 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
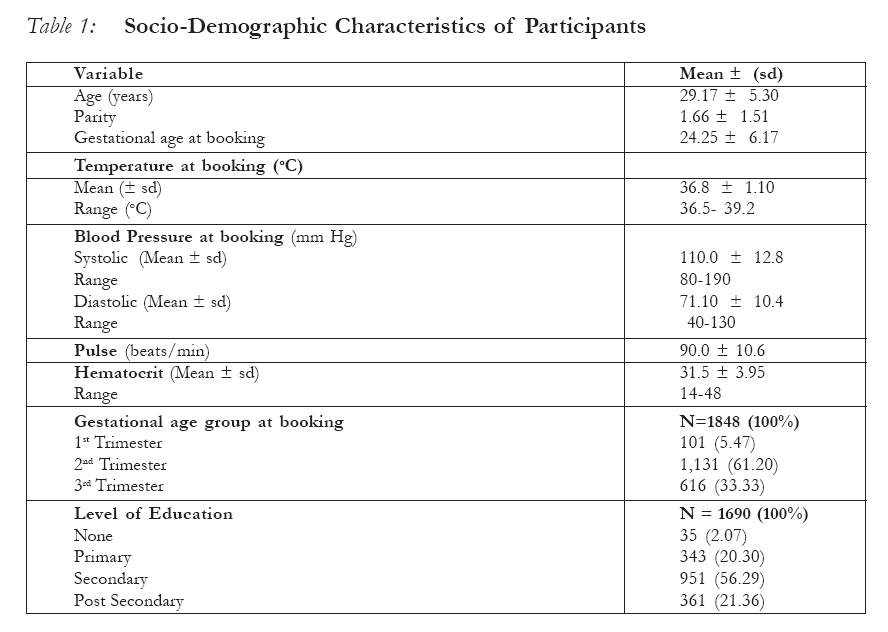
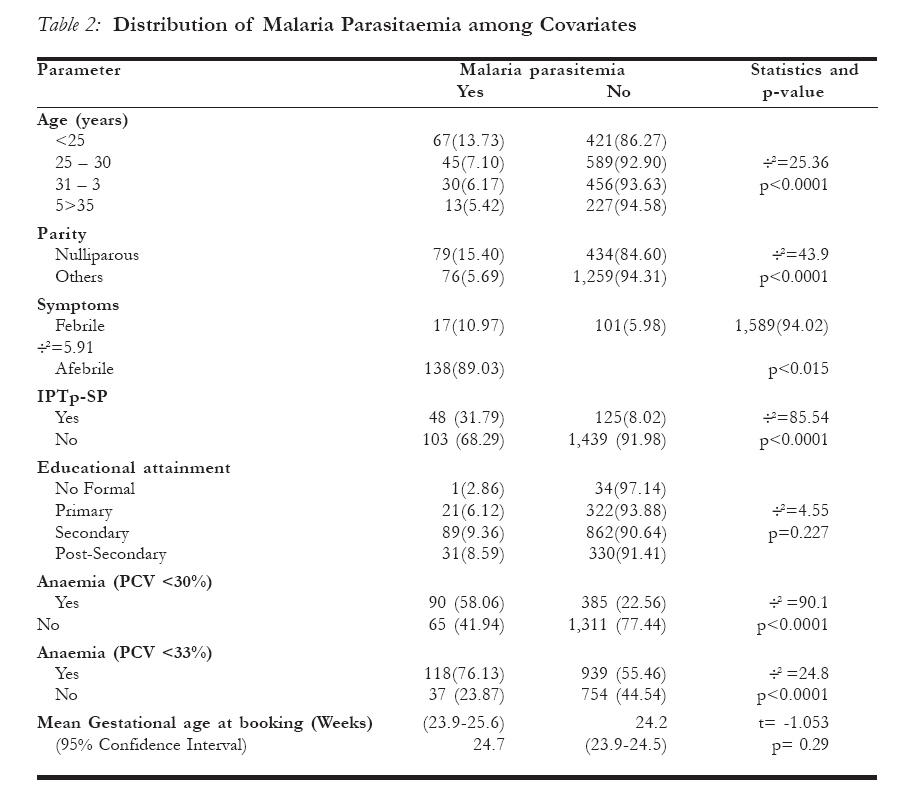
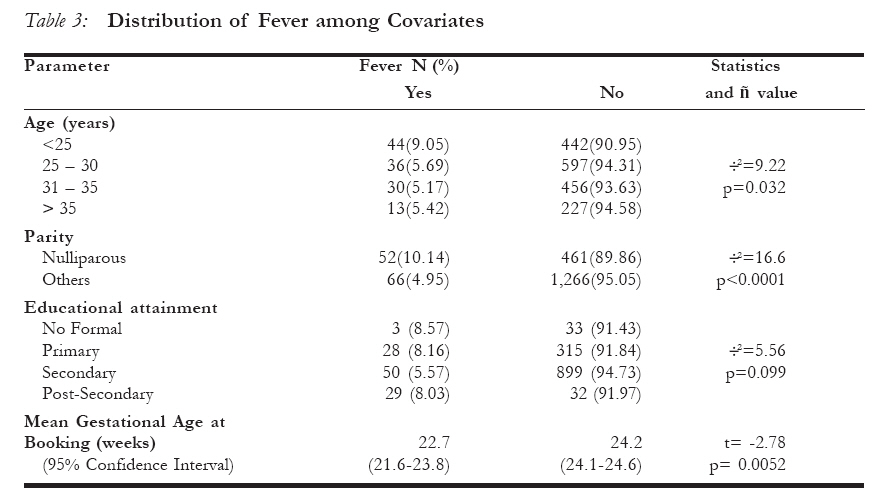
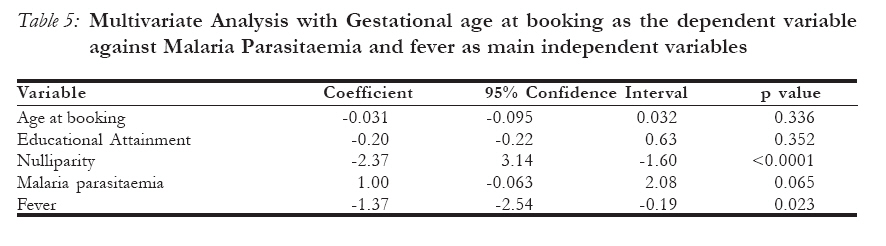
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 141-152 Prevalence of malaria at booking among antenatal clients in a secondary health care facility in Ibadan, Nigeria Prévalence du paludisme au moment de l’inscription chez les clients pour le service prénatal auprès d’un Centre de santé secondaire à Ibadan, Nigeria Falade C O1, 2, Olayemi O3, Dada-Adegbola H O4, Aimakhu C O3, Ademowo O G1, 2 and Salako L A1 1Department of Pharmacology & Therapeutics, College of Medicine, Universityof Ibadan, Nigeria Code Number: rh08030 ABSTRACT The prevalence of malaria parasitemia at booking was studied in 1,848 pregnant women in a secondary hospital in Ibadan, Nigeria. Main outcome variables were patent parasitemia and fever. 8.4% had patent malaria parasitaemia. Most clients (89%) with parasitemia were asymptomatic. Febrile subjects booked at an earlier gestational age [22.7 versus 24.2 weeks] than afebrile patients (p = 0.0052). Anemia was more prevalent among patients with patent parasitemia than those without (58.1% versus 22.6%, p<0.0001). Malaria parasitaemia was higher among nulliparous women than other parity groups (p<0.0001). Symptomatic malaria was associated with early booking for antenatal care and malaria parasitemia was a significant determinant of anemia. The prevalence of malaria parasitaemia in this study is much lower than in previous reports. RÉSUMÉ L’ étude sur la prévalence de la parasitémie du paludisme au moment de l’inscription a été menée auprès des 1,848 femmes enceintes dans un hôpital secondaire à Ibadan, Nigéria. Les principaux variables de résultat étaient la parasitémie évidente et la fièvre. 8.4 %( 155/1848) avaient la parasitémie du paludisme évidente. La plupart des sujets (89%) qui avaient la parasitémie étaient asymptomatiques. Les sujets fébriles se sont inscrites à un âge gestationnel plus jeune [22,7 semaines par opposition à 24,2 semaines] que les patientes afébriles (p=0,0052). L’anémie était plus significativement prévalente chez les patientes qui avaient la parasitémie évidente (58, 1%) par rapport à des patientes qui n’en avaient pas (58,1% contre, 22,6%, p<0,0001). Les femmes nullipares avaient une incidence plus élevée de la parasitémie du paludisme par rapport aux autres groupes de parité (p<0001). La prévalence du paludisme dans cette étude est beaucoup inférieure par rapport aux résultats signalés dans le passé. Le paludisme symptomatique a été lié à l’inscription précoce pour le service prénatal et la parasitémie du paludisme était un déterminant important de l’anémie. KEY WORDS: Malaria parasitaemia prevalence antenatal care clients Introduction Malaria is endemic in Nigeria and pregnancy increases the susceptibility to this infection.1 One of the most common complications of malaria in pregnancy is anemia which also has a negative impact on the outcome of pregnancy.2-5 This parasitic infection in pregnancy is associated with serious adverse effects which include acute febrile illness episodes, abortions, premature delivery, severe anemia, low birth weight babies, congenital malaria and even death. In endemic areas, malaria in pregnancy is more common and more severe in the primigarvida because women acquire resistance to chondriotin sulphate A (CSA) binding parasites in successive pregnancies. The multigravida unlike her primigravida counterpart is thus less susceptible to placental malaria and is more likely to produce healthy babies. Numerous epidemiological studies have reported a broad range of conditions during pregnancy which are a result of malaria.6, 7 Although antenatal clinic attendance in south western Nigeria is reported to be 99.1% and the overall figure for Nigeria 83.1% (NDHS 2003)8 booking is late9, 10 and the rate of delivery at health care facilities is low11, 12, 13. The few women who present early at booking are likely to have had medical complications or a history of poor pregnancy outcome in previous pregnancies. Women who book late in pregnancy are more likely to be multiparous with relatively good outcome in previous pregnancies14. Other reasons for late booking include ignorance, financial constraints and delay in the decision taking process which often requires the husband’s consent7. The aim of this study was determine the prevalence of malaria parasitaemia at booking and its influence on the gestational age of booking. Intermittent preventive therapy (IPTp) with sulphadoxinepyrimethamine (SP) was recently adopted in Nigeria for control of malaria in pregnancy. This stipulates that all pregnant women receive at least two therapeutic doses of SP during pregnancy starting soon after quickening and the second dose at least one month apart. Evaluation of the prevalence of malaria parasitaemia and gestational age at booking will afford us the opportunity of accessing the burden of malaria at booking, the proportion of infected women among the clients who will benefit from the presumptive treatment at first contact and give additional reinforcement for the implementation of the IPTp strategy. MATERIALS AND METHODS We used a cross sectional design. All pregnant women who reported for booking at St. Mary’s Catholic Hospital in Ibadan southwestern Nigeria and provided informed consent were enrolled into the study. Ibadan is located in the rainforest belt of southwestern Nigeria. Malaria transmission is intense and occurs all year round in the study area. St Mary Catholic Hospital, Eleta is a private secondary health care facility run by the Catholic mission. The hospital is located in the heart of the indigenous area of Ibadan. However, because of the reputation for good health care it had built over many years, the hospital draws patient from all over the ancient city of Ibadan. Statistics from the hospital revealed that on average eighty women book for antenatal care weekly, and thus we had a large pool of clients to study. Pregnant women who came for booking at the antenatal clinic of the study center between November 2003 and October 2004 were enrolled into this study. This study was conducted during both the high and low malaria transmission seasons (rainy and dry seasons respectively). Ethical approval was provided by the Joint University of Ibadan/University College Hospital Institution Review Committee as part of a larger study investigating the epidemiology of congenital malaria. A written informed consent or witnessed verbal informed consent was obtained from each participant. The study was done to Good Clinical Practice standard and followed the principles of the Declaration of Helsinki15 To be eligible for inclusion in the study, clients must be confirmed pregnant (abdominal ultrasound in early pregnancy or a positive pregnancy test). Pregnant women who meet the inclusion criteria and gave their consent were enrolled at the booking clinic which runs on Tuesdays and Thursdays. At booking, information on the age of the women, length of pregnancy, or gestational age at booking, gravidity, parity, level of education and other demographic details were obtained. Information on drug use before booking e.g. antibiotics, antimalarial drug and hematinics, were also obtained. Each study participant had a complete medical examination including the axillary temperature and blood pressure. Medical examinations were carried out by trained midwives who work with the hospital, resident doctors on the family practice fellowship programme in the hospital and the investigators (COF and HOD). Temperature African Journal of Reproductive Health Vol. 12 No.2 August, 2008 was measured to the nearest 0.1oC using an electronic thermometer. Fever was defined as axillary temperature > 37.5°C. Gestational age was assessed using a gestational calendar, trimester was defined as first (<14 weeks), second trimester, 14-<28 weeks and third trimester 28 weeks or above. Thick and thin blood films were prepared from a finger prick blood sample of all enrolled patients. Blood was also obtained into duplicate heparinized capillary tubes for evaluation of haematocrit. Methodology for quantification of malaria parasites employed a standardized quality assurance training program for malaria microscopists and investigators of four research centres participating in a larger multi-center study evaluating the epidemiology of congenital malaria in Nigeria.16 A mandatory 6-day training workshop was performed at one of the study centers (Ibadan). Each team was provided with identical protocols, and identical standardized reagents including Wright Giemsa stains, unsilicated microscopy slides, and buffer concentrates. Following completion of the workshop, monthly quality control was carried out at each study center whereby slides were given an intercode (blinded) and reviewed by a second microscopist at each respective center. Three refresher courses and quality assurance workshops were also carried out three months after commencement of the study, midway and at the end of the study period.16 Standard antenatal care protocols were followed in the study hospital. Screening for hypertension, proteinuria and anaemia were part of routine care. Also, serology for syphilis, determination of ABO blood groups, Rhesus factor and hemoglobin genotype were all part of routine care in the hospital. Attention is routinely paid to the prevention of anaemia and malaria and for this purpose hematinics - folic acid, ferrous sulfate are routinely given. During the study, intermittent preventive antimalarial chemotherapy (IPT), with sulfadoxinepyrimethamine was undergoing a pilot study. Mothers whose blood smears were positive for malaria parasite at any stage of the pregnancy received chloroquine at a dose of 1500 mg base over three day or sulfadoxinepyrimethamine for mothers who had a history of allergy to chloroquine. A repeat blood film for malaria parasite was carried out at days 3 and 7 to ensure cure. Chloroquine and sulfadoxine-pyrimethamine were the first and second line antimalarial drugs in Nigeria at the time of the study The prepared thick and thin blood films were stained with 10% freshly prepared Giemsa stain at pH 7.2 for parasite identification and quantification. Parasite density was determined by counting the number of asexual parasites relative to at least 200 leucocytes in each thick blood film and assuming a mean leukocyte count of 8000/µl of blood.17 Blood smears were screened by a trained microscopist following standard, quality control procedure. Parasitaemia was expressed, as the number of asexual forms of P. falciparum per microliter of blood and a blood smear was considered negative only after reading of 100 high power fields without detecting a parasite under a light microscope at x1000 magnification. Hematocrit was determined by Hawskey™ microhaematocrit centrifuge and read on the microhaematocrit reader. The mean of two readings were recorded as the hematocrit for the patient. Parasitaemia was graded as low (Parasite < 1000/µL), moderate (>1000 – 9,999/µL), and high (>10,000/µL). Hematocrit levels as normal (>30%); mild anemia (27-29%); moderate anaemia (19- 26%) and severe anaemia (< 18%). The main outcome variables were the presence of malaria parasites in blood film and fever. Both were categorized as a binomial variable “yes” if present and “no” when absent. Data was initially explored using the codebook function of the Stata software, categorical variables were analyzed using the chi-squared (Fischer’s exact) test while continuous variables were analyzed by t-test both for equal and unequal variance using the variance ratio function of the Stata software to determine the appropriate use of the Satterthwaite’s correction for the degrees of freedom. Multivariate analysis was by multiple linear regressions. Level of statistical significance was at p< 0.05 for all the analyses. Results Client Demographics Between November 2003 and October 2004, 1,848 clients were enrolled. The Mean age at booking for all the study subjects was 29.2 years (± 5.3). Most of the women were in the age group 25-30 years accounting for 34.3% of the study participants. The modal parity group is the nulliparous group with 27.8% of the participants in this group. The mean gestational age at booking was 24.3 weeks (± 6.2), 5.5% booked in the first trimester, 61.2% in the second trimester and 33.3% in the third trimester. Most (56.3%), of the women enrolled in the study had secondary school education, 21.36% had post secondary education and only 2.1% had no formal education. Other socio-demographic and biological characteristics of the participants are shown in Table 1. Prevalence of malaria parasitemia The prevalence of malaria parasitaemia in the study population was 8.4% of which 3.6% had low parasitaemia, 4.1% had moderate parasitaemia and only 0.7% had high parasitaemia. The prevalence of malaria by trimester at booking was 4% in the first trimester, 8.8% and 8.3% in the second and third trimesters respectively. Details of the distribution of malaria parasitaemia among covariates are shown in Table 2. The prevalence of patent parasitaemia was highest among the less than 25years age group with a prevalence of 13.7%. This was statistically significant (÷ 2=25.36, p<0.0001) when compared with other age groups. Nulliparous patients not only had the highest prevalence of malaria parasitemia (15.4%) compared to the other parity groups but also in the entire study population. The educational attainment of the study subjects had no significant association with the prevalence of malaria parasitaemia. The distribution of fever among the various covariates is shown in Table 3. The distribution followed a similar pattern as that of malaria parasitaemia. The age group less than 25 years and the nulliparous subjects had the highest incidence of fever. The prevalence of asymptomatic malaria was 89.0% as shown in table 2. Fever was significantly more common among clients who had patent parasitaemia (10.97%) when compared with those who did not have parasitaemia (5.98%) Details are shown in table 3. Only women who booked in the second and third trimesters (N = 1710) were eligible to receive IPTp. One hundred and fifty one (8.8%) of these had patent parasitaemia. About a third (48/151; 31.8%) of the women who had peripheral malaria parasitaemia received IPTp with sulphadoxinepyrimethamine while 8% (125/1564) of those who were free of malaria parasites received IPTp. The mean gestational age at booking was not associated with the prevalence of malaria parasitaemia as shown in Table 3. However the mean gestational age at booking had significant association with the incidence of fever. Febrile subjects booked at a mean gestational age of 22.7 weeks (95% CI 21.623.8) while the afebrile subjects booked at a mean gestational age of 24.2 weeks (95% CI 24.1-24.6). This difference was statistically significant. Although a large proportion (86.3%) of the pregnant women with parasitaemia were afebrile, fever was still significantly more frequent among those who had patent parasitaemia (10.97%) compared with those who did not have parasitaemia (5.98%) as shown in table 2. The multivariate model involving the various covariates is displayed in Table 5. In this model, fever and nulliparity were significant determinants of early booking, while maternal age at booking, malaria parasitaemia and educational attainment were not statistically significant in the model. Anaemia The incidence of anaemia at booking in this study was 25.6% (PCV <30%). In table 3, the incidence of anaemia at booking is tabulated against malaria parasitaemia and fever. The highest incidence of anaemia was among subjects who had malaria parasitaemia (58.06%) compared to those without parasitaemia in which it was 22.56%. This was statistically significant (p<0.001). In the group with malaria parasitaemia, 27.10% had mild and 30.32% had moderate anemia. This was significantly higher than among patients without patent parasitemia with 14.7% and 7.7% incidence of mild and moderate anaemia respectively. Fever did not have a statistically significant association with anemia. The incidence of anemia among febrile and afebrile subjects was 28% and 25.4% respectively and this was not statistically significant. When the WHO definition of hematocrit <33% was used for analysis, the incidence of anaemia among the study population was 57.2% (1057/ 1848) with 47.2% (876/1848), 9.6% (178/ 1848) and 0.1% (3/1848) belonging to mild, moderate and severe anaemia groups respectively. Discussion The prevalence of malaria parasitaemia found at booking in this study is much lower than figures reported in other studies from Nigeria. In a similar study in Jos, Nigeria, 18 the prevalence of malaria in pregnancy was 38.8%, in another study among antenatal patients booking at primary health care facilities in Lagos. Anorlu et al.19 found figures as high as 44% among primigravidae in their study population while Nnaji et al20 recorded 87.9% among primigravidae in Nnewi, south eastern Nigeria.. The location of the study is a variable that could have affected the prevalence of malaria parasitaemia. Our study was conducted in the urban city of Ibadan. The prevalence of malaria parasitaemia is usually higher in the rural environment where mosquito breeding and malaria transmission is more intense.21, 22 The fact that 77.7% of study participants had at least a secondary education could also have contributed to the recorded lower level of patent parasitaemia obtained in this study since they would have been better informed about antivector measures including window nets and insecticide spraying and so might have used them. Ikeako and his collegues12 working in Enugu south eastern Nigeria reported that formal education was a significant predictor of the use of maternity services in health institutions. Some of the women could have taken anti malarial drugs for self treatment of fever since these are freely availability over the counter in Nigeria. History of antimalaria drug use prior to booking was not collected during the study. These results might have as such under estimated the prevalence and morbidity of malaria in pregnant women at booking in Ibadan southwestern Nigeria. However, there has been conflicting reports on the effect of prior antimalaria use before booking. Arnolu et al19 reported that the previous use of antimalaria drug before booking had no significant effect on the prevalence of malaria parasitaemia or parasite density in a study conducted in Lagos south western Nigeria, while Akanbi et al23 reported that self treatment of malaria led to a reduction in the prevalence parasitaemia among pregnant women attending antenatal clinic. It is also noteworthy, that this study was carried out in a private mission hospital where subsidized fees were paid for health care. The majority of clients attending this health care facility when compared to primary health care (PHC) facilities where one of the earlier quoted studies19 was conducted may be from a higher economic class of people who can afford some preventive interventions. It is also pertinent to note that the microscopists and investigators involved in this study had undergone pre study malaria microscopy training to improve competence at microscopy and rigorous quality assurance procedure was adhered to during these studies. Malaria parasitaemia was significantly higher in nulliparous women in this study; they had about 3 times the prevalence of the other parity groups. This finding is well documented in other studies19, 20, 23, 24 and the immune response in pregnancy to the malaria parasite is the reason given for this observation. Age was also found to be a significant determinant of malaria parasitemia in this study. This may be due to the indirect effect of parity since most of the nulliparous women are younger than the multiparous patients. We are also aware that pregnant women aged <25 years has consistently been shown to have a higher prevalence of malaria parasitaemia. However, age was no longer significantly associated with patent parasitemia among our study population after multivariate analysis (table 5). The difference in the occurrence of fever relative African Journal of Reproductive Health Vol. 12 No.2 August, 2008 to malaria parasitaemia in this study is similar to the findings of Onyenekwe et al.25 Anemia was significantly associated with malaria parasitaemia in this study similar to findings from other studies.26, 27 The incidence of anaemia among patients with malaria parasitaemia was 58.06% using 30% hematocrit cut off level to define anaemia. If the higher level of 33% was applied the incidence would be much higher than this. Unlike malaria parasitaemia, fever was not significantly associated with anemia; this data can be interpreted as meaning that most of the anemic patients are asymptomatic for malaria. This is similar to previous the findings in Cameroon where they found a significant association between malaria parasitaemia and anemia in pregnancy.28 The mean gestational age at booking in the secondary health care facility where we conducted our study is slightly higher than the findings of Okunlola et al.14 working in a tertiary health care facility in the same city. The results of this study show that fever and nulliparity were significantly associated with a lower mean gestational age at booking while malaria parasitaemia showed no statistically significant change in the mean gestational age at booking (Table 2). This supports the finding of Okunlola et al.14 that illness in current pregnancy and nulliparity were associated with early booking for antenatal care. Symptomatic patients booked for antenatal care at a mean gestational age 1.4 weeks earlier than the asymptomatic patients in this study and nulliparous patients booked at a mean gestational age 2.4 weeks earlier than the multiparous patients after controlling for other factors in the multivariate model (Table 5). Symptomatic malaria was a significant associated with the time of booking for antenatal care among the study participants, and malaria parasitaemia was a significant determinant of anemia in pregnancy in this study. The observed pattern of late booking during the second and third trimester for antenatal care recorded in this study is in keeping with previous reports.7, 8, 14, 19 . Undesirable as this might be for safe motherhood, it still affords a significant proportion of the clients the oportunity of receiving the first dose of IPTp at booking and instructions to come for the second dose one month after booking in keeping with the national guidelines for malaria prevention and control during pregnancy. This is of great significance as a large proportion of pregnant women in Nigeria are reported to attend only one (X%) or at most two (y%) Dapo, please insert the figures from the NDHS antenatal clincs through out pregnancy. It is of note that almost a third of the parasitaemic women enrolled in this study received IPTp at booking thereby benefiting from the IPTp strategy compared with less than 10% of those who were free of parasiatemia. Acknowledgement We thank the mothers who participated in this study, authorities of St. Mary’s Catholic Hospital, Eleta, Ibadan, Nigeria, our research staff and staff of the antenatal clinic in which this study was conducted. This work was supported by a Cooperative Agreement between Boston University and the Office of Health and Nutrition of the United States Agency for International Development. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID. The funding agencies did not influence the conduct or outcomes of the analysis or exercise any editorial control over this paper. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08030t4.jpg] [rh08030t3.jpg] [rh08030t5.jpg] [rh08030t2.jpg] [rh08030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}