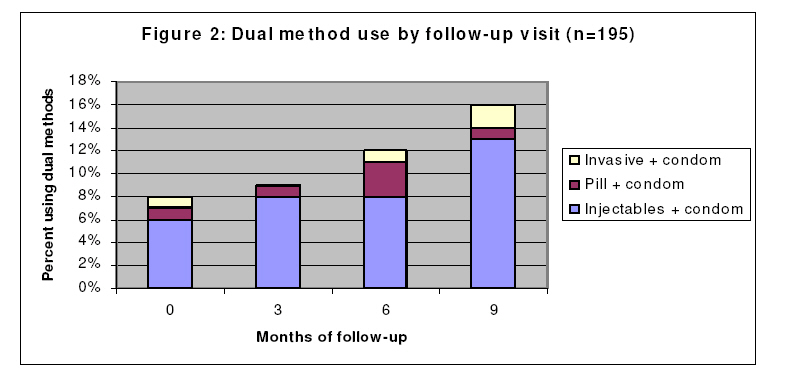
Women who spontaneously reported 2 or more contraceptive methods were assigned a primary method based on method effectiveness and reversibility21. Primary contraceptive method was defined as the most effective/permanent of reported methods (e.g. a woman using both injectables and condoms was classified as using injectables for her primary contraceptive method). Women who spontaneously reported one method and then reported a second method when probed were assigned the spontaneous method. On analysis, the spontaneous methods reported were also the most effective/permanent reported method in each case. Independent variables Variables for education, employment, food expenditure and household characteristics were used as proxies for socioeconomic status. Highest education level obtained was categorized in accordance with South African school levels: none/less than one year, primary (CLA-S5), some secondary (S6-S9), and completed secondary or above (diploma, bachelors, honors and masters were combined due to small numbers of women with higher degrees).2 Current employment was categorized as none or parttime/full-time, and was included in all multivariable analyses due to its importance in prior studies. Access to electricity, quality housing materials (roof of tile or corrugated iron, walls of cement or brick), toilet type (flush vs. other), water source (piped vs. collected), quality fuel source (gas or electric vs. other), expenditures on bread per person per month, and number of people (adults + children) per room in household were considered as potential proxies for household financial resources. The role of urban residence, defined as residing in a formally designated urban township, on contraceptive use was also investigated. Age, marital status (single, engaged, married) and cohabitation, number of current relationships, number of live births (0, 1, 23, 4+), previous HIV testing/ receipt of results, and religious affiliation (international churches, African Independent Churches, Nazareth Baptist and other) were also considered. The three clinics where recruitment occurred were included in all multivariable analyses as they varied in physical location, urban/rural area, and service provision. Changes in contraceptive use To evaluate longitudinal changes in modern contraceptive use, we investigated contraceptive practices among enrolled women who attended month 3, 6 and 9 follow-up visits (study closure and attrition led to a minority of participants completing a month 12 visit). Modern contraceptive use was defined as above. Analysis Data were entered into EpiInfo622 and exported to Stata v.823 for cleaning and analysis. We calculated descriptive statistics for 866 screened women (from 886 women, we excluded 1 with missing baseline data on current contraceptive use, 1 with inconclusive data on HIV serostatus, 2 intending pregnancy in the next year, 12 pregnant at screening, and 4 reporting no sexual partner). We examined univariable relationships between independent variables and contraceptive use/method choice using chisquare tests for categorical variables and unpaired t tests/ANOVA for continuous variables. Among 866 screened women with data on contraceptive use, we used multivariable logistic regression to evaluate predictors of contraceptive use, and multinomial logistic regression to investigate on contraceptive use. However, due to small predictors of method choice (using sample sizes, we categorized age in three injectables as the reference category). groups (15-24, 25-34, 35+) and included as Contraceptive use did not differ among indicators in regression models, and used a women with primary education (n=187) dichotomous measure of parity (<2, 2+ versus no education (n=86), so these groups births) for analyses of method choice. We were combined for multivariable models. explored interactions between marriage, Initially, five-year age categories were used cohabitation, age and parity in predicting to capture the non-linear influence of age contraceptive use but had limited statistical 2This study was conducted prior to recent restructuring of the South African education levels. The categories reflect the 2003 South African education levels for primary and secondary schooling. †Residence, religious affilitation, household variables (size, electricity, quality housing materials, flush toilet, piped water source) and number of current relationships had no univariate significance *P values from chi-square for categorical variables, unpaired t-test for continuous variables power to detect significant effects in We calculated descriptive statistics to multivariable models. As exclusion of determine if women included in our employment status from multivariate models longitudinal sample differed significantly did not change the direction or strength of from the population who were screened for association for other predictors, we kept the study, as well as enrolled women excluded employment status in the model for due to visit attendance. We then analyzed comparability with prior studies. changes in contraceptive use using chi-square tests for trend among 195 women with data on contraceptive use at enrolment, 3, 6 and 9-month time points. Results Table 1 presents baseline demographics significant in univariate analyses for the 866 women who met inclusion criteria for these analyses. Women were a mean age of 28.2 years (median 26, range 15-54), and 75% lived in rural areas. Approximately half of screened women were receiving a government grant for child support, and 87% described their financial status as “just getting by” or “poor.” Eighty percent of women reported ever using modern contraceptives, most commonly injectables (68%), barrier methods (26%), pill (16%) and sterilization (6%). Average age at first contraceptive use was approximately 21 years (range 11-42). Perception of HIV risk was high (not shown in table); 92% of women reported themselves at risk of contracting HIV, most because of unfaithful partners (81%) and non-use of condoms (83%). Only 14% of women reported being currently married, of whom 70% reported cohabiting with their husbands. Twenty-eight percent of unmarried women and 28% of unmarried women reported cohabiting with their partners. These rates of marriage and cohabitation are compatible with other findings in the area24. Predictors of contraceptive use Of 866 women with data on current contracep-tive use at screening, 466 (54%) reported currently using modern contraceptives. Results of univariable and multivariable logistic regression analyses regarding the relationship between independent variables and modern contraceptive use are shown in Table 2. Age, education level, employment, quality fuel source, expenditure on bread per person per month, marital status, parity and HIV testing history were significantly associated with contraceptive use in univariable analyses. A multivariable model with age, parity and marital status indicated statistically significantly higher contraceptive use among engaged vs. unmarried women (aOR 1.68), younger (under 30) vs. older women (aOR 1.61), and women with a history of 2 or more births vs. nulliparous/primiparous women (aOR 1.47). Analyses of marital status and cohabitation suggested increased contraceptive use among engaged and married individuals only if they were also cohabiting with their partner. However, due to insufficient power we modeled age, parity and marital status separately in multivariable analyses. Multivariable analysis revealed significant differences in contraceptive use according to age (p=0.008) and clinic (p<0.001) (Table 2). Women with some secondary education or who had completed secondary schooling had significantly increased odds of contraceptive use compared to those with primary education or less (aOR 1.54 and 1.64, respectively). Multivariable analysis also showed significantly higher odds of contraceptive use among employed women compared to those with no current employment (aOR 1.65). Bread expenditure greater than R21 pp/pm (aOR 1.58) and quality fuel source (aOR 1.49) were both significantly associated with increased contraceptive use. Married women had 1.64 greater odds of using contraceptives than single women, while engaged women did not differ significantly in contraceptive use from single women. We observed a significant increasing gradient in contraceptive use among women with 1 live birth, 2-3 live births and 4 or more live births compared to women with no live births (p<0.001). Compared to women who had never tested for HIV, prior HIV testing without receipt of results was associated with significantly lower contraceptive use (aOR 0.53). Predictors of contraceptive method choice Injectables were the most common contraceptive method among screened women, with 31% reporting current use as a primary method (Table 3). Women also reported using condoms (12%) sterilization (6%) and pills (4%) as primary contraceptive methods. Seventy-five women (9%) reported concurrent use of condoms and injectables, pill or sterilization. No women reported using implants or IUDs. Of the demographic characteristics available, age, clinic at recruitment, education level, piped water source, marital status, cohabitation, number of current relationships and parity were significantly associated with contraceptive method choice in univariable multinomial analyses. Multivariable analyses showed that women aged 35+ were significantly more likely to use oral methods (aRRR 3.57) and invasive methods (aRRR 13.59) than injectables (Table 4). Having a secondary education was significantly associated with the choice of a barrier method rather than injectables (aRRR 4.58). Having 2 or more live births significantly decreased barrier use (aRRR 0.40) and increased invasive method use (aRRR 9.95) compared to injectables. Marital status was an important variable in the model (LRT p-value<0.05) but was not significantly associated with any particular method, and the individual estimates suggest no clear pattern between marital status and method choice. This observation remained consistent in models with unmarried and engaged women considered separately and jointly. Women in 2+ relationships were much more likely to use oral methods than injectables (aRRR 5.62), although the sample size was quite small (n=46). Cohabitation and piped water source were insignificant in multivariable analyses and were excluded from the final model for the sake of parsimony. Changes in contraceptive use over time Of 886 women screened for the Microbicide Feasibility Study, 449 were enrolled. The drop in sample size between screening and enrolment was due to random invitation (according to HIV status) to enroll in the study and this would not be expected to introduce any bias in the sample with regard to contraceptive use. Of the 449 enrolled women in the Microbicide Feasibility Study, 73% (n= 328) returned for a week 2 visit. This loss to follow-up is most likely a result of women enrolling on the same day as screening and then re-thinking their decision, unrelated to contraceptive use. Contraceptive use was measured at enrolment and 3, 6 and 9-month time points. Of the women who returned after enrolment, 59% (n=195) had complete data on contraceptive use at 3, 6 and 9-month time points. The remaining women missed at least 1 visit and/or were censored prior to their 9 month visit due to study closure. The sample used for longitudinal analyses differed in certain characteristics compared to the 436 women screened but not enrolled in the study, and the 254 enrolled women who did not complete 3, 6 and 9month visits. The median age differed slightly across these groups (27, 24 and 27 respectively, p=0.002). There were fewer married women in the screened and enrolled groups compared to the longitudinal group (11%, 15% and 22% respectively, p=0.006), and distribution of clinic at recruitment differed across groups (p<0.001). However, the groups did not differ significantly in residence, grant receipt, education, religion, employment, household size, number of relationships or parity (all p>0.10). There were no statistically significant differences in contraceptive use among women attending 2 or fewer visits vs. women included in the longitudinal sample (p=0.387 at enrolment; p=0.073 at month 3; p=0.371 at month 6; and p=0.136 at month 9). At enrolment, 109 (56%) of the 195 women reported using a modern method of contracep-tion. Contraceptive use rose significantly to 72% at month 3 and remained stable through 9 months. Of the 109 women who reported using modern contraceptives at enrolment, 88 (81%) reported contraceptive use at every visit, 14 (13%) reported intermittent contraceptive use, and 7 (6%) did not report modern contraceptive use at any point during follow-up. Among 86 women not using modern contraceptives at enrolment, 58 (67%) reported using contraceptives at least once during followup, twenty-eight (48%) of whom reported using modern contraceptives at every follow-up visit. Contraceptive method choice varied throughout the study (Figure 1). Injectables (specifically DMPA) were the most common contraceptive method among women in our sample, reaching a high of 41% use at month 3 and remaining relatively constant thereafter. The significant increase in women using modern contraceptives from enrolment to month 3 (p=0.001) was primarily due to increased use of condoms (15% to 22%) and injectables (31% to 41%). The women who contributed to this initial increase were more likely to have completed some secondary education (p=0.04), but did not differ significantly in age, marital status or employment. After the initial significant increase at month 3, condom use increased again at month 6 (22% to 28%, p<0.001), then remained constant. Changes in use of invasive methods and pills from enrolment to month 9 were not significant. Dual method use (primarily injectables + condoms) increased from 8% at enrolment to 13% at study conclusion, albeit nonsignificantly (Figure 2). Very few women reported using traditional methods of contraception (rhythm/calendar, withdrawal, herbal remedies, Quinine), with use of these methods ranging from 1-2% throughout the study. In an additional sexual behavior question-naire, 31 women reported condom use during the study but not as a family planning method. Of the women contributing to the increase in condom use at month 3 (n=27), 50% had reported using a family planning method at screening. Of these existing users, 63% reported using condoms in addition to their existing method at month 3. Of women not previously reporting family planning use, the majority (86%) reported using only condoms at month 3. Seven of 195 women became pregnant during the study, none of whom reported intending pregnancy at any previous visits. Six women were not using modern contraceptives when they became pregnant (one woman was using injectables), although four reported contraceptive use at previous visits. The pregnancies were distributed evenly throughout the study, with no clustering by visit. Of 96 women with information on family planning decisionmaking at each follow-up visit, 31 (32%) reported always making their own decisions about family planning, 8 (8%) always decided together with their partner, and 57 (59%) reported a combination of the two approaches across visits. Only 1 woman consistently reported that her partner was the primary decision-maker regarding family planning. In general, differences in contraceptive use according to decisionmaking roles were not significant. Discussion Only half of a sexually active female study population in rural KwaZulu-Natal who declared no immediate pregnancy intentions reported currently using a modern contraceptive method. Among women using contraceptives, injectables were the preferred method and use of dual methods to protect against pregnancy and sexually transmitted infections was low. Nearly all screened women perceived themselves to be at risk of HIV infection, but only 9% reported use of condoms with injectables, pills or sterilization. These results are consistent with data from SADHS, and indicate the need for increased emphasis on dual protection from pregnancy and STIs in rural KwaZulu-Natal, where HIV incidence remains high25. Age, education, employment, household characteristics, marital status, and parity were significant independent predictors of increased modern contraceptive use among sexually active women in rural KwaZulu-Natal. In addition, age, education, marital status, parity and number of current relationships were associated with contraceptive method choice. We observed low contraceptive use among 15-19 year olds, increased use during the 20’s and 30’s, and a drop in use after age 40. These findings mirror fertility trends in KwaZulu-Natal, where many women have their first child in their teens and initiate modern contraceptive use in their early twenties10, and concur with estimates of contraceptive use among other South African women9. The effect of age differs by contracep-tive method, with women aged 35+ significantly more likely to use oral and invasive methods than injectables. This finding may reflect increased popularity of injectables among younger women and/or a shift with age to more permanent methods. This difference in method choice may also be related to parity, which was highly correlated with contraceptive use (particularly invasive methods) in our analyses as well as prior studies in South Africa9 26 27 and in other African settings5-7 28 29. Marital status may also play a role in the use of more permanent contraceptive methods; although not statistically significant, engaged women in our sample were more likely to use barrier methods and married sex education were unlikely to be included women to use invasive methods. We found in the curriculum. Therefore completion of that overall, married women had significantly secondary education may be a surrogate for higher odds of using modern contraceptives health literacy in terms of receptiveness to than engaged and unmarried women, corres-public health campaigns, and/or ability to ponding to findings from prior studies5 26 28 30. access contraceptive/condom service Married women may be likely to be having providers. sex more regularly than unmarried women31, Employment, which was also associated which may explain their higher contraceptive with an increased likelihood of contracepuse. Cohabitation status alone was not a tive use, may suggest equality with partners significant multivariable predictor of enabling negotiation of contraceptive use.36 contraceptive use. However, cohabitation The relationship between employment and may influence contraceptive practices in contraceptive use may also be endogenous combination with marital status; univariable rather than predictive; i.e., contraceptive use analyses suggested increased contraceptive prevents pregnancy and subsequent childcare use among engaged and married women responsibilities, enabling women to seek living with their partners compared to non-employment. However, this may not be the cohabiting unmarried women. In addition, case in rural South Africa, where extended age, parity and marital status may interact family structures for childcare may enable to influence contraceptive use. Models of women to return to their jobs shortly after these interactions were limited by small giving birth. Given that exclusion of sample sizes, but unadjusted results employment status from multivariate models suggested higher contraceptive use among did not change the direction or strength of older engaged/married women with multiple association for other predictors, we kept this births than among younger unmarried variable in the model for comparability with women with no children. prior studies28,29,37. Expenditure on bread Measures of socioeconomic status greater than R21 (approximately US $3) per (education, employment, assets) have person per month and having a quality fuel previously been linked to contraceptive use source were also significant predictors of and method choice in South Africa9 26 32 and increased contraceptive use. Contraceptives in other African countries5 7 8 26 28 29 33. In are available for free in South Africa, so these particular, use of dual methods to protect indicators of household financial resources against pregnancy and STIs in South Africa may represent increased freedom in has been linked to increased schooling34 35. reproductive decision-making and access We observed a higher likelihood of (particularly transport) to family planning contraceptive use with increasing education services. level, and noted that women who had We controlled for clinic at recruitment completed secondary education were in multivariable analyses and found it to be significantly more likely to use barrier a significant predictor of contraceptive use methods. At the time of schooling for the and method choice. This may be due to more majority of this cohort, life skills and safer frequent provision of family planning services at one clinic (daily as opposed to weekly), as well as different mixes of clientele at the study clinics. Prior HIV testing without receipt of results was associated with lower odds of contraceptive use. Given that only 7% of women were in this category, this finding may be due to chance. Nonetheless it highlights the importance of distinguishing between prior testing with results versus without results in future analyses, and indicates a need for further investigation into the impact of HIV testing and result collection on contraceptive use. Also of note is the non-significant role of urban residence and religion in our analyses. Due to the largely rural composition of our sample, we defined urban residence as residing in a peri-urban township, which may not reflect the effects of urban living previously identified in South African settings9 26. Religious affiliation and contraceptive practices have been investigated in other African countries with conflicting results 5 8 which was why we considered it in our analyses. Religious affiliation with different churches (categorized as international churches, African Independent Churches, Nazareth Baptist and other) was not a significant factor in multivariate analyses of contraceptive use or method choice. Religious affiliation was virtually universal in our sample so may have had similar baseline influence on contraceptive use. Alternatively, women may not have been strict followers of religious doctrines regarding contraception. Longitudinal analyses of modern contracep-tive use among women enrolled in the Microbicide Feasibility Study indicated that contraceptive use increased significantly during the first three months of the study, African Journal of Reproductive Health Vol. 12 No.2 August, 2008 then remained steady. Most women who reported using contraceptives at enrolment remained consistent users throughout the study, and almost 70% of baseline non-users reported using contraceptives at least once during follow-up. These results suggest that regular discussions about family planning and safer sex counseling in microbicide clinical trials may achieve significant increases in contraceptive use, especially condom use. However, there is no control group against which to explore this further. In addition, there is the possibility that some of the reported increase reflects social desirability bias given the messages promoted by study staff, but we believe that this is minimal given that reported non use of contraception was common. In a population where most women had a need for contraception (women intending pregnancy were excluded from enrolment), 14% of women never used modern contraceptives during the study, and 7 women became pregnant. None of the women who became pregnant were intending to do so (according to report at the previous visit), and most were not using contraceptives when they became pregnant. This indicates that even with repeated counseling, some women will be unable or unwilling to use family planning despite their desire to avoid pregnancy. Increased condom use during the Microbicide Feasibility Study may suggest that repeated safer sex counseling improves awareness of condoms as a dual protection method against HIV and pregnancy. However, interpretation of these results is limited by the lack of a control group for comparison. Approximately half of new condom users at month 3 had not reported using family planning at screening, indicating that part of the initial increase in condom use may have been for pregnancy prevention purposes. In fact, recent evidence indicates that condom use for pregnancy prevention has increased in sub-Saharan Africa38 and is becoming more common among South African youth35. Some women reported condom use during sex acts but not for pregnancy prevention, and a number of new condom users also reported concurrent use of an effective contraceptive method. This may reflect increased use of condoms for HIV/STI prevention, or may indicate social desirability bias in response to messages regarding safer sex at previous visits. We observed high levels of reported autonomy and partner cooperation regarding family planning decision making among women enrolled in the study. These findings correspond with prior studies regarding the influence of male partner’s approval of family planning5 7 29, gender roles and dynamics on women’s ability to negotiate contraceptive use in South Africa39 and in KwaZulu-Natal in particular40. Limitations and future directions Women were recruited from family planning and immunization clinics for the microbicide feasibility study, so may be more likely to use modern contraceptives than the general population. Our sample also included a large proportion of unemployed women, since our clinics were primarily open during working hours. However, unemployment prevalence in the microbicide feasibility study (67%) is comparable to unemployment among African women aged 15-65 in KwaZulu-Natal (62%)41. Our study collected detailed demographic data for screened women but did not collect in-depth sexual behavior data until after enrolment. Consequently, our analyses of contraceptive predictors do not include variables such as frequency and type of sex. In addition, we did not collect information on perceived quality of family planning services. Prior studies indicate that quality of care and provider attitudes significantly influence use of family planning services42 43 and likelihood of subsequent contraceptive use. Future studies of contraceptive use could benefit from more detailed information regarding quality of care as well as qualitative information on how women make contraceptive choices. Only 9% of screened women in our study using a highly effective contraceptive method like sterilization or injectables also reported using condoms. This finding corresponds to prior work in South Africa indicating approximately 12% use of dual methods44. The increase in dual method use among enrolled women throughout our study is encouraging, and the results suggest the need for further integration of family planning services and safer sex counseling in order to promote dual method use as a standard of care in rural KwaZulu-Natal45. Our analysis of changes in contraceptive use throughout the microbicide feasibility study was limited to approximately half of enrolled women. Women in our longitudinal sample were older and more likely to be married than all enrolled women, so our estimates of changes in contraceptive use may reflect biases due to irregular clinic attendance and attrition from the study. While our results may over-emphasize the impact of regular family planning discussions and safer sex counseling on increased contraceptive usage, the longitudinal analyses provide a useful picture of the potential changes in contraceptive use that can be achieved among a cohort of sexually active women over a 9 month period. Acknowledgements We would like to thank the Africa Centre Microbicide clinic, field and data centre staff, and the community for their contributions and support. The microbicide feasibility study was coordinated by the Microbicides Development Programme (MDP); we would like to thank the MDP team for their contribution and support. The microbicide study was funded by the United Kingdom Department for International Development (DfID) and the United Kingdom Medical Research Council (MRC). We would like to acknowledge their contribution to the study. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08022t3.jpg] [rh08022f1.jpg] [rh08022t4.jpg] [rh08022t2.jpg] [rh08022t1.jpg] [rh08022f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}