 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
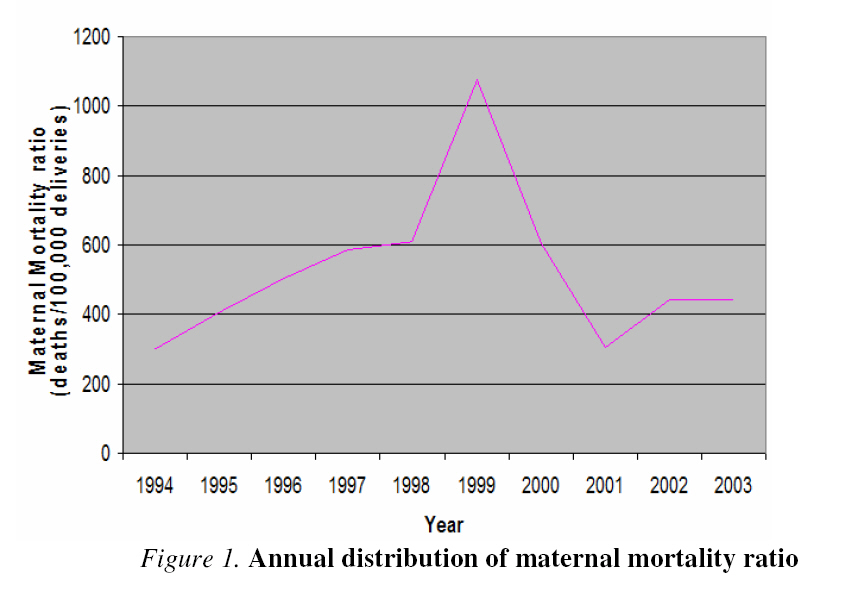
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 17-26 Original Research Article Maternal Mortality at the Central Hospital, Benin City Nigeria: A Ten Year Review Mortalité maternelle à Central Hospital, Benin City, Nigeria : Une revue de dix ansEghe Abe1 and Lawrence O. Omo-Aghoja2 1Department of Obstetrics and Gynaecology, Central Hospital, Benin City and Code Number: rh08034 ABSTRACT Maternal mortality remains a major challenge in Nigeria. This retrospective study was conceptualized to document the number and pattern of obstetric deaths at the Central Hospital, Benin City, over a ten year period, to identify common causes of maternal deaths and proffer relevant interventions. The overall maternal mortality ratio (MMR) was 518/100,000. MMR was 30 times higher in unbooked as compared to the booked patients, while 60% of maternal deaths occurred within 24 hours of admission. The leading direct causes of maternal deaths were sepsis, hemorrhage, obstructed labor and preeclampsia/eclampsia, while the major indirect causes are institutional difficulties and anaemia. Low literacy, high poverty levels, extremes of parity and non-utilization of maternity services were associated with maternal mortality. Recommendations are made for public enlightenment campaign and advocacy activities aimed at mobilizing resources for reducing maternal mortality. Also, female education and poverty alleviation programmes will contribute to the reduction of the burden of maternal mortality RĖSUMĖ La mortalité maternelle reste un défi principal au Nigeria. Cette étude rétrospective a été conceptualisée pour se documenter sur le nombre et le modèle de morts obstétriques à Central Hospital, Bénin City, au cours d'une période de dix ans, d’identifier les causes communes de morts maternelles et offrir des interventions pertinentes. La proportion de mortalité maternelle complète (MMC) était 518/100,000. MMC était 30 fois plus élevée pour des patients non réservés en comparaison des patients réservés, tandis que 60 % des morts maternelles sont arrivés dans 24 heures d'admission. Les causes directes principales des morts maternelles étaient la septicité, l'hémorragie, l’accouchement entravé et prééclampsie/éclampsie, tandis que les causes indirectes majeures sont des difficultés institutionnelles et l'anémie. L'alphabétisation basse, de hauts niveaux de pauvreté, les extrêmes de parité et la nonutilisation de services de maternité a été associée à la mortalité maternelle. Les recommandations sont faites pour la campagne d'éclaircissement publique et les activités de plaidoyer ont visé à mobiliser des ressources pour réduire la mortalité maternelle. Aussi, l'éducation féminine et des programmes d'allégement de pauvreté contribueront à la réduction du fardeau de mortalité maternelle KEY WORDS: Maternal Mortality, Benin City Nigeria, A ten year review Introduction Available evidence indicates that maternal mortality remains a major public health issue, especially in developing countries1. Globally, an estimated 585,000 women die each year from complications of pregnancy and childbirth – 99% in developing countries and 90% in sub-Saharan Africa and Asia2,3 . This translates to one maternal death every 90 minutes in developed countries compared to one maternal death every minute in sub-Saharan Africa and Asia and one maternal death every 10 minutes in other developing countries. Expressed differently, it means that maternal mortality is more than 100 times greater in developing countries than industrialized countries. Data from published Nigeria works put the maternal mortality ratio at 412 – 2420 per 100,000 total deliveries4,5,6,7 . A recent survey across the six geopolitical zones of Nigeria in 2004 by the Society of Gynecology and Obstetrics of Nigeria revealed mean maternal mortality ratios ranging from 727 to 7,523 per 100,000 live births from participating hospitals8. These figures are unacceptably high even by African standard. Existing data indicate that inadequate facilities and poor access to available services are associated with the high maternal mortality in developing countries9,10 . Major causes of maternal mortality in Nigeria are hemorrhage, sepsis, eclampsia, obstructed labor and complications of induced abortion8,11 . Anemia, malaria and chronic diseases are also commonly encountered. They operate within the context of rampaging high levels of poverty, ignorance and paucity of health facilities10,12 . Despite Nigeria being an active participant at the global safe motherhood initiative launched in 1987 in Nairobi Kenya, the indices of safe motherhood in Nigeria and indeed other developing nations have remained poor8,13. Hence the renewed UN global efforts of the Millennium Development Goals that have set out to address the key indicators of maternal mortality, with a specific target of reducing maternal mortality by 75% by the year 201514 is a very welcome development. It is our conviction that if these renewed efforts are not to go the way of previous initiatives, then a first step at systematically documenting the events and circumstances surrounding maternal deaths is a necessary prerequisite to design appropriate interventions to reduce maternal mortality in Nigeria. Yet there have not been previous efforts in doing so at the Central Hospital, Benin City. It is against this background that we embarked on this study with the aim of documenting the maternal mortality rate and pattern of obstetric deaths at the Central Hospital, Benin City, Edo State, Nigeria. Subjects and Methods This was a retrospective review of the service delivery records of patients that died in the obstetric unit of Central Hospital, Benin City from 1st of January 1994 to December 31st 2003. Central Hospital Benin City is a state government owned secondary hospital rendering obstetric care to the entire state, and serves as a referral center for other secondary and primary health care outfits. It is a 420-bed hospital with a total of 83 doctors. The Obstetrics and Gynaecology Department has a total of 10 consultants and 13 resident doctors. There are 60 nurses and supporting staff. The inhabitants of the state are mainly civil servants, traders and farmers. Of the 146 deaths that occurred within the study period, 135 (92.5%) patients’ case notes/labor ward records/theater records could be retrieved and therefore formed the basis of this study. Deaths due to abortion and ectopic pregnancy were excluded as the records of these patients could not be retrieved. For the few cases that their records were retrieved, the documentations were grossly inadequate for meaningful data extraction. A study protocol was used to extract the following information – patient’s sociodemographic profiles (age, parity, marital status of the patient, educational status of the patient and husband’s occupation), booking status, identifiable causes of death, length of hospital stay and interventions in the hospital before death. Due to refusal on the part of deceased relations or inability to afford hospital charges, post-mortem was rarely done; therefore causes of maternal death were based on clinical evaluation and diagnosis. The social class of the patient was based on the patient’s educational background and the husband’s occupation15 as recorded in the patient’s medical records. The study was approved by the human ethics committee of Central Hospital, Benin City. The data were coded and fed into computer using the SPSSPC+ statistical package. Univariate tables were generated for assessment and comparisons. Results There were 28,186 deliveries over the 10-year period and 146 maternal deaths, giving an overall maternal mortality ratio (MMR) of 518/100,000 total deliveries. However, there was marked yearly variation of the MMR and these ranged from 301/100,000 deliveries in 1994 to 1075/100,000 deliveries in 1999 (Figure 1). The trend showed a progressive increase in MMR from 1994 peaking in 1999 and thereafter underwent a progressive decline. By contrast, the delivery rates over the study period did not vary significantly. Overall, of the 135 maternal deaths reviewed, 41(30.4%) were booked giving a MMR of 338/100,000; while 94(69.6%) were unbooked giving a maternal mortality ratio of 10,732/100,000. Thus, the MMR amongst unbooked patients was about 30 times higher than in booked patients. Educational and socio-economic levels of the parturients were significantly associated with the risk of maternal death. Majority of the cases of maternal deaths were of low socioeconomic class, as 109(80.7%) of the women who died in pregnancy and delivery had no formal education or had primary level education with their husbands being low cadre civil servants or artisans. Table 1 shows other socio-demographic profiles of the women who died during pregnancy and childbirth. The modal age group of maternal deaths was 21-30, with 51.1% of the deaths occurring amongst this age group. This was followed by the age group of 31-40 years which accounted for 39 (28.9%) maternal deaths, and those that were < 20 years age represented 15 (11.1%) of the maternal mortality. The age range of the women who died in pregnancy and labour in this review was 15 – 46 years. Table 2 also depicts the parity distribution of the maternal deaths. The parity range was 0 – 14, with maternal mortality highest amongst the nulliparous population (42.2%). This was closely followed by the grand multiparous women who contributed 19.4% of the maternal deaths. The causes of maternal deaths are shown in Table 2. The four leading direct causes of maternal mortality were sepsis 37 (27.4%), haemorrhage 33 (24.4%), obstructed labour 22 (16.3%), and eclampsia/pre-eclampsia 21 (15.6%). On the other hand, the two leading indirect causes of maternal mortality were institutional difficulties (lack of power supply, lack of blood, delayed referral, delayed decision making, and inability to pay fees) in 24 (16.8%) and anaemia in 11 (8.2%) cases respectively. These institutional difficulties and anaemia as causes of death were identified from detailed notes taken and documented during the management of the pregnant women in the hospital. The mode of delivery and emergency procedures performed on the women are depicted in Table 3. Fifty seven (42.2%) of the women had emergency caesarean section; 35 (25.9%) had spontaneous vaginal delivery (SVD); while 18 (13.3.0%) died undelivered. Eight (5.9%) women had hysterectomy for ruptured uterus and uncontrollable haemorrhage. Additional, 8 (5.9%) and 3 (2.2%) women had manual removal of placenta and evacuation of retained products (ERPC) respectively. Six (4.5%) women had extensive genital lacerations repaired. Table 1: Age and parity distribution of Patients
Analysis of the duration of hospital stay before death is presented in Table 4. Over 60% (81) of the women died within 24hours of admission, while 7 (5.1%) were on admission for greater than 10 days before death. Discussion The overall maternal mortality ratio of 518/100,000 total deliveries recorded from this study is comparable with reports from earlier studies undertaken in other parts of Nigeria and some developing nations8,16-19 . It is however lower than the figures of studies from Kano and Port Harcourt respectively20,21 . It is also lower than the Nigerian national estimates22 but unacceptably high when compared with what is obtained in developed countries23,24. This review also demonstrated a trend of increasing yearly MMR from 1994 to 1999 when it peaked and thereafter it underwent a steady decline. The reduction in MMR coincided with the period when the maternity unit of the hospital secured full accreditation from the postgraduate colleges to undertake residency training. The department was therefore restructured to respond to emergency obstetric needs with accompanying increase in the number of residents (senior and junior) and consultants. This certainly improved the quality of obstetric care that would have translated to the steady reduction in MMR. Being unbooked or having not received antenatal care was an important correlate of maternal mortality in this study and this is in agreement with reports from previous works10,12,18,19 . Indeed, MMR in the unbooked was over 30 times higher than in the booked patients which underscore the need for continued health education of the populace on the importance of antenatal care and skilled attendance at birth. Also, majority of the maternal deaths occurred in women of low socio-economic group. This is consistent with the seminal work of Harrison in 1985 where he clearly demonstrated that low literacy and high poverty levels are major contributors to maternal mortality25 . Other authors have also reported same10,12,18-20,26 . Table 2: Causes of Maternal Deaths in Benin City
*Lack of power supply, lack of blood, delayed referral, delayed decision making, inability to pay fees Table 3: Mode of Delivery and Interventions before Death
Table 4: Duration of admission before death
Most of the maternal deaths occurred in those between the ages of 21 – 40 years (108 = 80%). This is however at variance with the report from Jos, North-Central Nigeria which revealed a higher maternal mortality ratio in those ≤15 years and ≥40 years, with those within the age bracket of 16 – 29 years protected from dying in pregnancy and childbirth4. And in contradistinction to the same report from Jos that showed that MMR increases with parity, our work revealed that MMR was higher at the extremes of parity. Nulliparity and grand multiparty has similarly been reported as being strongly correlated with the risk of maternal mortality in other studies similar to what we found in this review10,17,20,26 . The leading direct causes (sepsis, haemorrhage, obstructed labour and eclampsia/pre-eclampsia) of maternal deaths from this study are similar to those reported from other parts of Nigeria and sub-Saharan Africa4,13,16-21,27,28 . This was the situation before the safe motherhood initiative and has remained so despite this global effort. On the other hand, when we evaluate the indirect causes of maternal mortality, institutional delays which constituted lack of power supply, lack of blood, delayed referral, delayed decision, the making and hospital policy of “cash and carry” as a basis for treatment of patients even in the face of dire emergency, accounted most significantly as background cause of maternal mortality in this category. Overall, it contributed 16.8% of maternal deaths in Central hospital, Benin City. Interestingly, malaria as a cause of maternal mortality was not documented in this study. However, we were unable to exclude for certain the association of malaria with anaemia in pregnancy (a strong possibility) which accounted for 8.2% of maternal deaths in this series. It is also interesting to note that HIV/AIDS was not documented in this report because within the period under review the hospital had not put in place strategies for counseling and screening for HIV in pregnancy. Therefore the possibility of HIV/AIDS having contributed to complications such as sepsis, postpartum haemorrhage, complications of caesarean section and anaemia cannot be ruled out, particularly when reports have indicated that HIV/AIDS contributes to indirect causes of maternal death in pregnancy and child birth4,29,30 . Majority (81%) of the maternal deaths in this review occurred within the first 24 hours of arrival in the hospital, implying that most of the cases arrived moribund when their situation was already very critical. This is similar to the finding by Ujah et al in their 17-year review of maternal mortality in North-Central Nigeria and other similar studies4,19.Onwuhafua in his publication “dying undelivered” described maternal death with the baby insitu as a double tragedy because the unborn baby died prematurely31. This situation was recorded in our series with 18 (13.3%) of the women who died doing so with their baby undelivered. Similar situation have been reported in previous studies4. We totally agree with Ujah et al in their assertion that early recourse to postmortem caesarean section could spare such babies and that the issue of pregnant women dying with the baby insitu is an indictment on the health care delivery system4 . Conclusion MMR remains high in Benin City despite a downward trend in its pattern since 1999. The figures are about 30 times higher in the unbooked patients and 60% of maternal deaths occurred within 24 hours of admission. Low literacy, high poverty levels, extremes of parity and non-utilization of maternity services are significantly associated with the risk of maternal mortality. The leading direct causes of maternal deaths are sepsis, haemorrhage, obstructed labor and preeclampsia/eclampsia, while the major indirect causes are institutional delays and anaemia. Recommendations If the desired target of the Millennium Development Goal of reducing MMR by 75% in the year 2015, and reversing the worsening trend must be achieved in Benin City (and by extension in Nigeria), a multifaceted approach is recommended for urgent attention. Clearly, as a first step in this direction, a strategic plan should be put in place for public enlightenment campaign and advocacy activities aimed at mobilizing resources for reducing maternal mortality. Additionally, the introduction of widespread use of parthographic monitoring of labour will lead to a reduction in the incidence of prolonged obstructed labour, which is known to contribute to sepsis – the leading cause of death in this series. Efforts should always be made to prevent, minimize and combat sepsis when it does occur. We advocate for training, retraining and continuing medical education for private practitioners and other maternity care providers within Benin City and its environs on emergency obstetric care. Making maternal health care free will increase prompt utilization of these services. Finally, female education and poverty alleviation programmes will contribute to the reduction of the burden of maternal mortality. References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08034f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}