 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
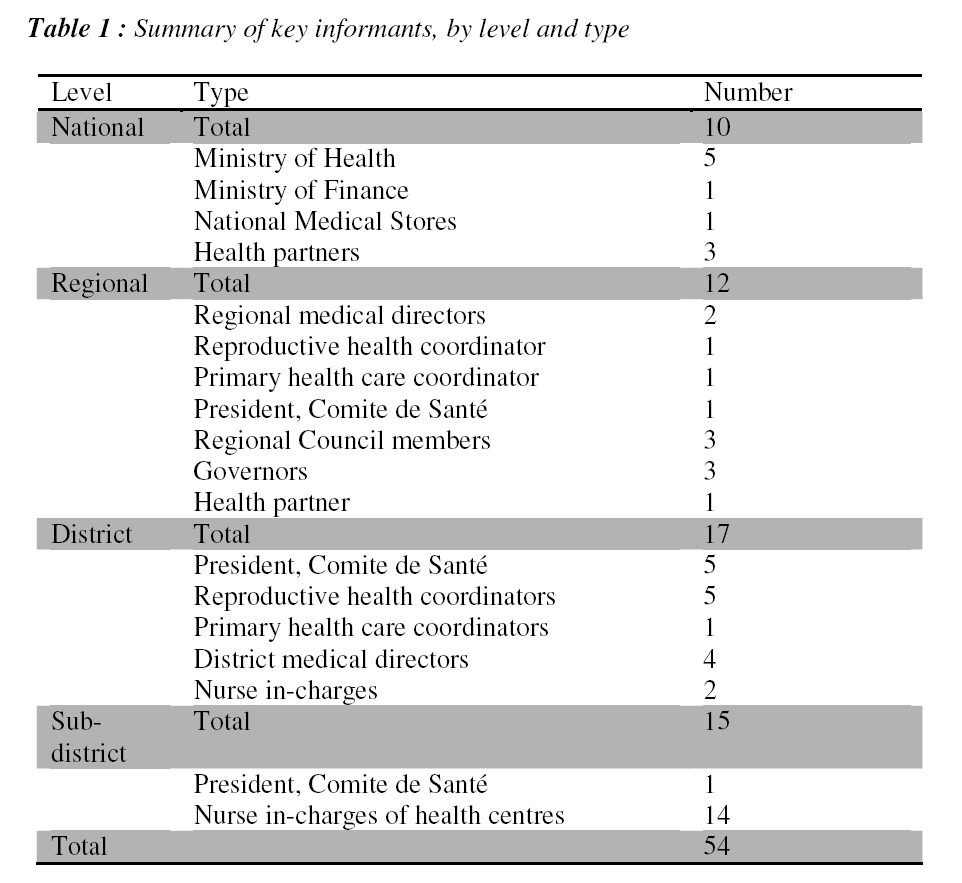
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 93-111 Original Research Article Key Informant Views of a Free Delivery and Caesarean Policy in Senegal Sophie Witter1 and Mohamed Diadhiou1 1 Immpact, Health Sciences Building, Foresterhill, University of Aberdeen, AB25 5DZ, Scotland, Code Number: rh08040 ABSTRACT This article presents the findings of one component of an evaluation of the national policy for free deliveries and caesareans in Senegal. The policy was introduced in 2005 in five more deprived regions of the country. It aimed to reduce the financial barriers to using maternity services and to increase the number of facility-based deliveries. The findings are drawn from 54 semi-structured interviews with key informants who had technical and administrative or political responsibility for the policy at national, regional, district and health post level. These were carried out from November 2006 to January 2007. The evaluation findings emphasise the importance of careful planning and communication before a major national policy is implemented, and also of simple and clear definition of the package of ‘free’ services on offer. Long term investment in supply will also be needed to increase access for the most remote areas (Afr J Reprod Health 2008; 12[3]:93-112). RĖSUMĖ Les vues d’informateur clef d’un accouchement gratuit d’une politique césarienne au Sénégal Cet article présente des constatations d’un composant d’une évaluation de la politique nationale sur les accouchements gratuits et césariens au Sénégal. La politique a été introduite en 2005 dans cinq régions défavorisées du pays. Il a comme but de réduire les barrières financières d’utiliser les services maternels et d’augmenter le nombre d’accouchements à l’aide des installations. Les conclusions sont tirées de 54 interviews demi-structurées avec des informateurs clefs ayant des responsabilités techniques, administratives ou politiques pour la politique au niveau national, régional, au quartier et au poste sanitaire. L’étude a été entreprise du novembre 2006 au janvier 2007. Les conclusions évaluées soulignent l’importance du planning soigneux et la communication avant l’application d’une politique national majeure ainsi que de la simple définition claire de la présentation des services ‘gratuits’ en demande. L’investissement en offre à terme long sera important pour augmenter l’accès pour des régions isolées (Afr J Reprod Health 2008; 12[3]:93-112). KEYWORDS: Deliveries, Caesareans, Fee exemption, Senegal, Key Informants Background The Millennium Development Goals set a target of reducing maternal mortality ratio by three quarters by 20151. However, progress towards this goal has been disappointing. The maternal mortality in many countries, especially in Sub-Saharan Africa and Asia, has stagnated or even deteriorated2. Furthermore, there are huge rich-poor inequalities in access to maternal healthy care and in maternal mortality3,4 . To achieve the fifth Millennium Development Goal, it is essential to address the financial barriers which are a significant factor in the low uptake of skilled care for deliveries and emergency obstetric care5. This has led to a growth in experimentation with different financing approaches focused on maternal health care, ranging from social health insurance in countries like Bolivia6 to vouchers for delivery and transport costs in countries like Nepal7 and national fee exemption policies in countries like Ghana8. There is considerable international interest in evaluating the different approaches and assessing which ones are most effective in different contexts9. Senegal is a West African country, with a surface area of just under 200,000 square kilometers. Its population was estimated at 10.6 million in 2005. Its GDP per capita, according to the OECD, was $497 in 2007. The health care infrastructure is well below international norms and not evenly distributed, with some of the most remote areas least well covered. For hospitals as a whole, the ratio is one per 500,000 inhabitants for the whole country (ranging from one per 300,000 in Dakar to one per more than a million in Kaolack)10. For health centres, the overall ratio is one per 193,000 inhabitants (higher than the WHO norm of one per 50,000 and the national norm of one per 150,000), while for health posts, the ratio is one per 13,000 inhabitants (in relation to a WHO norm of one per 10,000). There are also shortages and skewed distribution of personnel, which has led to recent training activities in obstetric care. Senegal currently has 1 doctor per 17,000 inhabitants; 1 midwife per 4,600 women; and 1 nurse to 8,700 inhabitants11 . Of the 56 health centres operating in 2006, only 12 were able of offer comprehensive emergency obstetric care services. Public service provision dominates, particularly outside Dakar, although the Catholic Church and some NGOs also offer limited services in some areas. Maternal mortality is high in Senegal, at an estimated 401 women per 100,000 births12. Moreover, there are considerable internal disparities, from 123 per 100,000 births in Dakar to 743 per 100,000 in Tambacounda. This is partly attributable to place of delivery: 37% of women deliver at home12 . For the poorest quintile, 70.2% deliver at home, compared with only 5.7% for the richest. In terms of attendants at the birth, 51.9% are attended by ‘skilled personnel’ (doctor, nurse, midwife or auxiliary midwife). Again, rates are closely linked to socio-economic group. Only 7.5% deliver with a TBA, but 35.7% are assisted by a relative or other person (and 4.2% delivery alone). Caesarean section rates are 3.3% nationally, but with wide regional and socio-economic variations. In Dakar, more than 10% of last deliveries were caesarean sections12 , while in Matam the figure was 0.5%. Rates rise with economic status and educational level. This article presents the findings of one component of an evaluation which was carried out in Senegal in 2006-7 of the national policy for free deliveries and caesareans. The policy was introduced in 2005 in five more deprived regions of the country (Tambacounda, Ziguinchor, Matam, Kolda, and Fatick). It aimed to reduce the financial barriers to using maternity services and to increase the number of facility-based deliveries. This was assumed to lead to a reduction in maternal and prenatal mortality. The strategy for doing so was to offer free caesareans at regional hospital level and health centre II level, and free normal deliveries at health centre I and health post level. This was funded by the national government, which transferred funds to the regional hospitals to reimburse them for lost caesarean revenues, and transferred kits to the health centres and health posts to cover the input costs of deliveries. In 2006, the policy was extended to regional hospitals in the remaining regions (excluding Dakar). The participating institutions are all in the public sector, but do not include the Cases de Santé, which are grassroots level structures providing normal deliveries via Matrones1. The private and traditional sectors are not included. Methods This article presents the findings of the key informant interviews, which were carried out from November 2006 to January 2007. The aim of the key informant (KI) interviews was to provide understanding of the fee exemption policy and how it has been implemented at different levels of the health system. This includes investigating how it is perceived by different stakeholders in the health system; what factors influence its implementation; whether there are significant variations by locality; how it is affecting different actors; and whether the policy is likely to be sustainable. Sampling for KI interviews is purposive, selecting those individuals who are likely to be knowledgeable about the area of enquiry. We interviewed 54 individuals with technical and administrative or political responsibility for the policy at national, regional, district and health post level (see Table 1). All interviews were conducted in French. Data analysis has been carried out manually and thematically, using the framework of questions posed and any additional themes that emerged. Researchers looked for similarities or differences between levels, areas and types of KI. Together with other evaluation components (focus group discussions at community level; financial analysis; and analysis of clinical findings), they contribute to an overall evaluation of the effectiveness and cost effectiveness of the policy. Results The findings are divided into five areas. The first deals with the aims of the policy and the process of its introduction. The second covers implementation issues. The third focuses on its perceived impact. The fourth covers stakeholders’ overall assessment of the policy. The fifth summaries their recommendations for the future. There is inevitably some overlap and linkages between these areas. Establishment of the policy The KI had a clear understanding of the policy’s goals. “It aims to reduce maternal and neonatal mortality by facilitating access to health services, since poverty and the high cost of services hold back access to facilities, which explains why home births are numerous” (regional KI). The process of establishing the policy was described, including the setting up of a steering committee, dialogue with stakeholders, and a technical working group to advice on kits. However, some limitations became apparent early on. One KI mentioned the absence of an overall document describing the policy. Other issues raised included the switch in the first year of leadership from the primary health care department of the Ministry to the reproductive health unit. The PNA was also given very short notice to prepare kits in time for the start of the policy in 2005, which caused delays in roll-out. The decision to expand the policy to the regional hospitals in the remaining regions was, according to one KI, informed by budget under-spend for 2004 and 2005, indicating that lack of funds at national level was not a constraint. After a review meeting in July 2006, the government responded to some of the issues being raised about contents of kits by agreeing to supply kits for complicated deliveries (in addition to normal delivery, and caesarean kits). Dissemination was carried out effectively through official, hierarchical channels, according to KI, who also described a wide variety of methods used to communicate the policy to communities. The KI felt that communities were well informed but that there still existed barriers to uptake, particularly distance and household preferences. “Everyone knows of it, but the problem is how to reach the health posts when you live in a distant village and your only means of transport is the cart. The people living around the post respond well. The media have broadcast it, and much more information has gone out via the teams that promote it” (facility KI). While well disseminated, the policy was not well understood, and KI highlighted a number of misunderstandings and ambiguities relating to it. Some, for example, cited beliefs that it was only covering caesareans, or that it also included antenatal care, or that normal deliveries carried out in hospitals were included. Providers clarified that the following types of care or items are not free: antenatal care, postnatal care, abortion, newborn care, and transport to facilities, other conditions in pregnancy (e.g. malaria), food in hospital, and prescriptions for items not included in the kit. The consensus then is that only the ticket price and the items which are covered by the kits are free. One KI even reported that clients were charged tickets for hospitalization, while another stated that only the act was free (i.e. none of the materials costs). “It has not been widely diffused because there is still a need for public awareness. Women and people in general, do not know the limits of what is free. There is confusion due to believing that the policy applies to the woman and her baby. What is free is the delivery. Ante-partum and post-partum are at their expense and this information they only receive from staff” (district KI). Implementation Issues According to national KI, kits were allocated according to national costing and experience and the budget was adequate at the start, though it failed to grow as the scale of implementation grew. The KI described a clear system for mandating and sending funds for the Central Medical Store (PNA) and the regional hospitals. However, no such clear system existed for the flow of kits and funds to district level and below. There was no mechanism to transmit funds to these levels to compensate for labour and facility costs. The regional hospitals complained of poor management and delays in funding, with funds arriving in November of 2005 and 2006 (for a financial year starting in January). There were also reports of kits sitting in the regional medical stores for long periods. There were misunderstandings relating to the caesarean kits, which the PNA manufactured for the regional hospital and health centres, while the regional hospitals made up their own. There were therefore excessive caesarean kits in the system, which were given to the regional hospitals in the end, in addition to the cash reimbursements for caesarean sections. Regional KI reported that kits were distributed to districts and hospitals according to a national list, in return for monthly accounting. The districts, however, were less clear about the rules, saying that they had received no communication about how kits were allocated, nor any feedback on their reports. They said that there were delays with kits and that kit supplies were unpredictable. This was confirmed by the sub-district KI, who suggested better planning of kits, which were not currently linked to demand at facility level. In addition, they raised the issue of reimbursement for other costs of services (beyond the few material supplies contained in the kits). “We ourselves were unclear as to how payment would be made for the kits. Since the policy came into force we have not received a single cent in reimbursement. In any case, we do not really know what procedure to follow for reimbursement” (district KI) KI concurred that there were not enough normal delivery kits, especially in the first year of operation. As for caesarean kits, these were considered adequate. At district level, only one out of ten KI thought that the number of kits had been adequate. The consequence, according to most, was that women had had to pay for supplies, being exempted only for the ticket. Eight out of nine at sub-district level were also of the view that stocks had been inadequate, though they reported an improvement over time. Stock-outs lasting months were reported by some, which led to charging for all items, unless the facility was able to supply some items from their stocks. One facility reported that it had only ever received one consignment of kits. “There were constant shortages. They were very, very frequent. When there was a breakdown in supply, advance financing was requested of the authorities” (national KI) The national level KI were aware of the limitations of the content of kits, but pragmatic about what could be included. “It’s relative. It depends on the budget; there are certainly things that are not contained in the kits, but then it’s a question of what’s possible” (national KI). At lower levels, though, there was more dissatisfaction with the contents. KI called for more kits to cover complicated deliveries, more items for post-natal care and disinfectants. Sub-district KI were unhappy with some of the items included, which were judged not to suit local customs. Regional KI reported a number of types of payments which households continued to make under the policy, including for medicines, when kits are inadequate or exhausted; for tickets (in Matam); and for caesareans in Ziguinchor, if the household is relatively well off. (Since June 2006, Ziguinchor has had to apply the free caesarean policy selectively, because of shortages of funds.) At district level, most reported that the ticket cost and supplies in the kits are free. However, even where this is the case, households are continuing to pay around 3,000 FCFA for normal deliveries without complications. Only one KI at district level reported that there were no co-payments made by women. In the event of complications, additional costs are incurred. Post-partum materials and transport costs are extra too. Where women have arrived expecting all services to be free, these additional costs cause problems and delays. At health post level, most KI reported that households only pay for items which are not included in the kits, if kits are available. If not available, then some charge for all costs, and others just waive the ticket costs and charge for all supplies. Costs of a normal delivery were reported to range from 750 FCFA to 11,000 FCFA. For complications, an additional 1,500 to 2,400 FCFA would have to be added. Of the 16 KI, only two reported no co-payments by women. Two reported that women pay full costs. In the case of women who deliver at home but come to the health post to register their baby and have a check-up, some reported that they have to pay for postnatal care and other not. When asked about the overall effectiveness of the policy, at national level, the mood was sceptical, with KI highlighting issues of poor understanding, uneven implementation, and dissatisfaction of key stakeholders, logistical problems, and stock-outs. Only the regional hospitals were thought to be getting a fair deal out of the policy. “Out in the field, one has the impression that the people involved have not understood or been sufficiently informed. It’s an exemption, but not everyone enjoys that benefit. Some are not entitled. Some preliminaries have not been completed. There are things left out during implementation. There should have been discussions in the regions to check on feasibility. The MCD are at the end of their tethers” (national KI) At regional level, the main concern was with continued charging. District KI were more positive, but still raised problems of stock-outs, lack of reimbursement, poor dissemination of information and the impact on facility finances in general. Sub-district KI also gave mixed responses, both positive, but expressing particular concerns about payments for community staff and about the need for a broader benefits package. “It’s a good policy, a relief for us, and we are satisfied because we are poor and no longer have to pay for deliveries and caesareans which were expensive. We would like the policy to become permanent and would ask for prescriptions to be paid for under the policy” (facility KI) Impact of policy Regional KI reported an increase in caesarean sections. The majority reported that facility deliveries had increased as a result of the policy. However, a few thought that there had not been much change and some stated that home deliveries are still significant, linked to traditional beliefs. At sub-district level, all believed that utilization had increased. One reported an increase of 50% between 2004 and 2005. Some reported fewer maternal and newborn deaths as a result. Most KI at district level thought that quality of care was unaffected. It was not reduced, but nor did the policy ensure it, given the shortages of kits and also of staff. Only one reported an improvement at health centre level, while at subdistrict, two reported an improvement (because of increased availability of basic supplies) and three no change. KI reported increased referrals from the Cases, due to reduced anxiety about ability to pay, but no clear change in referrals made from the health post level up. “There are more referrals thanks to the exemptions policy. Matrones no longer keep back in the Cases women who lack the means” (facility KI) District staff reported that systems had existed to deal with ‘social cases’ prior to the policy. These had relied on clients producing certificates or being brought in by the police or applying to the Comites de Santé for help. One KI estimated that about 10% of clients had been unable to pay. Most, however, could not estimate the proportion. Where eligible, these cases were given access to a special drug fund at the facility. Most sub-district KI reported that there was no change for the poor under the FDCP, as they had previously received free drugs, so there was no change. This suggests that both before and after, the poor were making some form of contribution. Only one reported that they had benefited as now the benefits went beyond free drugs. Estimates at health post level of the proportion of indigents ranged from 0% to 25%, with most estimating around 5%. In terms of financial impact, at national level, financial concerns were focused in the PNA, which was owed 124 million FCFA in November 2006 for kits sent out under the policy. At regional level, the main concern was about the short and medium-term impact on facilities. “The policy is a source of interruptions to feasibility in the health services. This is true of the health committees, who are heading for disaster. To resolve this problem the State should systematically ensure reimbursement of the subsidy” (Regional KI). All districts and sub-districts reported lost revenues (one reported losses in the region of 30-40% of total facility receipts, reflecting the importance of deliveries to the facility). They coped by increasing tariffs for other services, cross-subsidising from other sources, reducing investment, and soliciting more local government support. “There’s no change because we were able to offset the deficits by increases in tariffs” (District KI) While the workload increased with utilization, most KI at district and subdistrict level were unconcerned about the administrative burden imposed by the FDCP. They also reported that their staffing numbers had not changed. “There is practically no change in the workload. The ICP is always overworked. As for administration, there is no change” (Facility KI). All districts report the loss of revenues which were previously used to pay and motivate community staff (the matrones, who carry out most of the normal deliveries, the health promotion staff in the community, and some others, such as stretcher-bearers). This could pose a long-term threat to their retention, and led to calls from some for more state support for this group. The health posts are believed to be most affected. Subdistrict KI reported that community staff had been compensated out of general facility revenues. While most were paid a base allowance, plus a share of delivery fees before, now many receive an increased but fixed monthly allowance. Some reported a drop in income for community staff, some an increase, but most reported no change. “At the health centre level there is a distribution of the costs of community personnel, and so the policy can work well. However, at the level of the health posts there are problems” (District KI) Most district KI reported that the Cases had not been affected by the policy as they continued to serve women who were too distant to reach facilities. At sub-district level, the Cases were said not to be affected, but for contrasting reasons in different areas (either because they were still popular, or because they were no longer popular, or because they were not active). “In the Cases, deliveries are always to be paid for. This has not discouraged people due to their geographical accessibility” (district KI). District KI reported little activity by TBAs and private midwives, but subdistrict KI were more mixed: four out of ten reported that they continued to service remote areas; three reported that there were no TBAs in their zone; two reported that the TBAs had been affected negatively by the policy; and one that they were increasingly referring women to facilities. Overall assessment of policy The overall assessment by national KI was that the policy was important and positive, especially for poor women in rural areas, but that the implementation needed improving. “It is useful in reducing the financial barriers to access. On the other hand it has been poorly planned. There are weaknesses in planning, implementation and follow-up” (national KI). Regional KI felt that its main contribution was in increasing access to caesarean sections. At district level, responses were mixed: one welcomed the policy but was concerned about sustainability; one was positive but requested more kits and improved kits; one thought the policy inappropriate as many can pay for their care (except for caesareans, as these are an emergency); and the last felt that the initiative was mainly political. At the national level, the six stakeholders pointed to the following successes increases in utilization: reduced financial burdens for households; fewer deaths; providing reassurance to the population; showing political commitment to maternal health; helping to raise the profile of maternal health at the local level, thus mobilizing other resources; and increasing access to caesarean sections. At regional level, the following successes were noted by KI:
However, one KI sounded a sceptical note, saying that there had not been much change in his region (Fatick), due to difficult access and cultural perceptions. District KI echoed similar themes to those expressed at regional level, particularly in terms of increased utilization, reduced home deliveries and reduced deaths. However, one expressed concerns about the sustainability of the normal deliveries (more numerous than caesareans), and another noted the continuing high rate of home deliveries. The national KI highlighted the following problems with the policy:
The five regional KI were more reluctant to talk about failures, three of them pointing out that it were too early and that all support is positive. When asked about main constraints, Ministry KI highlighted an inadequate budget; communication issues right down the line, difficulties getting clear reports, difficulties verifying activity numbers; the fact that there is no budget line through which facility costs could be reimbursed; and poor dissemination and feedback from local levels. Donors highlighted lack of capacity at central level, in terms of staffing and skills, and also the need for a clearer definition of what ‘gratuité’ meant. At regional level, constraints included distance to accessing facilities. Another mentioned the issue of verifying residency. A third KI highlighted the difference between the rhetoric of free services and the reality of limited support for those services, and the need for clearer communication. Fatick has specific problems linked to the fact that it lacks an operating block and has to refer to neighboring regions. Constraints noted at district level included general overload of work; difficulties providing for community staff and free drugs; increase in work specifically related to the policy, shortfalls in supply of kits, cultural barriers, and lack of functional EmOC facilities and personnel. The national level KI were all sceptical, in varying degrees, about sustainability. The Ministry of Finance KI pointed out the uncertainties facing state coffers over the years ahead and suggested instead a focus on microinsurance and community health insurance. Donors emphasized the need for government leadership and political commitment. Ministries KI were uncertain about the policy’s future. One saw it as worthy but possibly lacking support outside the Ministry. The other two saw the design as inherently unsustainable. “I do not know. There is awareness in the MSPM. Is it backed by other ministries (above all finance), because resources must follow?” (national KI) “Taken as such – no! Financing supply and demand is something that cannot last. One must think in terms of a global financial strategy for demand” (national KI) The regional KI were united in their desire for the policy to be sustainable, but with varying degrees of optimism about that likelihood. Two insisted that it must be sustained; two thought it was possible, with certain measures; and one thought it unlikely. Regional KI felt that the state should support the policy financially, but two KI also suggested more popular contributions, and one more support from regional authorities. One reported that hospitals had been asked to seek funds to support the policy. When asked about who had benefited from the policy, the national level KI felt that all women and their households had benefited from the fact that they did not need to pay for deliveries. One also mentioned the hospitals, which receive funding for caesareans and also free kits from the PNA (via the regional medical directors). One mentioned rural women in particular. One thought that politicians were the main beneficiaries. The eight regional KI showed very similar views. District KI were more concrete about the beneficiary group, pointing out that only those women who deliver in health facilities benefit, while women with home deliveries are even penalized (3,000 FCFA in one example). One KI disagreed and said that in his area women who delivered at home also benefited from free care. Another pointed out that while intra-partum care is covered; early complications such as pre-eclampsia or post-partum complications such as haemorrhages were not covered by the kits. When questioned about who had lost out as a result of the policy, the most common response at national level was that the Comites de Santé had lost out, from revenues foregone and not adequately compensated. One person mentioned the community staff. One mentioned the women who had gone to deliver in facilities where kits were lacking. One person mentioned the PNA, which was being asked to upfront kits without payment. One mentioned the Ministry, which was ‘swallowing up’ a lot of money. One person thought that women and the whole health system were the losers, and one person went even wider and thought that the state had lost credibility as a result of the policy. The three regional KI mentioned different groups who had lost out. One mentioned the villages which could not reach services. One mentioned the health facilities and also the better off households (in Ziguinchor, some form of means testing is being applied for caesareans). A third mentioned the hospitals but also private clinics which were getting less business in terms of caesareans. At district level, one KI felt that there had been no losers, while the other felt that those with complicated deliveries other than a caesarean had lost out, as their cases were not covered by the kits. Despite these problems, most national and regional KI reported that the policy should receive high priority, because of the potential to save lives of a vulnerable and critical group (mothers and babies), because of lack of protection against health care costs, and because it helped health staff to do their jobs more effectively. Most district KI gave unconditional priority to the policy, saying that it relieved suffering, reduced delays, increased facility deliveries, led to a change of mentality in relation to home births, and addressed the low decision-making power of women in relation to paying for deliveries. However, two pointed out that in order for it to work, the kits had to be augmented to include the materials to deal with complications. Sub-district KI were more sceptical, with broadly half negative, and half positive or conditionally positive. The sceptics felt that health care should have a cost and that it was more important to improve quality and staffing than reduce costs. Recommendations KI were asked for their recommendations for the policy. In terms of the overall design, only one recommended abolition. Other major modifications included targeting the policy to the poor; encouraging more contributions from communities; generating more support from the Mutuelles de Santé and donors; focusing on caesareans only; and increasing state support to the facilities to allow them to lower user payments. There were also a number of recommendations related to the financing of the policy, including the need for longer term financing, expanded funding and funding according to real needs. There was also much demand, especially from districts, to reimburse facilities for their losses under this policy. In terms of implementation, national level KI had a number of recommendations, calling for improved dialogue and communication between stakeholders; a more efficient reimbursement system; effective verification of facility claims; a thorough plan for implementation; improved leadership; proper feasibility studies; more sensitization of all actors; and involvement of local leaders. The subdistrict KI focused also on the need for incentives to motivate staff. There were also detailed recommendations in terms of additional items to be included in the caesarean and delivery kits, along with the request for kits to cover complicated deliveries and more materials for the care of the newborn. District and sub-district KI also requested an increased overall supply to avoid stock-outs. In addition to recommendations relating directly to the policy, a number of KI focused on complementary actions, which are necessary to make the policy effective. These included: more trained staff; more midwives; training all nurse in-charges in basic emergency obstetric care; extending the network of facilities; making sure that all operation blocks are functional; improving the quality of services and the reception of patients; improving the working conditions of staff; and improving roads and transport for referrals. Discussion The key informant interviews provide a rich seam of insights into the application of the FDCP in Senegal. There is a high degree of commitment to the goals of the policy and the importance of the problem that it is tackling. Facility data from the five regions also suggests that the policy has had a positive impact, with an increase in coverage of facility deliveries from 40% to 44% over 2004-5 (which is highly significant – p<0.0001), and an increase in caesarean section rates from 4.2% in 2004 to 5.6% in 2005 (which is highly significant – p<0.0001)13. At the same time, it is clear that many practical problems remain to be solved. Even at the highest levels, there is a lack of ownership of the policy and process, and the recommendations relating to implementation from the national level key informants imply going back to basics. A number of them – such as the setting up of a steering committee, taking technical advice, consulting stakeholders – overlap with what the key informants themselves told us had already been undertaken. At the same time, there is evidence on the ground of contradictory policies being pursued in delivery services. Some of the findings are unexpected. That there is no clear overall document laying out the policy may in part explain some of the ambiguities at lower levels about what the policy means and how it is to be implemented. Dissemination has been largely oral, even for health staff. Communication is not assisted by the fact that there are different rules for different facility types. However, more fundamentally, many KI commented that the concept of ‘free’ services was in itself confusing. The benefits being offered and the items which are not covered have to be spelled out extremely clearly, both for providers and clients. The absence of clear guidelines has not helped this process. One of the fundamental issues emerging for providers is the inadequacy of kits to compensate them for the full loss of earnings at district and health post levels. This relates to the absence of funding channels, which should have been foreseen. This, along with other findings, suggests that the policy was rushed in without adequate preparation, though the reasons for this are not clear. Delays and inadequacies in numbers of kits from the start gave a poor impression of the policy from the beginning. The providers have since been faced with another exemption policy – ‘le Plan Sesame’ -for the over-60s. It was launched in 2006. As this policy also involves retrospective reimbursement of services, it is adding to the burden faced by the Comites de Santé. Facilities report losing 30-40% of their receipts in some cases, although the financial analysis suggests that their overall revenues are holding up 13 . However, all the coping strategies that they adopt have costs (e.g. for other patients, if tariffs for other services are increased). Concern for the community staff comes out clearly from these interviews. Their situation is precarious, as they perform many of the key functions of the lower facilities, but are not on payroll. It appears that they have not suffered much either in terms of pay or numbers – that is confirmed by the financial analysis too – but that this is thanks to increased funding from the general facility revenues. The use of kits as a support mechanism is in itself challenging, as it requires transport costs, proper storage and management, and is inflexible (making it hard to provide for different needs in each case). Although the KI did not discuss kit management, the financial analysis component found inadequacies in this area (no registers were given, for example). The addition of kits for complicated deliveries, promised in 2006, will add to the logistical problems of proper planning and distribution. Another theme to emerge from the interviews is the mismatch between demand for and supply of kits at district and sub-district level. While higher KI report a system based on estimated deliveries, this is not reflected in the experience on the ground, and the financial analysis supports the view that kits were not allocated according to population-based indicators in practice. Irregularity and unpredictability are disastrous characteristics for a policy of this kind, leading to lack of confidence and compliance by providers and clients. Some areas appear to have been particularly disadvantaged (e.g. Ziguinchor, which received no funding for caesareans in 2006). The use of caesarean kits for CS II is a debatable design decision. While regional hospitals are being reimbursed at above-cost level in ‘real money’13 , the few health centres which are functioning as surgical blocks in the FDCP regions will lose significant revenue per caesarean, given the labour and general costs which are not reflected in the content of the kits. An evaluation of a similar exemption scheme in Ghana found that inadequate funding at the national level was a key constraint in implementation14 . It is interesting that so far this does not appear to be the case in Senegal, despite the fact that the policy has no external support. The decision to roll-out to all regional hospitals in 2006 was, according to KI, motivated by budget under-spend. This however is a very short-term approach to decision-making, and as the policy expands, the funding constraint may become more of an issue. Moreover, if overall resources were not constrained, it is not clear why there was an outstanding debt to the PNA of 124 million FCFA in November 2006, unless this was part of a dispute about the operation of the policy. One of the themes which emerges strongly from the lower level KI is the reality of geographical exclusion – women living in remote villages have very little chance of benefiting from this policy as they do not use the facilities where it is being applied. These and cultural barriers are explored more in the focus group discussion and in-depth interviews15 . They contribute to what some of the KI acknowledge is a continuing high level of home deliveries and deliveries in the Cases de Santé. For normal deliveries, even for households living within reach of health posts or health centres, it is not clear how significant the benefits of the policy have been, given the number of cost items which KI listed as being excluded. The interviews provide important information on ongoing costs to clients, even when the policy is functioning and kits are available. When they are not, the clients at worst have been paying full costs, at best being exempted a ticket cost worth 1,000-2,000 FCFA ($2-$4). In some areas the policy is reported as having been suspended. In others, there were stock-outs lasting months. Given the real costs of arriving at and using formal health services, it is important to reevaluate whether the degree of subsidy to households is likely to be sufficient to motivate behavior change, especially for normal deliveries. For caesareans, the policy is functioning better, as funds to regional hospitals are flowing albeit with significant delays and the support to households is likely to be more significant (though in the absence of an exit interview, it is hard to be certain how much households are now paying for caesareans). It is clear however that the caesareans have to be more closely monitored, to counteract fraud and inappropriate use. At the community level, attitudes towards caesareans are reporting to be shifting, and the policy may be contributing to that increased awareness and acceptability. We have to conclude however that financial barriers and lack of certainty still exist under the policy. Households are paying around 3,000 FCFA at health centre level for normal deliveries, without complications, when kits are there. To that must be added the cost of postnatal care items, transport, plus potential complications, plus possibly all costs when kits run out. At health post level, they are reported to be paying between 750 and 11,000 FCFA for normal deliveries, with an additional 1,500 to 2,400 FCFA if complications arise. Some are even reported to be paying full costs. If, in addition, they arrive with the expectation that all items will be free, then the efforts needed to belatedly seek funds will add to delays in treatment and erode confidence. For caesareans, information is lacking on how much households are continuing to pay, but it is likely to include costs of some significance, such as transport, hospitalization and food costs. Although systems existed before and continue to exist at facility level for the ‘cas sociaux’ (those unable to pay), the vagueness of KI on the proportions who were eligible for this support suggests that the system is informal and that most have paid something. It appears that free drugs are the most that can be offered. In terms of the quality of care, it appears from the KI that quality has not been affected – but then, nor has it been guaranteed. This is similar to the findings in Ghana, where quality of care was found to be poor both before and after the delivery fee exemption policy was introduced16 . Moreover, in Senegal most delivery care in health posts is provided by matrones, who have only basic training, so the value-added of bringing women into these facilities needs careful consideration. The main advantage is the availability of the ICP, in theory, to handle complications as they arise. A policy such as the FDCP has to fit within a national health financing policy which is based on the consensus of the major players. There is some evidence from the KI that such a consensus is missing. How realistic is it for government to subsidise certain services? Are the mechanisms there to do it effectively? Are community financing options preferable, and if so, for which services? These questions and others are raised by the comments of the KI. Alternative support mechanisms, such as increased central funding in exchange for reduced charges to certain patient categories, need careful consideration. Conclusions The KI interviews have provided detailed information on how the Free Delivery and Caesarean Policy has been implemented in its first two years and how it is perceived by key stakeholders at different levels. The findings suggest a high degree of commitment to its goals and relevance, but also a number of major implementation issues. The evaluation findings emphasized the importance of a number of measures, including establishing a consensus on health financing strategy at the national level (reconciling access with sustainability, particularly for lower level facilities); careful planning and communication of the policy on exemptions; the establishment of strong and transparent systems for allocating resources and accounting for them; and the articulation of an unambiguous entitlement package for communities which is adequately reimbursed for providers. Geographical and cultural barriers are even more intractable than financial ones, in many contexts, and long term investment in supply will also be needed to increase access for the most remote areas. Acknowledgements The evaluation in Senegal was carried out in partnership between the Ministry of Preventive Health and Medicine (MSPM), UNFPA, Immpact and CEFOREP, with funding of local fieldwork coming from UNFPA. Immpact is funded by the Bill and Melinda Gates Foundation, the Department for International Development, the European Commission and USAID. We would like to acknowledge the support of all key informants, particularly within the Ministry, and the work of the whole research team, including Thiam Touré Tarr, Amadou Hassan Sylla, Thierno Dieng, Professor Vincent de Brouwere, Isabelle Moreira, Dr Anna Coates, Fatoumata Bintou Drame Mbengue, Daouda Mbengue, Dr Marguerite Ferreira Crato Cisse, and Binta Mbaye. 1 Matrones are assistants to midwives, recruited through the community and given 3-6 months’ training in normal deliveries. They usually work at the periphery in health posts or Cases de Santé but can also work in district or regional hospitals as auxiliary midwives References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08040t1.jpg] |
| |||||||||

{kind=link}