 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
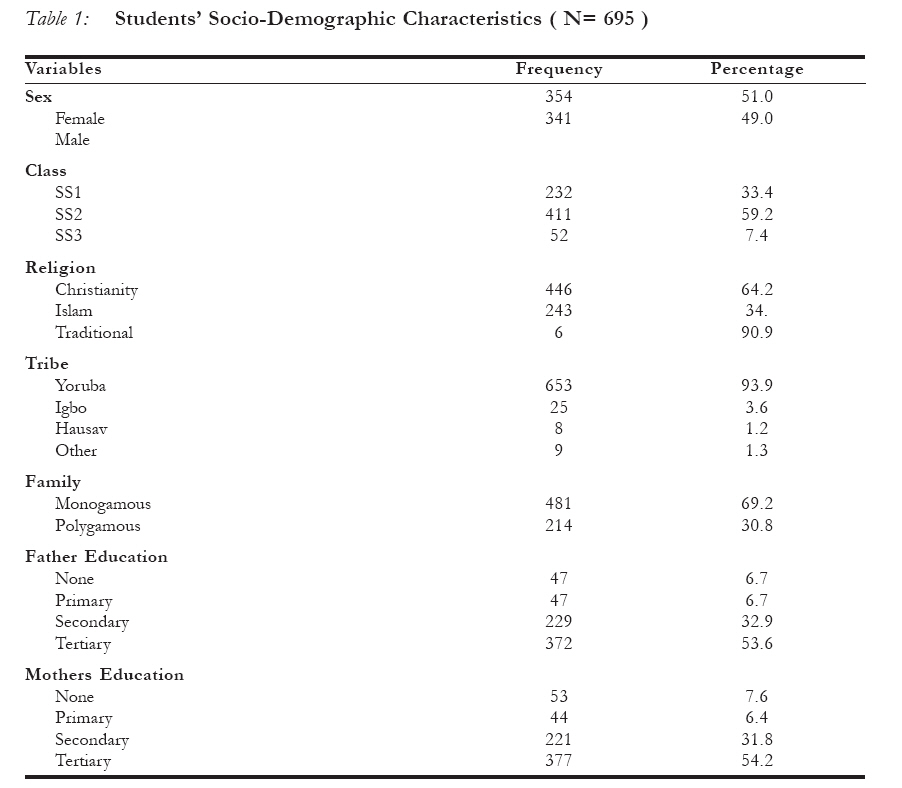
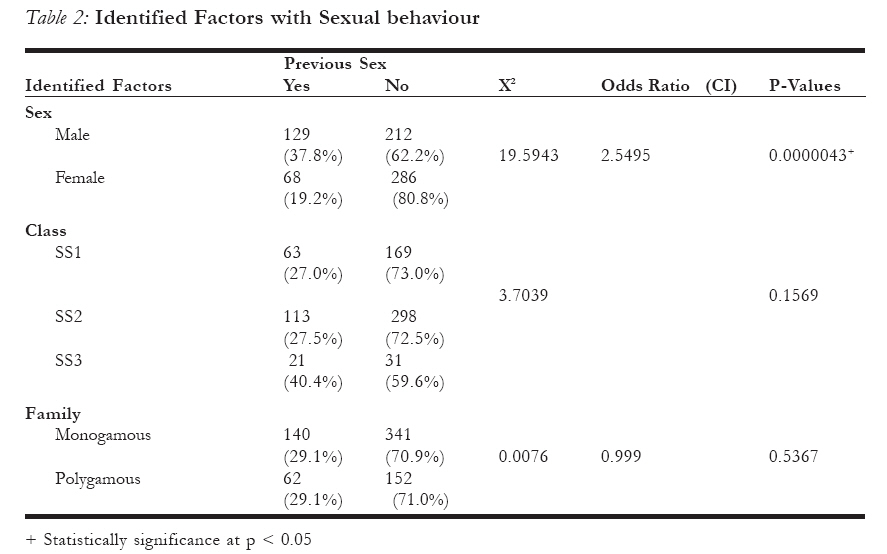
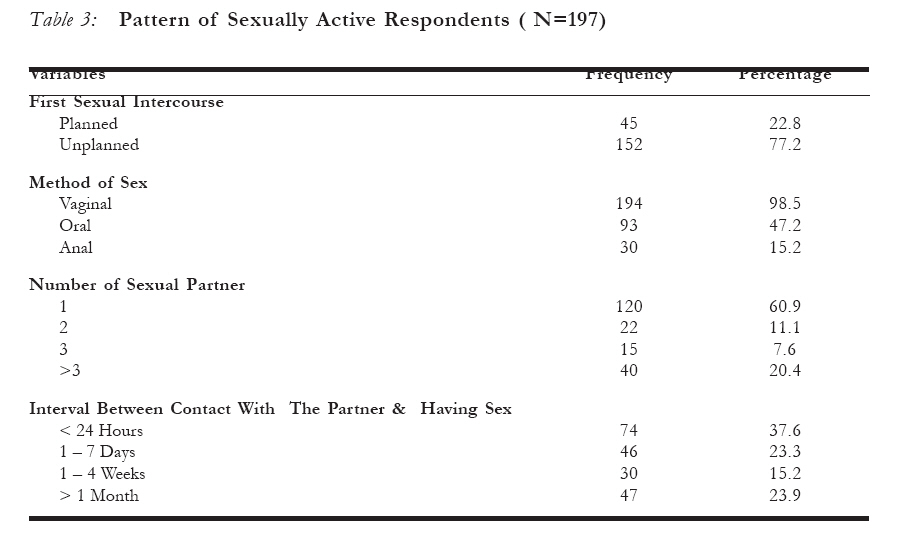
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 89-97 Sexual behaviour of in-school adolescents in Ibadan, South-West Nigeria Comporteuent sexuel des adolescents qui fréquentent encore l´ école à Ibadan au sud-ouest du Nigéria Morhason-Bello IO*, Oladokun A, Enakpene CA, Fabamwo A O*, Obisesan KA, Ojengbede OA Department of obstetrics and Gynaecology, University College Hospital, Ibadan and*Department of Obstetrics and Gynaecology,Lagos State University Teaching Hospital, Ikeja, Lagos. NIGERIA. Code Number: rh08025 ABSTRACT This study was a crossectional survey conducted among 716 senior secondary school adolescents in Ibadan from March to August 2005. The result of 695 that was analyzed revealed that the mean age of 15±2.6years. 28.3% of the respondents had previous sexual exposure with higher proportions being male (p=0.00043). Majorities’ first sexual exposure was unplanned. Family settings and educational level do not have significant influence on the previous sexual exposure. The methods of sexual activity were mainly through vagina route while some had also practiced oral and anal sex. Most of those that are sexually exposed had more than one partner. About half of the respondents learn about sex from their friends while others through their parents and media. We conclude that in-school adolescents practiced unsafe sexual activity and they are therefore predisposed to STI/HIV and other reproductive health risks. KEY WORDS: Adolescents, In- School, Sexual activity, Sexual exposure, Nigeria RÉSUMÉ Cette étude était une enquête transversale menée au sein de 716 adolescents des lycées à Ibadan entre les mois de mars et d´août 2005. Le résultats concernant 695 qui ont été analysés ont révélé que l´âge moyen était de 15±2,6, ans. 28,3% des enquêtés ont eu une expérience sexuelle antérieure, les adolescents mâles ayant des proportions supérieures (p=0,00043). Dans la plupart des cas, la première expérience sexuelle était imprévue. Les cadres familiaux et le niveau de scolarisation n´influencent pas de manière significative les expériences sexuelles antérieures. Les méthodes de l´activite sexuelle étaient surtout par voie vaginale alors que certains ont pratiqué aussi le fellation et le sexe par voie anale. La plupart de ceux qui sont exposés sexuellement avaient plus d´un partenaire. A peu près une moitié des enquêtés se renseignent sur le sexe auprès de leurs amis tandis que les autres le font auprès de leurs parents et dans la média. Nous concluons que les adolescents qui fréquentent encore l´école s´engagent dans l´activité sexuelle dangereuse et qu’ ils sont en conséquence prédisposés aux IST/VIH et aux risques de la santé de reproduction. Introduction Adolescence represents a transition from childhood to adulthood with features including secondary sexual growth, changes in hormonal milieu, emotional, cognitive and Recent WHO reports showed that many of them engage in risky sexual activity without protection and most had their debut through a subtle coercion by their partner7,8. This practice commonly resulted in sexually transmitted infections (STIs), human immunodeficiency virus, unwanted pregnancy and unsafe abortion1,9,10. Studies within Africa including Nigeria have demonstrated increasing rate of premarital sex and decline in age of sexual debut among adolescentscontrary to our moral and cultural values6,11,12. The following reasons has been advanced for the above observations, these include; high poverty level, adoption of western norm of sexual liberty, gradual erosion of traditional norms/values, lack of parental control, mass media, urbanization and tourism12,13,14. At International Conference on Population Development in both Cairo and Beijing in 1994 and 1995 respectively, adolescent/youth health was identified as a major public health problem especially among developing nations of the world6. However, despite these pronouncements a decade later nothing substantial has been achieved especially in sub-Saharan Africa6. In fact, Nigeria presently cannot boast of any functioning programme that specifically addresses adolescent reproductive health issues6. Likewise, family planning services in Nigeria did not cater to youths/adolescents rather, efforts were concentrated on married couples15. Sexuality education among adolescents in Nigeria schools had been a controversial issue that is begging to be resolved. Apart from this, studies in Nigeria have also reported high rate of parental aversion in discussing sexuality issues with their children16. This has resulted in Nigerian adolescents being vulnerable to all forms of sexually transmitted infections including HIV and unsafe abortion practices with the attendant complications18. We undertake this study to describe the sexual behaviour of in-school adolescents in Ibadan, Nigeria. Our specific objective was to determine the prevalence and pattern of sexual activity among in-school adolescents and to find out any relationship between the sociodemo-graphic characteristics of respondents and their sexual MATERIALS AND METHODS This was a descriptive cross-sectional study conducted among senior secondary schools (grades 10 – 12 high school) students in Ibadan, the largest city in West Africa. The city is located in the south-west of Nigeria, and it is made up of 11 local government councils (LGC), five councils are located within the metropolis, while six are in the outskirts of the city. Four schools (2 within the metropolis and 2 in the outskirts) were selected using stratified multistage random sampling technique among schools with coeducation. In each of the selected schools, only students in senior secondary school level 1 to 3 (grades 10 to 12) were selected using systematic random method for equal representation of both sexes. Ethical clearance was obtained from the state ministry of education and health. Consents were also required from students before enrolling them in the study. The school authorities and the respondents were assured of confidentiality in view of the intricacy and sensitivity of the questions contained in the questionnaire such as age of first sexual debut, number of sexual partners, and type of sexual practices. They were thus encouraged to answer the questions with utmost sincerity. In order to validate the questionnaire, a pilot study of 100 respondents was conducted at a school not involved in the study. The study period spanned between March to August 2005 using a self-administered questionnaire containing both open and close-ended questions. Data obtained were coded and entered into a computer running Epi-Info 2002 software package. The same module was used to validate all entries. Initial analysis was done by generation of frequency tables while further analyses were done by crosstabulation to explore statistical relationship between variables. Categorical variables and proportions were analyzed using Chi-square and parametric continuous variables with normal distribution were analyzed using student t-test. Means +Standard deviation and 95% confidence interval were calculated for normal values. Differences between two parameters were taken as statistical significance when P-values were less than 0.05 Results Out of the 716 students interviewed, the response of 695 was suitable for analysis. The age range of respondents was 12 - 24 years with mean of 15 ± 2.6years. Table 1 showed sociodemo-graphic characteristics of respondents. Both sexes were fairly represented with most respondents (59.2 %) in the second level of the senior class. Most of the students interviewed were Christian (64.2%); Yoruba (93.9%) and from monogamous family structure (69.2%). The parents of about half of respondents had tertiary level education while only few had no formal education. Of the 695 respondents, 197 (28.3%) admitted to previous sexual exposure (Figure A). Among sexually experienced group, 129 (65.5%) were male while 68 (34.5%) were female. The cross tabulation of some identified factors with respondents sexual behaviour showed that 37.8 percent of all the male students and 19.2 percent of all female interviewed were sexually experienced (X2= 19.5843, OR 2.5495, p= 0.000043) (Table 2). With respect to the level of education, about 40 percent of SS3 level, 27.5 percent of SS2 level and 27.0 percent of SS1 level students amongst those interviewed were sexually experienced (X2=3.7039, p=0.1569) (Table 2). About 29 percent of those from monogamous family were sexually experienced and similar proportions were from polygamous family (X2=0.0076, OR=0.999, p=0.5367) (Table 2). Majority (77.2%) of the sexually experienced respondents admitted that their first sexual exposure was unplanned (Table3). The method of sexual activity practised by the sexually experienced respondents were vagina (98.5%), oral (47.2%) and anal (15.2%) (Table3). About 40 percent had more than one sexual partner and most had their first sexual exposure the same day they met the partner (37.6%) (Table3). Most respondents first learnt about sex from their friends (47.7%). Others learnt from parents (25.3%), other siblings (6.0%) and through the media (21.0%) (Figure B). Discussion Adolescent reproductive health issues have been particularly of interest in the last decade because of widespread HIV/AIDS. Several researchers have made efforts find measures to curb the unacceptable prevalence of HIV/AIDS and other STIS among the youths. The sociodemographic characteristics of students studied were comparable to previous findings in Nigeria12,18,19. However, unlike other previous studies, most respondents in this study were from monogamous family11 (69.2%) and more than half of their parents had tertiary education12,18. From this study, 28.3 percent had prior sexual experience. This is a lower figure compared to the earlier reports12,18,19,. Okpani et al reported seventy-seven percent among the adolescents in Port Harcourt. He suggested that the increased sexual activity among in-school adolescents in Port Harcourt might be due to rapid urbanization of the city as Nigeria’s crude oil operations expand; coupled with the poor socioeconomic background of the indigenous adolescent12. The in-school adolescents who are sexually active had initial sexual exposure at about the same age in Ibadan like their peers in Port Harcourt12. Male respondents were more sexually active than female (p<0.05), however, they both initiated sexual activity at same age. This observation is similar to Adegbenga et al (2003)11. Sexual debut at an earlier age has been associated with increased risk of cervical cancer20; viral infections (HIV, HPV etc)21; bacterial infection (gonorrhoea, Chlamydia trachomatis)22,23. Studies have also showed that adolescent with earlier debut tend to have multiple sexual partners per unit time24. Most of the sexually experienced respondents in this study admitted that their first exposure was unplanned (77.2%). This finding further confirmed the previous observation of increased risk of adolescents to STIs and HIV, unwanted/teenage pregnancies and complications of abortions in an attempt to terminate such pregnancies13,25. Most of our respondents (60.9%) unlike other studies had only one sexual partner12. Nearly half of the respondents in this study engaged in oro-genital sex and 15 percent in anal sex. These two methods have been associated with increased risk of HIV/ other STI transmission compare with vaginal sex26,27. This may be a reflection that homosexuality is now gaining ground in our society contrary to the earlier believe of only being popular in western countries. Most respondents first learnt about sexual issues from their school-mates/ friends, sources often not properly informed about adolescent reproductive issue. Worse still, the government is not taking a bold step in incorporating adolescent sex education into the secondary school curriculum. One report indicated that parents are now having courage to discuss more about sexual matters with their children than in the past16. This is a welcome development because they will be in a better position to guide their children against unsafe sexual practises. Conclusion The outcome of this study is consistent with earlier studies conducted in many other Nigerian cities which showed that in-school adolescents to be sexually active11,18. In fact, one can conclude from this study that at least one out of every four in-school adolescents in Ibadan is sexually active and most engaged in unsafe sexual practises. Therefore, this makes them vulnerable to various medical complications including STIs, HIV/AIDS and genital cancers. Apart from this, this study also shows that male students are more sexually active than their female colleagues. Also, worrisome is the high rate of anal sex observed among these students. We therefore recommend that safe sexual practises should be discussed with our adolescents while abstinence and chastity should be upheld. In addition, there should be promotion of youth friendly forum in schools where morality, abstinence, and contraception are discussed as well as other diversionary activities like sports, debate etc . The responsibility for proper sexual awareness of our youth lies with government at all levels, parents, and other stakeholders (teachers, counsellors, community/religious leaders, non-governmental organisations, community based organisations, faith based organisations etc) and all should embrace more interventions. More research is needed. Therefore, we are proposing a wider based interventional research aimed at providing necessary information on various ways of ensuring safer sexual practices using religious/ community leaders amongst in-school adolescents in Oyo state. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08025t3.jpg] [rh08025f1.jpg] [rh08025t2.jpg] [rh08025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}