 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
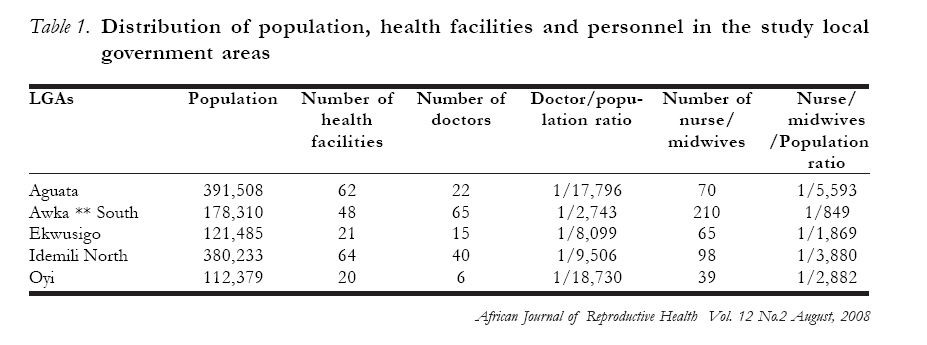
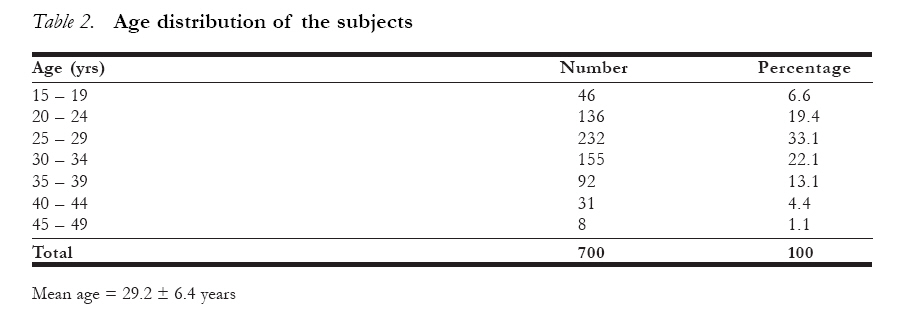
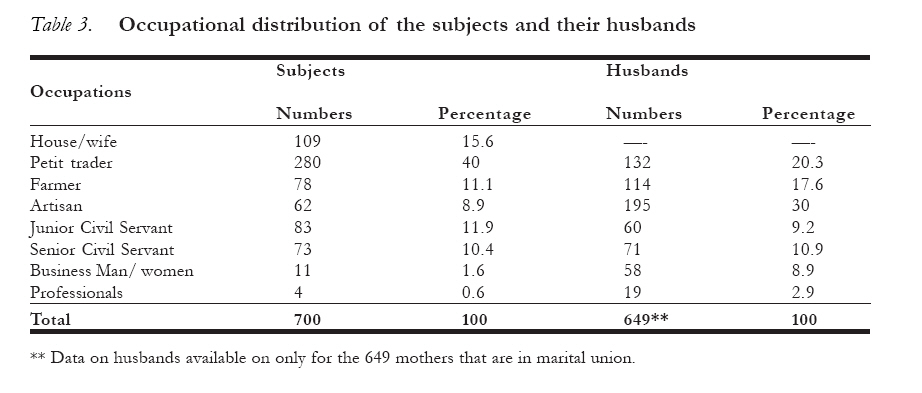
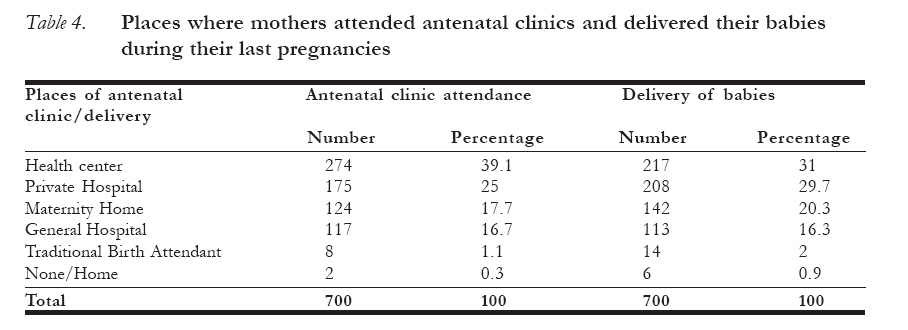
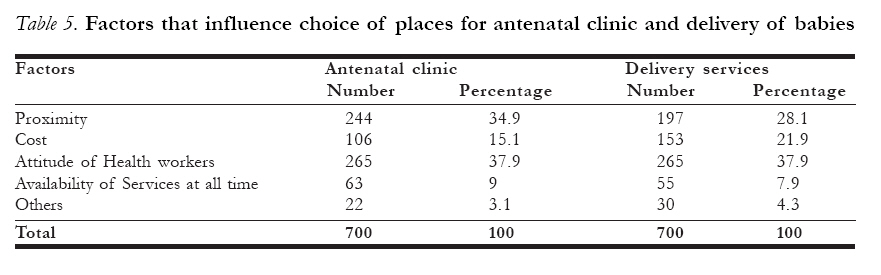
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 132-140 Is poor maternal mortality index in Nigeria a problem of care utilization? A case study of Anambra State Est-ce qu´un mauvais indice de la mortalité maternelle au Nigéria constitue un problème de l´utilisation des soins? Ibeh, Christian C. Department of Community Medicine Nnamdi Azikiwe University Teaching Hospital Nnewi,Anambra State, Nigeria. Email: christiancibeh@yahoo.com Code Number: rh08029 ABSTRACT Maternal mortality in Nigeria is unacceptably high. Some of the reasons may include poor socioeconomic development, weak health care system, low socioeconomic status of women and socio-cultural barriers to care utilization. A cross sectional study was carried out to assess the use of maternal services in Anambra State. A multi stage sampling technique was used to select 800 nursing mothers from the State who were interviewed on the use of maternal services during their last pregnancy. Over 95% of the subjects had formal education. Almost all the subjects (99.7%) attended antenatal clinics during their last pregnancy with 92.3% (646) of them making 4 or more visits before delivery. Over 97%(680) of the deliveries took place in formal health facilities. Obviously, the women in the study population utilize maternal health services. The problem of maternal mortality in the country may not necessarily lie with utilization but with the quality of services. RÉSUMÉ Une étude de cas de l´ Etat d´ Anambra. La mortalité maternelle au Nigéria est si élevée que c´est inacceptable. Parmi les raisons on peut citer le développement socio- économique, un mauvais système de soins médicaux, la mauvaise situation socio-économique de la femme et les obstacles socio-culturels à l´utilisation de soins. Une étude transversale a été menée pour évaluer l´emploi des services maternels dans l´Etat d´ Anambra. A l´aide d´une technique d´un échantillon à multi-stade, nous avons selectionné 800 mères qui allaitent qui ont été intérrogées sur l´utilisation des services maternels au cours de leurs dernières grossesses. Plus de 95% des sujets ont suivi une scolarité formelle. Presque tous les sujets (99,7%) ont fréquenté les consultations des services prénatals pendant leur dernière grosssesse alors que 92,3% (646) d´elles se sont présentées 4 fois ou plus avant l´ accouchement. Plus de 97% (680) des accouchements ont eu lieu dans des établisements de santé formels. Evidemment les femmes dans la population étudiée utilisent des services de santé maternelle. Le problème de la mortalité maternelle dans le pays peut ne pas nécessairement rester celui de l’utilisation mais celui de la qualité des services. KEY WORDS: Maternal mortality, maternal services, care utilization Introduction Maternal deaths have devastating impacts on families and communities1. Unfortunately, it is not an uncommon event in several parts of the developing world. An estimated 600,000 women die from complications of pregnancy, child bearing and unsafe abortions worldwide2, 3,4. About 99% of these deaths occur in the developing world2, 3. Indeed, the greatest discrepancy in all human development indicators is seen in the maternal mortality ratio between the developed and the developing world. The maternal mortality ratio is highest in sub-Saharan African countries3. Nigeria has a maternal mortality ratio of 800 deaths per 100,000 live births. About 35,000 women are estimated to die annually from pregnancy related causes. Out of about 27 million women of reproductive age in the country, about 2 million will not survive pregnancy or childbirth5, 6. The high maternal mortality in the developing world is sustained by a weak health care system, poor socioeconomic background and low socioeconomic status of women7. Provision of health care services to parturient mothers is critical in the outcome of pregnancy. Proportion of births attended by trained personnel has been found to correlate closely with the maternal mortality rates of nations8. Individual characteristics of mothers found to influence maternal deaths include maternal age, educational attainment, socioeconomic status and antenatal clinic attendance 9,10. While concerns are on reviewing the current pattern of obstetric services in the sub-region to make them more effective in addressing the complications of pregnancy, labour and peurperium7, 8,11,12,13,14, the socioeconomic status of women and use of maternal services must not be lost out of sight. A cross sectional survey was carried out in Anambra State, southeast Nigeria to determine whether mothers make enough contact visits with health care workers during pregnancy and delivery. Materials and methods A cross sectional study was carried out in Anambra State southeast Nigeria in 2002 to determine the use of maternal services by parturient mothers. A multi stage sampling technique was used to select the subjects. Five Local Government Areas (LGAs) were selected by simple random sampling out of the 21 Local Government Areas in the State. The selected LGAs are Awka South and Oyi in Anambra Central Senatorial District, Aguata and Ekwusigo in Anambra South Senatorial District and Idemili North in Anambra North Senatorial District. Their population in 2002 were 178,310, 112,379, 391,508, 121,485 and 380,233 respectively. Data on number of health facilities, doctors, nurse/midwives for each LGA was obtained while doctor/population ratio and nurse/ midwife population ratio were estimated. A modified WHO-30 cluster sampling technique was used to select 160 nursing mothers (mothers with babies under 6 months of age) in each of the 5 LGAs making a total of 800. The interviewers were final year medical students undergoing a rural posting in Primary Health Care. A three day training workshop was organized for them in various aspects of the survey. The field work lasted for 6 weeks. Three interviewers and a field supervisor conducted the survey in each LGA giving a total of 15 interviewers. The mothers were interviewed on the use of maternal services in their last pregnancy. A semi-structured questionnaire that sought information on sociodemographic variables and use of maternal services was used for the data collection. The supervisor edited the question-naires before collecting them from the interviewers so that incorrectly filled ones were identified and necessary corrections made while in the field. Subjects that were unavailable after three call backs were replaced with new ones by the supervisor. The data entry, validation and analysis was by EPI info software version 6. This was carried out over a 6 months period by the computer Unit of the Arbo Virus Research Laboratory, Federal Ministry of Health, Enugu. Frequency distributions, means and standard deviations of relevant variables were obtained. Results There is a high number of health facilities in each of the LGAs. The number of doctors in each LGA varied from 65 in Awka South LGA, which is the State Capital to only 6 in Oyi LGA. The number of nurse/midwives varied from 210 in Awka South to 39 in Oyi LGA. The doctor population ratio as well as the nurse/midwife ratio is low in all the LGAs except Awka South table 1. Data from seven hundred mothers were returned for analysis giving a response rate of 87.5%. The mean age of the subjects was 29.2 ± 6.4 years. Most of the subjects (87.7%) fall within the 20 to 39 year age group table 2. Six hundred and forty-nine (92.7%) of the mothers are in marital union while 24 (3.4%), 23 (3.3%), and 4 (0.6) were widowed, single and divorced/separated respectively. Over 95% of the subjects had formal education with 51.9% (363) and 18.9% (132) of them attaining up to secondary and tertiary levels of education respectively. The main occupations of the subjects are trading, civil service and farming table 3. Almost all the subjects (698; 99.7%) attended antenatal clinic during their last pregnancy. The places where the clinics were attended were mainly health centers, private hospitals, maternity homes and general hospitals table 4. The factors that influence choice of place for antenatal clinics were mainly attitude of health workers (265; 37.9%), proximity of the clinic (244; 34.9%) and cost of the service (106; 15.1). Similar factors also influenced the choice of place for delivery services though with slightly varying proportions table 5. The mean number of antenatal clinic attendance before delivery was 6.5 ± 1.8. Over 92% (646) of the mothers made 4 or more visits to the antenatal clinics before delivery. The use of formal health facilities for delivery services is very high among the subjects as 97.3%(680) of the deliveries took place in health centers, private hospitals, maternity homes and general hospitals. Only 6 (0.9%) of the mothers delivered their babies at home without the assistance of health workers. Similarly, patronage of the traditional birth attendants for obstetric services is minimal among the study group as only 14 (2%) mothers delivered their babies under their care table 4. Majority of mothers attended health facilities for antenatal clinics and for delivery of their babies in places less than I Km from their homes. The mean distance to the health facility was 1.4 ± 1.6 Km. The subjects got to the health facility by trekking (503; 71.9%); cars/motor cycles (188; 26.9%); and bicycles (9; 1.3%). Discussion The number of health facilities in the LGAs is high. However, the doctor-population ratio and the nurse/midwife-population ratio are low in the study area. This is because of the high number of primary health centers in the LGAs, which are mostly manned by nurse/midwives and nurse assistants (Community Health Extension Workers). Similarly, most private hospitals and maternity homes engage the services of nurse assistants (auxiliary nurses) thereby leading to the relatively low number of nurse/midwives working in the study area. The Socio demographic profile of the subjects is similar to the findings of the Nigeria Demographic and Health Survey (NDHS) of 2003 for southeast Nigeria. For while the study showed that over 95% of the subjects had formal education with 51.9% (363) and 18.9% (132) of them attaining up to secondary and tertiary levels of education respectively, the NDHS found that 7.7% had no education while 55.5% and 12.1% had secondary and post secondary education respectively15. A high proportion of mothers are gainfully engaged in productive ventures. The high proportion of mothers with formal education and means of livelihood has implications for health, as education and income are important determinants of maternal health2,9,10. Almost all the mothers attended antenatal clinic during their last pregnancy. This is in contrast to the findings in Northern Nigeria and rural Pakistan where only 25.9% and 61% of the women respectively received antenatal care during their last pregnancy16, 17. The high rate of patronage of antenatal services in the study population is commendable, as prenatal services have been known to be one of the sure ways of reducing maternal morbidities and mortalities7, 13,18,19. The subjects obtained their antenatal services mostly from the formal health sector viz health centers private hospitals, maternity homes and general hospitals. These health facilities are conventionally manned by trained personnel and regulated by the state ministry of health. The proportion of mothers that used the services of the traditional birth attendant for antenatal visits is meagre. This is corroborated by the findings of the NDHS which showed that only 0.9% of the mothers visited the traditional birth attendants for prenatal care in southeast Nigeria15. The factors that influenced choice of facilities for prenatal services are very revealing and have policy implications. The attitude of health workers is considered the most important factor followed by proximity and the cost of services. Other authors have recognized the influence of health workers attitude to care utilization16, 20,21. The current reform in the health sector in Nigeria is expected to address this. The primary health programme in Nigeria has obviously helped in making health care services including maternal care available to people close to where they live. As a result distance to antenatal services in the state does not seem to pose serious problems. Majority of the subjects reported that the facilities were less than 1.5 Km and that they trekked to their places of prenatal services. The number of antenatal visits by the subjects before delivery is commendable. For while over 94% of the mothers made 3 or more visits, the mean number of visits of 6.5 ± 1.8 is enough contact time for the health workers to identify and address any likely untoward events of pregnancy. It is above 4, minimum number of antenatal visits recommended by the World Health organization22. A study in Israel showed the rate of physician visits during prenatal period to be in the range of 2.3 ± 2.4 to 4.9 ± 2.923. Studies have compared the standard model of prenatal services with a new model that emphasizes actions known to be effective in improving maternal and neonatal outcomes and has fewer clinic visits. In such studies, the standard model with a median visit of 8 and the new model with a median of 5 were shown to be comparable in both maternal and perinatal outcomes11, 12,13. The use of the formal health facilities for delivery services is very high in the study population as 97.3% of the subjects delivered in health facilities. This is in contrast to a study in Pakistan where 67% of the women delivered at home while a study in northern Nigeria showed that only 9.9% of the women delivered in a health facility16, 17. Compelling evidence show that maternal deaths are substantially reduced when a high proportion of births are attended by health professionals2, 3,7,8. From the above, it is normal to expect a high standard of maternal health in the study population since their utilization pattern for maternal services is comparable to what is obtainable in some of the developed nations11, 12,13,23 . This however is not the case. The maternal mortality ratio for Nigeria is 800/ 100,000. The reasons for the high maternal deaths are not far fetched. In the developing world, it is not just sufficient to state that attendance of births by trained professionals will drastically reduce maternal deaths. It is also necessary to consider the preparedness of the health facilities to cope with obstetric emergencies. Avoidable hospital factors are known to contribute substantially to maternal mortality in the developing world20, 24,25,26. A number of the health facilities especially at the primary health care centers, maternity homes and some private and general hospitals in the country do not meet up with the criteria for basic or comprehensive essential obstetric care. A national survey on essential obstetric care revealed that less than a third of the public sector referral health facilities in Nigeria met the standard for comprehensive essential obstetric care27. As a result, even the referral centers in the country are incapable of effectively attending to women with obstetric emergencies. Even in situations where the health facilities do meet the EOC criteria as in teaching hospitals, several other contending forces still render emergency obstetric care ineffective. For example, the decision-surgical intervention intervals in teaching hospitals in Nigeria could vary from 30 minutes to 5.8 ± 1.2 hours. The delays are attributable to unavailability of blood, electricity, sterilized instruments, ambulance, late arrival of experienced theatre staff and unhealthy hospital policy20, 24 . The interval between request for blood and its availability for transfusion to patients in hospitals in Nigeria could be up to 3 to 4 hours28. With these scenarios in mind, it becomes clear that the problem of maternal mortality in Nigeria may not necessarily lie with the mothers’ failure to utilize maternal care but that the health care system probably needs to be repositioned to meet up with the challenges of modern obstetric care. Acknowledgement I wish to thank Prof J.I.B. Adinma of the Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University Teaching Hospital Nnewi for his useful contribution to the conduct of the study, Mr Francis Orizu of the National Arbovirus Research Laboratory Enugu for assistance in data entry and analysis and staff of the Department of Community Medicine Nnamdi Azikiwe University Teaching hospital Nnewi for their support and understanding in the conduct of the study. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08029t5.jpg] [rh08029t4.jpg] [rh08029t3.jpg] [rh08029t2.jpg] [rh08029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}