 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 50-58 Original Research Article Prevalence and Prevention of Malaria in Pregnancy in Edo State, Nigeria Wagbatsoma V.A1 and Omoike B.I2 1 Department of Community Health, School of Medicine, College of Medical Sciences, University of
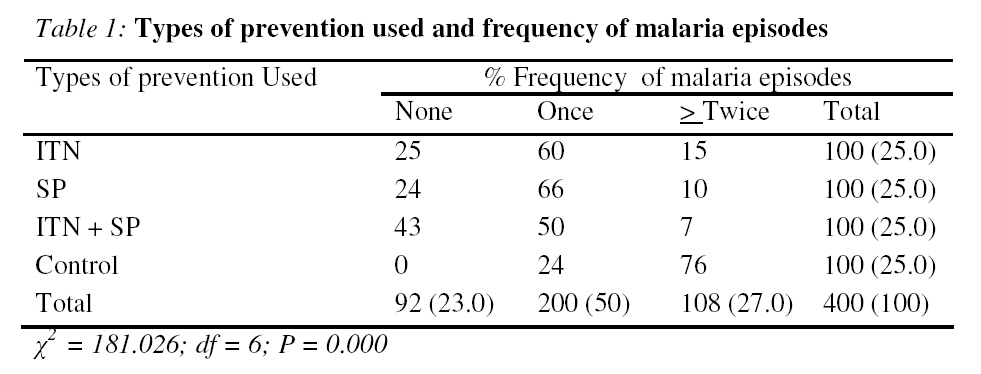
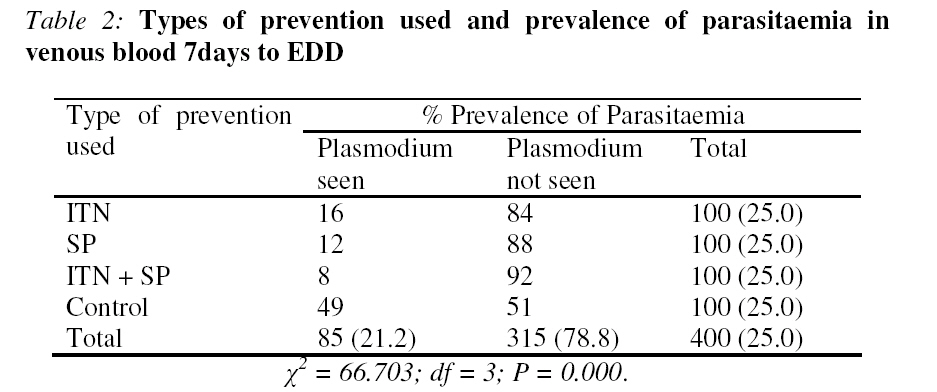
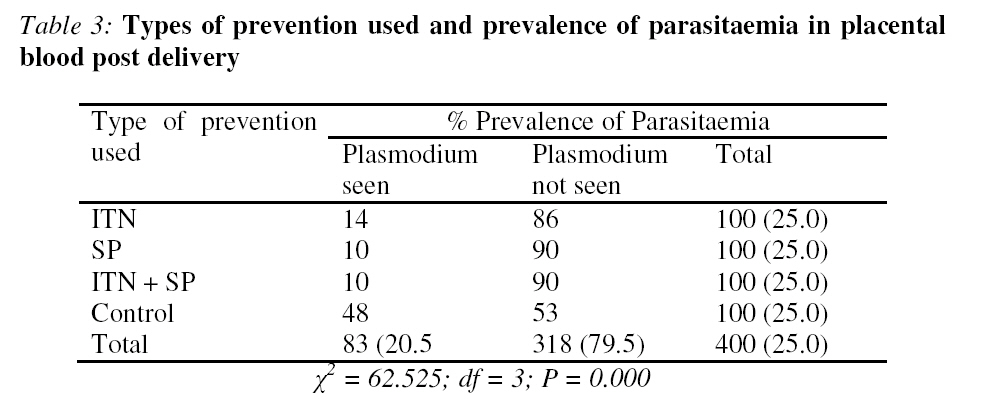
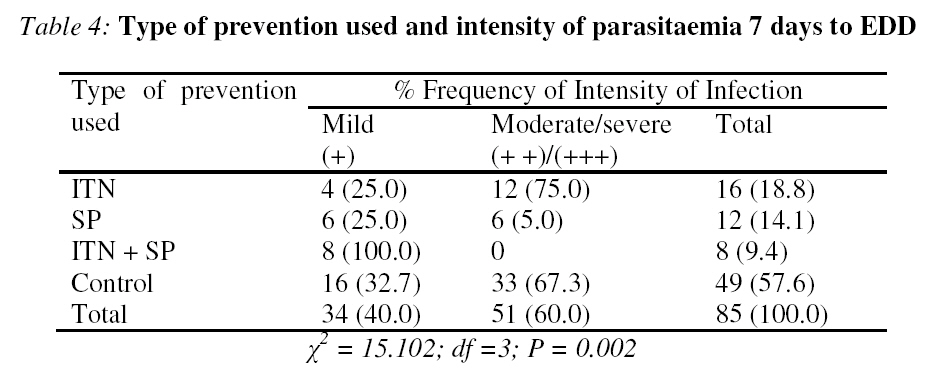
Benin, Benin City, Nigeria, Code Number: rh08037 ABSTRACT The observational/longitudinal study was undertaken in Igueben Local Government Area (LGA), Edo State, Nigeria. The objective of the study was to determine the effect of prevention on the prevalence of malaria during pregnancy. The study population comprised 4 groups viz; Group1, had 100 women protected with Insecticide Treated bed Nets (ITNs); Group2, another 100 treated with Sulphadoxine – pyrimethamine (SP); Group 3, 100 protected with both ITN and SP, while Group 4, were 100 unprotected others who served as control. Venous blood was collected 7 days to expected date of delivery while placental blood was collected after delivery from the subjects for parasitaemia determination. Findings showed that all protective devices used were effective against malaria. Prevention used against malaria in pregnancy is a sure safe guard against maternal morbidity/mortality and should be encouraged. It is therefore, recommended that pregnant women should be health educated to appreciate the need for malaria prevention RĖSUMĖ Fréquence et prévention du paludisme dans la grossesse dans l’Etat d’Edo, au Nigeria L'étude d'observation/longitudinale a été entreprise dans la région locale d’Igueben de l'État d’Edo, Nigeria. L'objectif de l'étude était de déterminer l'effet de prévention sur la fréquence du paludisme pendant la grossesse. La population d'étude y compris 4 groupes à savoir : Groupe 1, qui avait 100 femmes protégées par les moustiquaires traités à l’insecticide (MTI); Groupe 2, d'autres 100 ont été traitées à Sulphadoxine -pyrimenthamine (SP); Groupe 3, 100 protégées tant avec MTI qu'avec SP, tandis que le Groupe 4, étaient 100 autres femmes non protégées qui se sont servies du contrôle. Le sang veineux a été recueilli 7 jours avant la date d’accouchement tandis que le sang du placenta a été recueilli après l’accouchement des patients pour la résolution/détermination de parasitaémie. Les résultats ont montré que les appareils protecteurs utilisés étaient efficaces contre le paludisme. La prévention utilisée contre le paludisme pendant la grossesse est une sécurité bien sauf contre la morbidité/mortalité maternelle et doit être encouragée. C’est ainsi recommandé que les femmes enceintes doivent prendre des leçons de santé afin de pouvoir apprécier la nécessité de la prévention du paludisme KEY WORDS: Malaria, Pregnancy, Prevention (ITN, SP, ITN + SP), prevalence, PHC Introduction Maternal mortality is a major health problem in developing countries including Nigeria. Malaria due to Plasmodium falciparum in pregnancy is an important and major contributing factor to the high maternal morbidity and mortality in sub-Saharan African1,2 and about 47%3 of pregnant women are diagnosed with malaria in Nigeria. Pregnant women compared to nonpregnant women are at an increased risk of malaria and the severity of the clinical manifestation experienced by these women and their foeti depend on the level of pre-pregnancy immunity4. In areas of stable malaria transmission, the population is constantly exposed to intense transmission due to frequent infective Anopheles vector bite. Under such condition significant immunity develops among the adult population with children under five years and pregnant women being the most affected. Pregnant women are more susceptible to Plasmodium falciparum infection with more frequent episode of clinical malaria, increased prevalence and density of parasitaemia during episode5,6 . The effect of infection on the pregnant is dependent on pre-pregnancy immunity. This acquired anti-malarial immunity depends on intensity of transmission and the number of previous pregnancies among others. In areas of stable malaria transmission, the ill health effects are particularly apparent in the primigravida, and secondigravida7. Previous studies have shown that prevalence of infection is highest in secondigravida while others have reported a higher prevalence in primigravida and the density of parasitaemia is reported to be highest in the first trimester and primigravida could be at maximum risk in highly endemic areas8,9 . Also multigravidae with HIV infection are similar to primigravidae without HIV infection in terms of susceptibility to and negative consequences of malaria10. However, in areas of unstable transmission exposure is infrequent and people of all ages are at risk of severe malaria. In such areas pregnant women also suffer more severely than nonpregnant adults with about 3 to 4 times the risk of developing severe malaria and death11,12 . Placental parasitaemia in pregnant women lead to impairment of foetal nutrition and this contributes to low birth weight, a leading cause of poor infant development and survival in Africa13,14 As a result of the increased risk of malaria during pregnancy; WHO recommended a three pronged approach to the strategic framework for malaria prevention and control during pregnancy in areas of stable transmission in Africa. These include the use of intermittent preventive treatment (IPTp), insecticide treated bed nets (ITN) and effective case management of malaria illness and anaemia7. Unlike the prophylactic antimalarial drugs that are given at less than therapeutic dose at regular interval that could encourage parasite resistance, (IPTp) using sulfadoxine-pyrimethamine (SP) employs a therapeutic dose regimen with only two doses at monthly interval during the course of pregnancy which effectively reduces parasite load. Similarly, insecticide treated bed nets reduce human vector contact by physically excluding vector mosquitoes, killing them if they land on it or repel them, thereby driving them from the vicinity of the sleeper. The use of ITN benefits the pregnant woman as well as her family by reducing malaria related illness and death16,17. These efforts are geared towards making pregnancy safe. The (IPTp) strategy assumes that every pregnant woman living in stable malaria transmission area has malaria parasite in the blood or in placenta and therefore should have full treatment doses of antimalaria at specific interval during the second and third trimesters to reduce the effect on mother and foetus. It has been reported that (IPTp) with SP can effectively reduce parasitaemia, improve birth weight and reduce severe anaemia in primigravidae15,18 . Focused ante – natal care19 recommends 4 ante – natal visits for normal pregnancies .The major goal of the focused ante – natal care is to help women maintain normal pregnancies through identification of pre – existing health conditions, early detection of complications arising during pregnancy, health promotion and disease prevention and birth preparedness and complication readiness planning. Health promotion and disease prevention include protection against malaria through intermittent preventive treatment and insecticide treated bed nets in areas of high prevalence of malaria. Similarly, the use of ITN during pregnancy in stable malaria transmission zone reduces the overall risk of morbidity and mortality among pregnant women and their infants. Studies in Kenya16 and Gambia20 showed that the use of ITN during pregnancy reduced the prevalence of malaria and premature babies. The African Heads of States declared in Abuja (Nigeria) that by the end of 2005 at least 60% of all pregnant women at risk of malaria, especially those in the first pregnancies, have access to intermittent preventive treatment. Unfortunately, use of ITN and IPT with SP as prevention against malaria in Nigeria is still very low17. However, in Igueben Local Government Area (LGA), the government and a non-governmental organization (NGO) collaborated to distribute ITN to pregnant women who attended ante-natal clinic in the Primary Health Care (PHC) Centres for the first time and mothers who have completed the immunization of their babies free of charge. Also IPT with SP was administered to pregnant women that attended ante-natal Clinic in the LGA who could afford the cost of the drug. The observational/longitudinal study seeks to determine the effectiveness of these preventive measures against malaria during pregnancy in Igueben LGA. Igueben is a rural community and such communities are usually associated with high fertility and maternal mortality rates due to poor health services, and other socio-cultural factors. Now that these services are available in the local government area which has been designated a model LGA with assistance from some NGOs, it would be useful to assess the effectiveness of the malaria control programme. This is aimed at comparing the findings with those from other areas where the programme is established. Material and Methods The study was undertaken in Igueben LGA which is predominantly rural, within the rainforest and stable malaria transmission belt of Edo State, Nigeria. The inhabitants are mainly Esan speaking and subsistent farmers. The study was conducted between April and December, 2005. There were 8 Health Centres A – H located in each of the communities that constitute the LGA. The survey was an observational/longitudinal type in which respondents were followed up till delivery. The programme of malaria prevention was already on ground in the LGA assisted by an NGO. All that was done was to select the respondents within the clinics based on the type of preventive services they received from the LGA. The researchers did not administer the devices or manipulate any intervention between groups, but rather assessed the effect of the use of the provided devices on the prevalence of malaria. The health Centres are located in the various communities and within walking distances. Antenatal attendance for pregnant women in their first and second trimester in each centre per month were: A, 90; B, 84; C, 78; D, 78; E, 72; F, 72; G, 66; H, 60 giving a total of 600. Sample size was derived using 47%3 prevalence of malaria in pregnancy giving 383.To achieve a 90% response rate 383 was divided by 0.9 to give 425. However, only 400 agreed to participate in the study giving 94.1% response rate. Using a sampling fraction of 400/600 ; the following samples were selected within each health centre A,60; B,56; C, 52; D, 52; E, 48; F, 48; G, 44; H, 40. These pregnant women were selected by simple random sampling method within clinics (balloting) using the attendance list as sampling frame. Four hundred pregnant women in their first and second trimesters who received ante-natal services in the PHC Centres were recruited for the study with their informed consent. The subjects were informed about the details of the study and their expected level of participation. Informed consent was given verbally by the respondents. They were informed that they had the right to withdraw at any time without any penalty. Only ITNs were provided free, sulfadoxine-pyrimethamine was given to those who could afford the cost. At the time of the study ITNs were in short supply from the NGO and the last supply from government was in 2004. The control was those who could not benefit from the distribution of ITNs and could not afford to buy SP at the time of the study but were not deliberately denied access to the preventive devices. The 100 subjects per group was rounded up for convenience. They were grouped into 4 categories by the type of preventive device used. Group 1: comprised 100 pregnant women who slept every night under ITN during the period of the study and were monitored through home visit by Community Health Extension Workers (CHEW) to ensure that the ITNs were in place for use. However, nightly use of ITNs was by self reporting by the users to the (CHEW) weekly during the day. Group 2: comprised 100 of them who were administered with 2 therapeutic doses of sulfadoxinepyrimethamine (SP) at monthly interval. The first dose was administered after quickening was confirmed. Quickening was confirmed by the doctor. Quickening is defined as ‘the first perception of the baby’s kicking and movement2 and this usually occurs between 14 – 26 weeks of pregnancy. Each pregnant woman was provided with three tablets of SP with a glass of water and observed by a nurse to ensure tablets were swallowed. Date of first treatment was recorded, subjects were asked to report any feeling or reaction after treatment. Four weeks later the second dose was administered. Group 3: were 100 pregnant women who slept every night under ITN and also received 2 therapeutic doses of SP. Group 4: these were 100 pregnant women who received no form of protection and served as control. The control subjects were not denied access to the devices but that they had not received ITNs due to short supply at the time of the study and could not afford the cost of SP. Users of (ITPp) were those who could afford to purchase the drug since it was not given free to the pregnant women. However, they were treated whenever, they had malaria attacks. These pregnant women were followed up till when they delivered their babies and none of the subjects dropped out of the study. All participants were advised to report all cases of ill health to the team doctor for proper management. Two cases of diarrhoea were reported and managed. Subjects were advised not to take any form of prophylaxis (in form of either orthodox drug or herbal preparation) during the study period. They were advised against the use of herbal preparation and not herbs. Venous blood was collected from each of the subjects, 7 days before expected date of delivery while placental blood was collected after delivery into sequestrene bottles by the Medical laboratory scientist who also prepared and examined the films. Thick and thin blood films were prepared, stained and examined as described by WHO21. The women registered for the survey were those already attending the ANC, had identification numbers and were located in the clinics and no transportation expenses were incurred because health Centres were located in the community. The questionnaire was administered by trained personnel recruited from the LGA. They were trained on good attitude towards the respondents, understanding of questionnaire, pre-testing and its precise application and checking after administration for correctness. Data collected were analysed using PEPI22 the computer programme for epidemiological studies. Association was established using Chi-square test for statistical significance at 95% confidence limit. Results Findings from the study showed that protective devices used were effective in reducing the frequency of malaria episodes. Malaria episodes were determined clinically and parasitologically. Ninety-two (23.0%) of the pregnant women protected by each of the devices had no malaria attacks during the period of pregnancy, 200 (50.0%) experienced only one attack while 108 (27.0%) experienced 2 or more episodes of malaria and the association was found to be statistically significant (P = 0.0000) as indicated in Table 1. All the control subjects experienced malaria attacks during the course of pregnancy. Twentyfour percent experienced one episode while 76% had 2 or more attacks. There was a statistically significant difference in the frequency of malaria episodes when that of control was matched with the frequency of different devices used. (ITN, P = 0.000; SP, P = 0.000; ITN, + SP, P = 0.0000). There was also a statistically significant difference between frequency of malaria attack between ITN + SP and ITN and SP alone (P=0.014; 0.017) but there was none between ITN and SP (P=0.520). This suggests that the use of any of these devices confers effective protection against malaria. Table 2 shows that the overall prevalence of parasitaemia in venous blood was 85 (21.2%) while Plasmodium falciparum was the only specie found in the blood films examined. Prevalence of parasitaemia reduced remarkably with the use of protection and was also found to reduce with type of device used and the difference was found to be statistically significant (P=0.0000). Prevalence of infection was highest among the control subjects, 49%. There was also a significant difference between the prevalence of parasitaemia in control group and that of users of the various protective devices (ITN, P = 0.0000; SP, P = 0.0000; ITN + SP, P = 0.0000). However, there was no statistically significant difference between the prevalence of parasitaemia among users of ITN + SP, ITN or SP alone (P=0.082; 0.346; 0. 415). The prevalence of parasitaemia in placental blood was 82 (20.5%). The use of protective devices and specific types of devices used was found to reduce the prevalence of infection appreciably and the association was found to be statistically significant (P = 0.0000) as indicated in Table 3. Similarly, when the prevalence of parasitaemia in control was compared with that of individual protection used a statistically significant difference was found (ITN, P = 0.0000; SP, P = 0.0000; ITN + SP, P = 0.0000). Intensity of parasitaemia decreased with the use of prevention and type of device used and the difference was found to be statistically significant (P = 0.002) as indicated in Table 4. Thirty-four (40.0%) of the pregnant women had mild infection while 51 (60.0%) were moderately/severely infected. Only 8 (100%) of users of ITN + SP had mild infection while 6 (50%) each of those who used SP had mild and moderate infections respectively. However, as expected 33 (67.3%) of the controls had moderate/severe malaria but surprisingly, users of ITNs, 12 (75%) also had moderate/severe malaria. Accordingly, there was no statistically significant difference between the intensity of parasitaemia in the control group and ITN (P=0.565), and SP (P=0.262) but was statistically significant for ITN + SP, (P=0.000) as indicated in Table 4. Discussion The use of ITN, SP and ITN + SP were observed to be highly effective in reducing the episodes of malaria among the pregnant women. Previous studies revealed similar outcome with the use of ITN in Kenya16 and SP in Malawi23 . Meanwhile, the combination of ITN + SP was found to be most efficacious of the devices used in protecting the pregnant women24 than either the ITN or SP alone. However, the cost of combining these devices may affect the use except for the affluent. The fact that 76% of the control had two or more clinical attacks of malaria during the course of pregnancy underscores the importance of malaria prevention during pregnancy. There is the urgent need to encourage the pregnant women on the necessity to use any of these devices through appropriate health education to ensure safe motherhood. Plasmodium falciparum was the only specie found in the blood films examined5,6. This prevalent specie of malaria parasite attacks both young and old red blood cells causing severe consequences on the unprotected victim. The prevalence of malaria in this study was 21.2% for peripheral blood, higher than 17% reported among pregnant women attending ante –natal clinic in India25. This could be due to the location of the study area within the rain forest belt where transmission is perennial. The high prevalence of 49% parasitaemia in the peripheral blood of the control was higher than 47%3 reported for pregnant women in Nigeria. The 49% prevalence could be considered a high risk, which could have dangerous consequences such as anaemia and low birth weight among others but for immediate treatment administered when signs/symptoms of malaria were reported. Fortunately, the prevalence of parasitaemia was reduced following the use of protective devices. This observation corresponds with earlier studies with use of ITN in Kenya16 and Gambia20 and SP in Kenya15,18. The overall prevalence of placental parasitaemia was 20.5%. The high prevalence of placental infection of 48% observed among the control could be harmful to the foetus. It could interfere with the function of nutrient transportation by the placenta, impairing nutrient flow to the foetus thereby retarding growth and development resulting in low birth weight, still birth and peripheral death. Evidence from the study indicated that the use of any of the devices could abate the incidence of these outcomes during pregnancy. The prevalence of placental parasitaemia was 10% among subjects who used SP (IPT). This observation is lower than reports from similar studies in Malawi23 where placental parasitaemia reduced from 32% to 23% using SP and in Gambia26 from 29% among those who received placebo to 4% in those who were treated with maloprim. The use of SP as prevention against malaria in pregnancy can be regarded as effective, cheap and tolerable as no reaction against SP was reported. Although the intensity of infection decreased with the use of protection, it was surprising that 2 (11.8%) of those who reported that they slept under ITN at night had moderate/severe parasitaemia. Effective prevention against malaria reduces intensity of infection15 as observed in this study. It is possible that these may have defaulted in the use probably due to poor installation of ITNs. It is also likely that the pregnant women who complained of heat while sleeping under the net at night exited the net to overcome heat. It is also probable that they did not comply as much as reported. However, it could be unethical to interrupt the privacy especially that of couples who have retired to bed in order to ensure compliance to ITN usage. This is a limitation in the study; compliance to ITN usage would have been better assessed if the study was facility based where nightly usage could be effectively monitored. It is therefore suggested that the health education at the ante-natal clinic should include the effective installation and proper use of ITN to ensure expected result. The strategic framework for malaria control during pregnancy in Africa which includes the use of Insecticide Treated Bed Nets and Intermittent Preventive Treatment with SP among others is low in Nigeria and needs to be stepped up. Prevention used against malaria in pregnancy is a sure safeguard against maternal morbidity, mortality and foetal death and should be encouraged. Although, the discomfort associated with the use of ITN during pregnancy and the cost of combined protection could affect compliance, it could be overcome. It is therefore recommended that pregnant women should be health educated to appreciate the use of these protective measures and these should be provided at subsidized cost to ensure compliance. References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08037t2.jpg] [rh08037t4.jpg] [rh08037t1.jpg] [rh08037t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}