 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
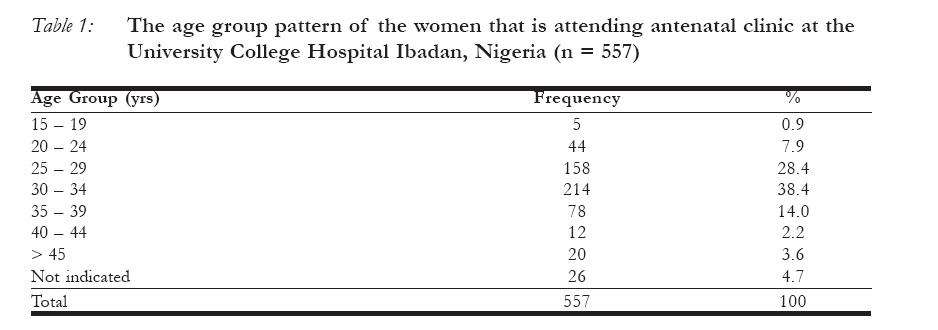
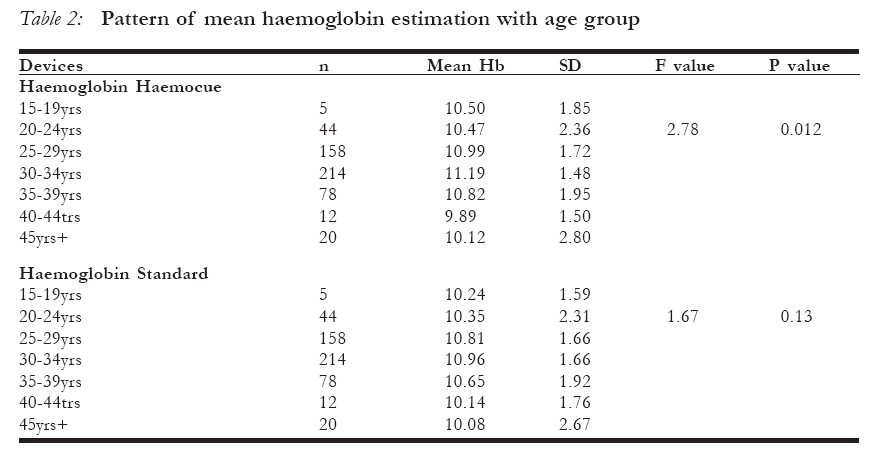
African Journal of Reproductive Health, Vol. 12, No. 1, April 2008, pp. 153-159 Comparative evaluation of haemoglobin estimation amongst pregnant women in Ibadan: Hemocue – B Haemoglobin analyzer versus haemiglobincyanide (Standard) method as the gold standard Evaluation comparative de l’ estimation de l’hémoglobin chez les femmes enceintes à Ibadan: L’analyseur de Hémoglobin Hemocue B par opposition à la méthode de l’hémoglobincyanide (standard) comme le standard d’ or. O. A. Ojengbede1, S. N. Okonkwo, I. O. Morhason-Bello all from Department of Obstetrics & Gynaecology, University College Hospital Ibadan, Nigeria. Correspondence to be addressed to: Professor Oladosu A. Ojengbede Department of Obstetrics & Gynaecology, College of Medicine, University of Ibadan, University College Hospital, Ibadan, Nigeria. Email: ladosu2002@yahoo.co.uk Code Number: rh08031 ABSTRACT: This was a comparative crossectional study that was conducted among 557 antenatal women at the University College Hospital, Ibadan, Nigeria between 1st April and 30th May 2006. The study compared the accuracy of haemoglobin estimation using an automated HemoCue B analyzer kit with a standard laboratory method (haemogloincyanide) as the gold standard. The result showed a positive correlation of HaemoCue haemoglobin results when compared with the standard methods (Pearson’s correlation coefficient = 0.892; p value = 0.000). We concluded that the use of the automated HemoCue kit for haemoglobin estimation gives an objective assessment which overcomes the challenge of extra skilled manpower or power outages in rural areas thereby enhancing access to quality of care in resource poor countries. RÉSUMÉ Il s´agissait d’une étude transversale comparative qui a été menée au sein de 557 femmes qui fréquentaient le service de consultation prénatale au Centre Hospitalier Universtaire d’ Ibadan, Nigéria, entre le le avril et le 30 mai 2006. L´étude a comparé l´exactitude de l´estimation de l’hémoglobine à l’ aide d’une trousse de l’analyseur automatique de’ l´Hémo Cue B avec une méthode standard de laboratoire (l´hémoglobincyanide) comme le standard d´ or. Le résultat a montré une corrélation positive des résultats de l´hémoglobine hémo Cue par rapport aux méthodes standard ( le coefficient de corrélation de Pearson = 0,892; p valeur = 0,000). Nous avons conclu que l’emploi de l’analyseur automatique de l’ Hémo Cue pour l’ estimation donne une évaluation objective qui surmonte le défi de main–d’oeuvre très qualifiée ou des interruptions d’électricité dans les régions rurales promouvant ainsi l´ accès á la qualité de soin dans les pays qui ne disposent pas d´assez de ressources. KEY WORDS: Haemocue, B analyser, Anaemia in Pregnancy, Haemoglobin estimation Introduction Anaemia in pregnancy is a public health problem all over the world1. The burden of this disease is mainly in developing countries including Nigeria1,2,3. Conservative estimates indicate that about 1500 million people are anaemic worldwide, with about 1400 million in South Asian and African countries1. In addition, the World Health Organization (WHO) estimate and other hospital based studies reveal that two-fifth of non-pregnant and about half of pregnant women in developing countries have anaemia1,4,5. Studies have shown that most of the women who suffer complications have moderate to severe anaemia and they also suffer from morbidities such as; recurrent miscarriages, intrauterine growth restriction, preterm labour and fetal wastages1,6. In addition, majority of the pregnant anaemic women leave in rural areas that lack basic social ammenities7. One of the most crucial aspects of management of anaemia is the determination of haemoglobin concentration. This affords the health care providers the opportunity to determine the severity of the disease and the likely methods of prompt treatment. The 2003 demographic and health survey of Nigeria showed that majority of pregnant women seek antenatal care services at primary health care centers that are manned by midwifes or community health extension workers without the luxury of laboratory services handled by trained personnel7. As such these women do not have the opportunity of objective assessment of the clinical status by haemoglobin estimation. Studies have shown that clinical assessment of anaemia is very unreliable when compared to other standard methods of haemoglobin estimation8. Even, where the microhaemtocrit centrifuge machine is available, supply outages and paucity of laboratory scientists in Nigeria remained major impediments to its use. The WHO introduced both Taliquist9 and haemoglobin colour scale10 as a simple method for haemoglobin estimation however, they were later found to be inaccurate and unreliable11,12,13. The continuous search for a more reliable but simple technology for objective estimation of haemoglobin generally led to the development of Hemocue Bhaemoglobin analyzer. This automated kit is portable, rapid and accurate in measuring haemoglobin concentration at the bedside14,15. It is designed in a way to function whether electric current is available or not because it runs on direct current supplied by the widely available batteries (1.5V). The kit is so simple to use by anyone as such, there is no need for a separate manpower unlike the standard centrifuge14. Therefore, our objective was to compare the haemoglobin estimation result between haemocue B-haemoglobin analyzer methods and the standard laboratory technique in our own setting. MATERIALS AND METHODS This was an experimental study conducted among the booked antenatal women at the University College Hospital, Ibadan between 1st April and 30th May 2006. An Institutional review Committee approval from the University of Ibadan/University College Hospital Board was obtained. An initial pilot study was conducted at a secondary health care facility to validate the process/protocol of the study. All consenting pregnant women were recruited for the study after explaining in detail the study protocol. Information on the age and the result of the investigation from the two methods were recorded on a proforma. Study protocol: The hemocue B – haemoglobin analyzer Method14, 15, 16,17 The patient’s finger pulp was cleaned with methylated spirit and then pricked using a lancet/needle. The initial blood was cleaned and thereafter a gentle squeeze of the finger was performed to get a drop of blood. The blood was collected by capillary action into a microcuvette and this was then inserted into the hemocue Hb 201+ automated machine system (HemoCue AB Angelholm Sweden). It uses either alternating or direct current. The haemoglobin result is then displayed after about 30 to 45 seconds in g/ dl units. The haemiglobincyanide (Standard/ traditional) Method18,19 About 2-mls of venous blood was obtained from the cubital vein of each participants into the sodium EDTA bottle and this is then transferred into the laboratory for analysis. Twenty microliters (0.2mls) of blood was taken from the bottle and this was than added to 4ml of diluent (to make 1 in 201 dilution of blood). Stopper the tube containing the solution and invert several times. Each sample was allowed to stand at room temperature for at least 3-10mins and this is to allow for complete conversion of haemoglobin to haemiglo-bincyanide. The sample was then poured into a cuvette and its absorbance in a spectrometer at 540nm or in a photoelectric colorimeter with a suitable filter was read on each occasion. Thereafter, compare the colour change against a reagent blank within 6hours of beginning the initial dilution. The haemoglobin concentration is then calculated using the formula: Alternatively the haemoglobin concentration of each solution can be read from a standard graph/table relating absorbance readings to Haemoglobin in g/dl (mg/dl) specific for each particular photometer19. Results A total of 557 antenatal clinic attendees at the University College Hospital, Ibadan were studied. The mean age of the respondents was 31.3years (SD= 6.2years) with about two thirds of women in the age group 25 to 34years (Table 1). The mean haemoglobin concentration using the standard laboratory estimation method increased with age (in five year interval) till 34years and thereafter declined. A similar trend was observed across the age group using the Haemocue – B analyzer method. (Table 2). Although, the overall mean haemoglobin concentration using Haemocue was 10.96g/ dl compared to10.78g/dl using the laboratory method (Paired t = 5.19, p = 0.000), the measurement from the two methods were strongly positively correlated (Pearson’s correlation coefficient = 0.892; p<0.0001). (Table 3) .Figure 1 also shows a scatter plot of the relationship between the two methods with a positive slope.
The time range for estimating haemoglobin (from the point of sample collection till availability of the result) using the standard method was 2 to 24-hours while the haemocue-B analyzer time was 30 to 45 seconds. Discussion The objective assessment of haemoglobin is the key to the prevention and management of anaemia in any setting. Effort has been made to ensure that appropriate technique emerges over the years that will combine the quality of comparable accuracy to the standard laboratory methods and at the same time simple and fast to deliver result with minimal or no challenges20,21. This is very important because delay in characterizing the severity of anaemia may jeopardize the entire management process especially in a pregnant woman. In addition, morbidities associated with anaemia amongst pregnant women such as abortion, intrauterine growth restriction, preterm labour, blood transfusion risks and other complications of labour could be averted when an accurate quantitative assessment of haemoglobin level is made on time and at all times. This study shows that the mean haemoglobin concentration using haemocue B analyzer was comparable with the haemiglobincyanide (standard) method despite the seemingly increase in mean values with age. This finding is similar to studies by Kapoor et al and Bhaskaram et al22,23. Although, Nguyen in 2002 examined the effects of environmental temperature changes and or humidity on the accuracy of the haemoglobin estimation among pediatric patient using hemocue B analyzer but, there has been no other reported incidence of such effect till date24. Our experience from this study revealed that haemocue B analyzer is about 1000 times faster than haemiglobincyanide method. This observation is significant because prompt availability of investigation result will drastically reduce one of the third level delays in various health facilities especially in developing countries like Nigeria. Therefore, the use of this simple automated kit in the management of obstetric emergencies including haemorrhage will be beneficial. Furthermore, we observed that there was no change in the haemoglobin value obtained from this kit irrespective of the source of power used (batteries or electric current). This further attests to the manufacturer’s claim but, the use of battery that is weak in voltage output will need to be investigated because we had no such experience in our study. Likewise, the estimation of haemoglobin using the haemocue B analyzer needs no technical dexterity for the kit to be operated unlike the standard method. Therefore, the use of this kit in rural areas where majority of pregnant women that are anaemic resides and which lack social amenities and manpower will be a ready effective haemoglobin assessment tool in their management. In conclusion, this study which to the best of our knowledge is the first in Nigeria shows that haemocue B Analyzer when properly used will provide comparable accuracy of haemoglobin estimation irrespective of source of power to it. Furthermore, it is fast and simple to use by any cadre of health care providers irrespective of location of their practice. We therefore recommend that haemocue B Analyzer kit should be adopted for haemoglobin estimation for antenatal women and labour. Acknowledgement This study was supported with grant from The Centre for Population and Reproductive Health, College of Medicine, University of Ibadan through funds from The Gates Institute, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland, USA. REFERENCES
Copyright 2008 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh08031t1.jpg] [rh08031t3.jpg] [rh08031t2.jpg] [rh08031f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}