 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
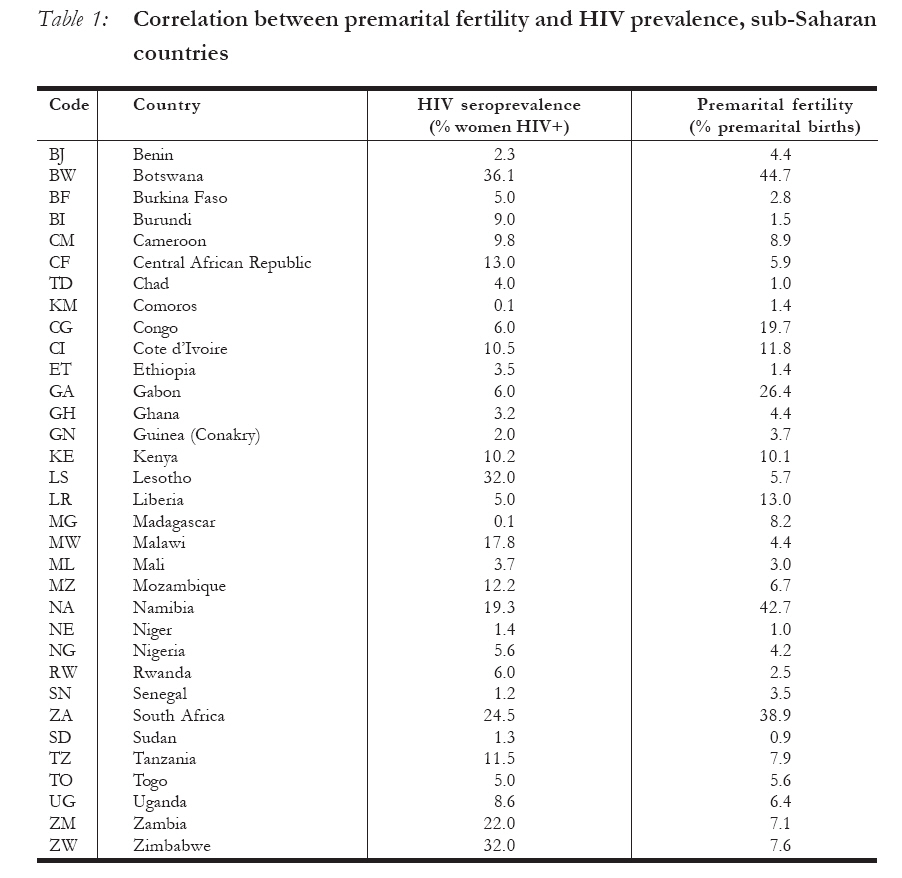
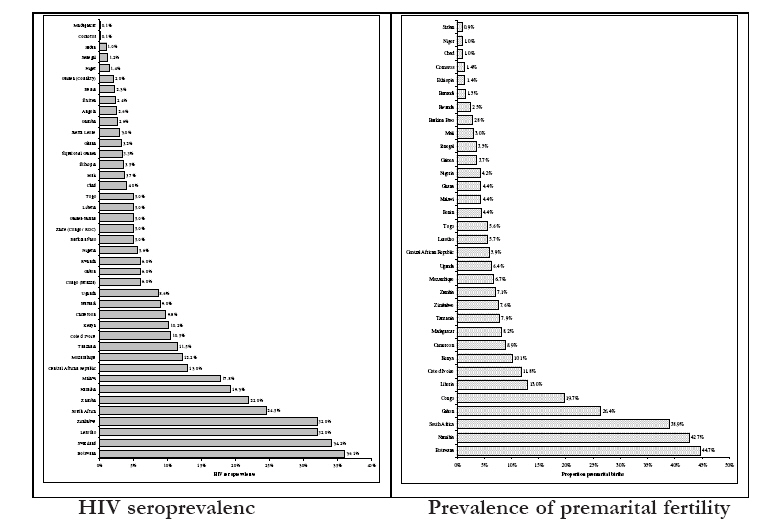
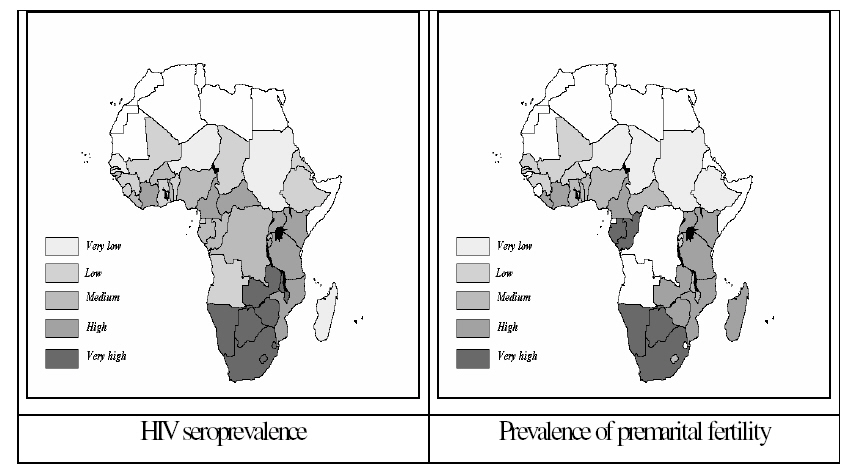
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 64-74 Premarital fertility and HIV/AIDS in sub-Saharan Africa Fécondité avant le mariage et le VIH/SIDA en Afrique Michel Garenne1, Julien Zwang2 1Directeur de Recherche, IRD/ISD and Institut Pasteur, Paris 2Research Associate, Shoklo Malaria Research Unit, Wellcome Trust - Mahidol University, Oxford Tropical Medicine Research Programme, Maesod, Thailand Code Number: rh08023 ABSTRACT The paper investigates the complex relationships between premarital fertility and HIV/AIDS in sub-Saharan African countries. The DHS surveys provided data to compute the prevalence of premarital fertility, defined as any birth before the first marriage. The UNAIDS database provided data to compute the prevalence of HIV infection among pregnant women. Results indicate a moderate association between the prevalence of premarital fertility and the prevalence of HIV infection (correlation coefficient = 0.64, P< 0.0001), and similar geographical patterns. Compared with the average pattern, outlier countries had either high levels of premarital fertility and relatively low HIV prevalence (Liberia, Madagascar, Gabon, Congo), or high levels of HIV prevalence despite low levels of premarital fertility (Lesotho, Malawi, Zambia, Zimbabwe). The overall relationship is discussed in light of the relationships between age at marriage, permissiveness and lack of protection during intercourse and their impact on premarital fertility and HIV infection among women. KEY WORDS: Premarital fertility, Adolescent fertility, HIV-AIDS, Sexual behaviour, Contraception, sub-Saharan Africa. RÉSUMÉ Cet article étudie les rapports complexes entre la fécondité avant le mariage et le VIH/SIDA dans les pays africains sub-sahariens. Les enquêtes menées par les WFS et DHs ont fourni les données initiales pour évaluer la prévalence de la fécondité avant le mariage. On a défini la fécondité avant le mariage comme toute naissance avant le premier mariage. La prévalence de la fécondité avant le mariage a été évaluée comme étant la proportion des femmes fécondes qui sont âgées de 25 ans et plus qui ont eu une naissance antérieure avant leur premier mariage. La base de données du Bureau de Recensement a fourni les données qui ont permis d´ évaluer la prévalence de l´ infection du VIH chez les femmes enceintes. On s’est servi d´ un simple modèle pour normaliser les tendances dans la séro-prévalence du VIH et pour évaluer la séro-prévalence moyenne au cours de la période 1995 – 1999. Les résultats ont montré un lien modéré entre la prévalence de la fécondité avant le mariage et la prévalence de l´ infection du VIH (le coefficient de corrélation = 0,37, P=0, 04). Par rapport aux tendances globales, certains pays africains avaient soit des niveaux plus élevés de la fécondité avant le mariage et une prévalence relativement peu élevée basse du VIH (Libéria, Madagascar) ou bien le modèle opposé, cést-à-dire des niveaux élevés de la prévalence du VIH malgré les niveaux bas de la fécondité avant le mariage (Ethiopie, Rwanda). Le rapport global a été discuté à la lumière du rapport entre la permissivité et le manque de protection au cours des rapports sexuels et son impact possible sur à la fois la fécondité avant le mariage et l´ infection précose du VIH chez les femmes. Les cas des pays comme le Libéria et le Madagascar ont été discutés à la lumière des dynamiques qui sous-tendent le modèle de la fécondité avant le mariage et les dynamiques de l´ épidémie du VIH dans des pays particuliers. Introduction The HIV (Human Immunodeficiency Virus) epidemic emerged in the 1970’s, probably somewhere in Central Africa. Its origin is still a matter of academic debate.1 The disease was unknown prior to its identification in the United States in 1981, and the earliest record of an AIDS death goes back to 1959. AIDS soon emerged as a major cause of death in African populations in the mid 1980’s, and since then the epidemic has been raging in large parts of sub-Saharan Africa, and much faster than any other part of the world.2 Many questions are raised by the rapid spread of the disease. If core groups such as commercial sex workers (CSW’s) played a significant role in the early spread of the disease, their role soon became shadowed by other dynamics.3 When the epidemic became “generalised” in the 1990’s, that is when the level of seroprevalence became high in the general population, other dynamics appeared and in particular the disease spread rapidly among young female adults who had no obvious risk factor.4 Among the questions raised by the rapid spread of the disease among young women are the patterns of sexual partnership and the lack of protection from sexually transmitted diseases (STD’s) during intercourse. About twenty years after the identification of the disease and the understanding of its sexual transmission, it is striking to note that we poorly understand why large parts of the population, and in particular young women, get infected so quickly. This rapid spread of HIV among young women reveals first an intense exposure and second a lack of protection. This seems to occur throughout Africa, though with different intensity, despite widespread knowledge of disease transmission and ways to prevent it, as shown by numerous surveys, and in particular the Demographic and Health Surveys (DHS). If young women have frequent and unprotected intercourse, not only do they get infected, but they also become pregnant, unless they use efficient contraceptive methods other than condoms. Various studies on developing countries have addressed the issue of adolescent fertility in a demographic perspective.5-8 More and more in Africa, the first pregnancy occurs before the first marriage, primarily because age at marriage tends to rise, as in many developed countries of Europe and North America. As a consequence, large numbers of women now experience premarital fertility, as exemplified by case studies in Southern Africa.9-12 In earlier periods, most African women were married early, and had their first births within marriage, though there were cases of premarital births in numerous ethnic groups throughout continental Africa as well as in Madagascar. In modern Africa, one can therefore expect a statistical relationship between prevalence of premarital fertility and prevalence of STD’s, and in particular HIV, since both phenomenon have the same rationale: unprotected intercourse in teenage years. Of course, the relationship is by no means likely to be a one to one relationship since many divergent situations may happen and many other factors interplay. For instance, premarital intercourse with a regular partner who will become a husband is unlikely to bear a higher risk of contracting STD’s than with a formal husband; similarly, premarital intercourse with multiple partners will not lead to infection if they are not infected; obviously intercourse with an infected husband is likely to lead to an infection; hormonal contraception has a strong effect on the risk of pregnancy, but does not decrease the risk of contracting STD’s. Lastly, STD’s have their own dynamics, and unless a germ is circulating in a population being a priori at risk does not lead to infection. Several papers have discussed the underlying factors of premarital fertility or HIV infections among young African 13-22 women. A recent review summarizes critical points and major social factors of unsafe sexual behaviour of young adults. 23 Authors categorize factors in three levels: individual, interpersonal (proximal), and societal (distal), and discuss the theoretical and practical issues around risk taking in sexual behaviour in a gender perspective. They cover most known factors which could explain levels of premarital fertility or prevalence of HIV and STD’s, though they seldom address the issue of marriage and stable relationships in a cultural perspective. In any case, the main point of interest for our analysis is that most factors of unsafe sexual behaviour, from gender imbalance to peer pressure, are likely to play a similar role for premarital fertility and HIV prevalence, unless other factors interact, such as modern methods of family planning other than condoms. Furthermore, these relationships may be compounded by other socioeconomic factors, such as urbanization and poverty. The aim of this paper is to investigate the statistical relationship between premarital fertility and HIV prevalence in sub-Saharan Africa countries. This will be done at the country level, trying to understand the possible relationships between the two variables. In fact, as it will be seen below, there are major differences in both the prevalence of HIV/AIDS and the prevalence of premarital fertility among African countries. Some of these differences could be due to socio-demographic factors, such as early versus late marriage, and social control versus permissiveness of the society. These two factors are likely to have an effect on both premarital fertility and HIV prevalence, though may be confounded by other factors, such as other forms of contraception and unexpected dynamics of HIV epidemics. This study is part of a more comprehensive study on premarital fertility in Africa undertaken by the same authors, and supported by the Wellcome Trust. Data and methods Premarital fertility Premarital fertility is defined here as any birth prior to the first marriage. Several indicators of premarital fertility could be used for estimating its prevalence in the population. In this study, we have chosen to use the proportion of premarital births among all births recorded at time of survey. Data were derived from the World Fertility Surveys (WFS) and the Demographic and Health Surveys (DHS) in sub-Saharan Africa. The prevalence of premarital fertility could be computed directly and simply from the files by matching date of first marriage and date of birth. The prevalence of premarital fertility could also be easily computed for cohorts of women or children, and for selected socioeconomic characteristics, such as urban residence, ethnic group and others. A total of 88 surveys were used in the analysis. When several surveys were taken in the same country, the results were merged by adding numerators and denominators to produce a single estimate. A total of 33 countries are covered in this sample (see list of countries in Table 1). HIV prevalence HIV prevalence was estimated by reconstructing the dynamics of the prevalence of HIV from seroprevalence surveys taken in sentinel sites among pregnant women, and calibrated with HIV seroprevalence surveys whenever possible. The database used for these calculations was provided by the US Census Bureau data base for data prior to 2000, and by the UNAIDS database for the recent years. These databases cover comprehensively published and unpublished estimates of seroprevalence in a large number of African countries. The database is somewhat heterogeneous, since in many countries only sporadic estimates are provided, and not yearly estimates, and from selected clinics, and not from a proper random sample of pregnant women. The best estimate around year 2000 was taken as the reference value, which corresponds to a peak of HIV seroprevalence in most countries, or values close to the peak for the others. Results Premarital fertility In the sample of countries studied, the prevalence of premarital fertility varied from very low values, such as 1.0% in Niger and Chad, to very high values, such as 38.9% in South Africa, 42.7% in Namibia and 44.7% in Botswana, with an average value of 9.6% of premarital births (Table 1, Figure 1). This indicates the magnitude of the risks for young women, and the wide range of variations between countries. A marked geographical pattern of differences in premarital fertility could be seen. Premarital fertility was very high in countries of Southern Africa (South Africa, Botswana, and Namibia), and Central Africa (Congo, Gabon), primarily because of high median age at first marriage. Premarital fertility was also high in most Eastern African countries as well as in Madagascar. Premarital fertility was particularly low in Sahelian countries, from Senegal, Niger, Chad to Northern Sudan and Ethiopia, for the opposite reason, that is low median age at first marriage. Other countries of Coastal Western Africa and Central Africa tended to have medium levels. There were some exceptions to this broad geographic pattern. In West Africa, Liberia, Côte d’Ivoire and Cameroon had higher levels than their neighbouring countries. In Central Africa, Rwanda and Burundi had lower levels than their neighbouring countries despite relatively high age at first marriage. HIV seroprevalence among pregnant women A marked gradient in HIV seroprevalence, of similar magnitude, could also be seen in the sample of countries available, from very low values: 0.1% (Madagascar), 1% (Sudan), 1.2% Senegal, 1,4% (Niger) to very high values: 32% (Zimbabwe, Lesotho), 34.2% (Swaziland), 36.1% (Botswana), with an average value of 10.0% (Table 1, Figure 1). As for premarital fertility, there was also a geographical pattern, with some similarities with the previous pattern (Figure 2). The prevalence of HIV among pregnant women was very high in the Southern Africa band going from Zambia to South Africa, high in Eastern Africa, low to very low in most Sahelian West Africa, and medium in several Coastal West African as well as in the Central African Republic. Note that the geographical patterns of high and low prevalence of premarital fertility and HIV prevalence were quite similar. Correlation between premarital fertility and HIV seroprevalence Plotting HIV seroprevalence against premarital fertility revealed a pattern (Table 1). The correlation coefficient based on the 33 countries was 0.643 (P= 0.00005), showing the effect of common underlying factors of the two variables. About half the countries fitted the pattern, from low values (Burundi, Rwanda, Mali, Burkina Faso, Central African Republic), to medium values (Tanzania, Uganda, Kenya, Cameroon, Côte d’Ivoire), and to high values (Botswana, Namibia, South Africa). Other countries were located far away from the regression line, either above or below. Several patterns of outliers could be identified:
The pattern of relationships between premarital fertility and HIV prevalence, as well as the differences from this pattern could be related to a number of external factors. Firstly, very traditional countries with repressive norms on sexual behaviour (e.g. Muslim countries and some Christian countries) tended to have an earlier age at marriage, lower levels of premarital fertility and lower levels of HIV prevalence. Secondly, more urbanized and more industrialized countries, in particular the mining countries tended to have the opposite pattern, of later marriage and more permissive attitudes towards sexual behaviour, and more HIV. Thirdly, countries affected by migration to- and from- poles of development (such as South Africa or to a lesser extent Côte d’Ivoire) could be more exposed to HIV than they would have been otherwise. Fourthly, some countries may be particularly isolated because of their geographical location (Madagascar, Comoro Islands) or because of poor economic resources or of political isolation. Another factor could possibly complicate the picture, and act as a confounder: modern contraception. Modern contraceptive methods among young women, and primarily Depo-Provera in Eastern and Southern Africa, could strongly reduce the risk of pregnancy of exposed women but not reduce the risk of contracting HIV and other STD’s. We tried to investigate this relationship, however we failed because of reverse causality: the higher the level of premarital fertility the higher also was the prevalence of modern contraception. This could easily be explained since more exposure to unwanted pregnancy prior to the first marriage increases at the same time the level of premarital fertility and the motivations for contraception. In our sample, the correlation was high between contraceptive prevalence among unmarried women age 1524 and premarital fertility by age 25 (coefficient of correlation = 0.70), as well as with the prevalence of HIV/AIDS (r= 0.61), so that we could not run any multivariate analysis including at the same time premarital fertility and contraceptive prevalence. Discussion A number of patterns emerged from this analysis. A sticking observation was the wide heterogeneity between countries, from low to high levels of both premarital fertility and HIV infection. Sub-Saharan Africa is very heterogeneous in many respects: a large number of ethnic groups, with some 2000 groups on record; a wide variety of social norms, from permissive to repressive, well documented in the ethnographic literature; many religions, in particular various forms of Islam and of Christian religions who have reshaped traditional norms, not counting numerous traditional religions; a wide variety of situations in socio-economic development (income, education, urbanization), as well as in access and use of public health services, in particular in preventive policies for HIV and unwanted pregnancy. All these factors may explain the wide variations in outcomes such as premarital fertility and HIV infection, and the erratic patterns seen in some countries. The rationale for the correlation between premarital fertility and HIV infection seems to be straightforward. Many HIV infections among women occur at an early age, prior to age 25, and probably many occur prior to first marriage, and indicate unprotected intercourse. A micro-simulation model currently under development by us and aiming at reproducing age patterns of HIV infections suggests that a majority of infections indeed occur during casual intercourse prior to first marriage. Even if this is only one marker of the many risks involved, premarital fertility appears as an important correlate of HIV infection among young women, and of the dynamics of HIV epidemics. The effect of high social control on sexual behaviour could be observed in traditional countries of Sahelian Africa (many of them primarily Muslim), with low income levels, where age at marriage is low and most women are married early, and therefore premarital fertility is low. This conservative attitude seems to have had so far a large effect on the dynamics of the HIV epidemic, reducing it to relatively low levels (Senegal, Guinea, Niger, Chad, Sudan and Ethiopia). The effect of economic development, and in particular the outstanding situation of the mining countries was also apparent (Botswana, Namibia, South Africa, Zambia). This situation implies higher income, more urbanization, higher education and therefore later marriage, and intense flows of circulatory migration, which are very conducive to the spread of sexually transmitted diseases (Lesotho, Swaziland, Malawi, Mozambique). The situation was somewhat similar in the countries providing migrant workers to Côte d’Ivoire, which could have had even lower prevalence of HIV if they had not been affected by migration (Mali, Burkina-Faso). The islands, such as Madagascar and Comoro Islands enjoy a situation of geographical isolation, which seems to have protected them so far. The situation of Rwanda and Burundi is also interesting, since these countries are located near the epicentre of the HIV epidemic, and have been the locus of major civil unrest. However, despite this unfavourable situation, the HIV epidemic was kept to only medium levels of HIV infection, probably primarily because these are highly conservative Christian countries. A number of countries appear in a situation close to that expected from exposure associated with premarital sexual behaviour, at least in the African context. This is in particular the case for the Eastern African countries (Kenya, Ouganda,Tanzania), as well as for Cameroon. However, this pattern of exposure reveals a lack of protection from sexually transmitted diseases. In addition to these patterns, the situation of some other countries is harder to explain, and in particular that of Congo, Gabon, and Liberia. These countries deserve further research. If data on premarital fertility can be considered reliable, some doubts remain with data on HIV seroprevalence. As mentioned above, only few countries publish yearly (or every other year) data based on a representative sample of pregnant women, and only about half have conducted HIV seroprevalence surveys on nationally representative samples. If there is little doubt that the level of HIV prevalence is now approximated in a satisfactory way in many of the countries studied, many questions can be raised for some countries. Both premarital fertility and HIV prevalence have a strong dynamic component. Premarital fertility has been increasing in many African countries (although diminishing in others), especially in urban areas, and although the largest differences seen today existed already twenty years ago, we did not take these dynamics into account. The problem is even more serious for HIV prevalence. For instance, doing the same analysis 10 years earlier would have hardly changed the estimates of premarital fertility, but would have dramatically changed the situation of HIV in many countries. To take a simple example, HIV prevalence in South Africa was below 1% before 1990, and one of the highest in Africa in year 2000, whereas HIV prevalence in the Congo Democratic Republic (formerly Zaire) hardly increased over the same period, from levels considered high in the mid1980’s and now considered rather low. Doing the same analysis in 1989 would have led to different correlations and different conclusions. Our snapshot around year 2000 is only part of the picture, though more convincing than before since exposure to the HIV virus has been more uniform some 25 years after the onset of the epidemic than it was in 1990. However, this is not the end of the story, and the relationship between premarital fertility and HIV prevalence could become different in the coming years. Furthermore, HIV prevalence has been declining in many countries since year 2000, and the same analysis could lead to different conclusions in a few years. We have worked at the country level of obvious reasons of data availability. Much more could be done when more data on HIV prevalence will be available, at least for urban and rural areas, and if possible by large administrative divisions (region, province). Both premarital fertility and HIV prevalence are likely to differ markedly by such categories in many countries. Much remains to be done to better understand the dynamics of HIV epidemics in Africa. Here we presented an attempt at quantifying some important cultural factors (age at marriage, permissiveness of the society) through a simple indicator (premarital fertility). Of course, this is only one element of a more complex picture, in which cultural, behavioural, socio-economic and epidemiological factors all play a role and possibly interplay. A better understanding of these complex dynamics would require more extensive and better quality data on HIV seroprevalence, and the possibility of crossing these epidemiological data with other cultural and behavioural factors, either at the individual level or at least for typical social groups, in particular by ethnic-, socio-economic-, and religious groups. We hope the HIV epidemic will become under control before these interesting data become available. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08023t1.jpg] [rh08023f2.jpg] [rh08023f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}