 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
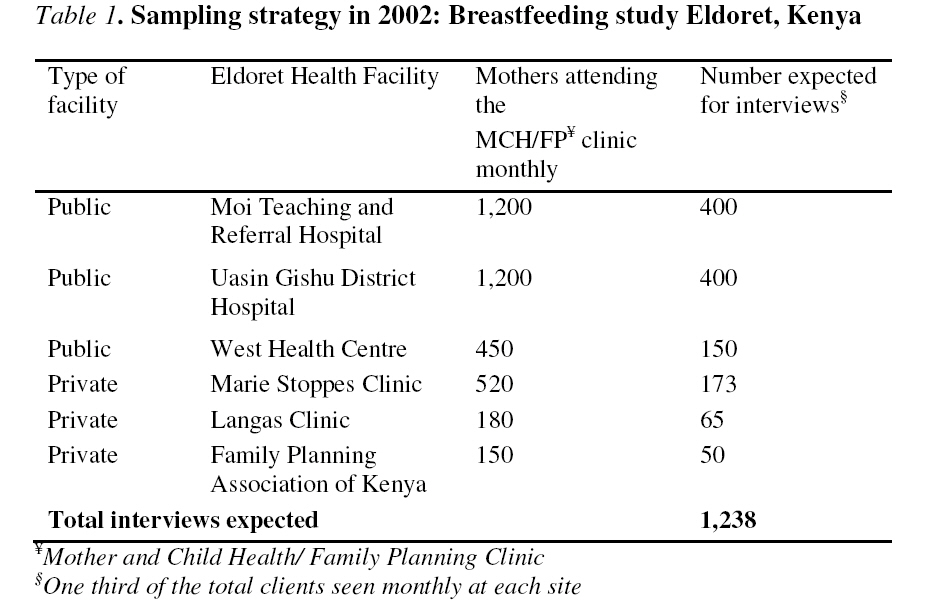
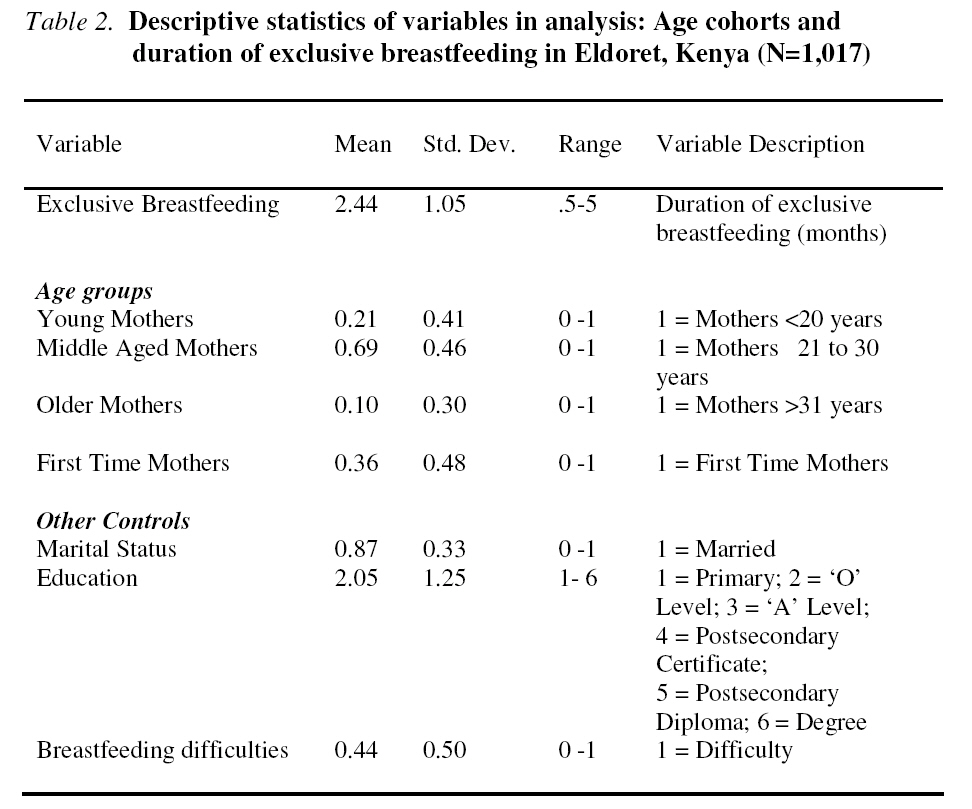
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 125-138 Original Research ArticleYoung Mothers, First Time Parenthood and Exclusive Breastfeeding in Kenya Violet Naanyu Correspondence: Department of Sociology, Indiana University, BH 744 1020E. Kirkwood Avenue Bloomington, IN 47405-7103. Tel:1-812-606 6081 Fax: 1-812-855-0781 Email: vyebei@indiana.edu Code Number: rh08042 ABSTRACT Breastfeeding behaviour is explored in Kenya using data collected in the town of Eldoret, Kenya. This paper specifically examines duration of exclusive breastfeeding among young mothers below 20 years of age as compared to older cohorts. Additionally, focus is laid on the effect of first time motherhood and breastfeeding difficulties on exclusive breastfeeding. Results show that Eldoret mothers are aware of benefits of breastfeeding; nevertheless, the mean duration for exclusive breastfeeding in this sample is 2.4 months. Higher durations of exclusive breastfeeding are associated with increasing age and first time motherhood. Predictably, breastfeeding difficulties bear a negative association with exclusive breastfeeding. While HIV is transmissible through breastfeeding, breast milk remains a vital source of nourishment for infants in Sub-Saharan Africa. More research on mothering should examine the changing socio-economic milieu and its influence on women’s infant feeding decisions RĖSUMĖ Jeunes mères, maternité débutante et allaitement exclusif au Kenya Le comportement d’allaitement est employé au Kenya en se servant de données assemblées dans la ville d’Eldoret, Kenya. Cette communication examine spécifiquement la durée d’allaitement exclusif parmi les jeunes mères au-dessous de 20 ans par rapport aux plus âgées. En outre, on a mis le point sur l’effet de la maternité débutante et les difficultés d’allaitement exclusif. Les résultats montrent que les mères à Eldoret ont conscience des bénéfices d’allaitement ; néanmoins, la durée moyenne pour l’allaitement exclusif dans cet échantillon est 24 mois. Les durées plus élevées d’allaitement exclusif sont associées avec l’augmentation de l’âge et la maternité débutante. D’une manière prévisible, les difficultés d’allaitement exercent une association négative sur l’allaitement exclusif. Bien que le VIH soit transmissible par l’allaitement, le lait maternel reste une source vitale nourrissante pour des petits enfants en Afrique subsaharienne. Plus de recherche sur la maternité doit examiner le milieu socioéconomique en mutation et son influence sur les décisions des femmes de l’allaitement infantile (Afr J Reprod Health 2008; 12[3]:125-138). KEY WORDS: Exclusive breastfeeding, Young mothers, First time parenthood, Breastfeeding difficulties, Kenya Background Breastfeeding recommendations stress the importance of six months of exclusive breastfeeding. This means that an infant relies on breast milk without any additional fluids or food1. Breast milk is convenient, hygienic, and has high concentration of growth and immunity factors. It decreases the incidence of many illnesses in childhood and thereafter in adulthood, and also confers benefits on the mothers’ health1. Additionally, through the physical breastfeeding relationship, mothers and infants find enhanced bonding and attachment2. Exclusive breastfeeding has been defined as giving the infant breast milk only, except for drops/syrups containing vitamins and minerals3. Although exclusive breastfeeding is recommended for the first six months of life4, early introduction of supplementary fluids is common globally5, 6 . Mothers in developing countries engage in mixed feeding for a number of reasons 7, 8,9,10 . In Nigeria, none of the infants are exclusively breastfed; they are given alternative feeds like water, formula, or herbal tea7. In a Malawi study, only 19% of infants in a cohort of 720 got exclusive breastfeeding in their first year of life8. Complementary foods are usually introduced early due to perceived lactation insufficiency7, 9. Exclusive breastfeeding is considered ‘risky’ hence supplementary water herbal infusions are believed to enhance growth, quench the infant’s thirst, and serve as food and medicine9. Another reason for mixed feeding is a mother’s perception of breastfeeding as ‘physically draining’ especially where lactating mothers find limited access to nutritious and adequate amounts of food for themselves7. Some Indian communities believe infants need additional fluids to maintain body-water balance10 while in Honduras, solid foods are introduced early in order to extend the time between feeds and also because mothers find breastfeeding to be time demanding. They also believe that infants have to learn how to differentiate food flavours, eat and digest other foods11. The foregoing examples show that exclusive breastfeeding decisions are influenced by cultural beliefs as well as role conflict on the part of mothers. Of interest to this paper is a mother’s age and first time parenthood. Cohort variation in breastfeeding duration is investigated since some argue that young women are immature and psychologically ill-prepared for parenthood12. Others emphasize that, understanding social change is important because there are enduring cohort differences owing to historical influences on cohort development13, 14. Over the years, Kenyan women have experienced great micro and macro socio-economic changes. For instance, younger cohorts access more education resulting in higher possibilities for formal employment and self reliance. Indeed past studies indicate that there is aggregate increase in education in Kenya over time15. Another age related variable of interest to this study is transition to parenthood. First time motherhood especially for young women below twenty years of age is a major milestone in life. For best results, this transition requires adaptation and support from close social networks16, 17 . First time parenthood is therefore understood as a key stage (entering the parent role) in a woman’s life that may have enduring effects on her social experiences and breastfeeding decisions. This paper specifically investigates duration of exclusive breastfeeding among young mothers during the first five months after birth. It also examines whether exclusive breastfeeding varies with first time motherhood, marital status, education, and breastfeeding difficulties. Methods Study Site, Design and Sample This study was conducted in 2002 in Eldoret, an urban centre in western Kenya. It included face to face semi structured interviews and focus group discussions with women in Eldoret town. All study activities were approved by the local institutional review board, government administrators, and workplace administrators (where focus groups were held). Participants were assured of confidentiality and objectives of the study were clearly explained to them prior to interviewing and group discussion. Interviews took place in selected health facility waiting bays. Two research assistants were trained to conduct interviews. The study began with a pilot test of the interview tool involving 30 women from three Mother and Child Health and Family Planning (MCH/FP) clinics in Eldoret. The pilot study led to an improved version of the tool and development of appropriate sampling strategies. Six Mother and Child Health and Family Planning clinics in Eldoret were randomly selected from the facilities with the highest turnover of clients. In order to reach mothers with diverse demographics, three of the selected facilities were from the private sector while another three were public facilities. As shown in Table 1, the number of respondents invited for interviewing corresponded to a third of the total number of clients seen monthly at each of the selected facilities. Random stratified sampling was used to select participants for the purpose they served the study. The selection criterion employed included employed and self employed mothers with infants aged < 24 months old, and mothers residing in Eldoret town. In total, 1,121 mothers were successfully interviewed (Table 1). Focus group discussions were convened with the intention to discuss mothers’ knowledge of breast feeding advantages, their social roles and breastfeeding experiences, and general infant feeding practices. Invitations to key workplace administrators were issued by the researcher with a general description of the discussion topic. In turn, invitations were extended to workers who fulfilled the study criteria: mothers with children below two years of age. Meetings were convened during lunch break and commenced once a majority of expected participants had arrived. They were held in offices or meeting rooms at different work places. Participants were seated on chairs in a semi-circle facing the facilitator and reporter. Communication was in English and Swahili and the meetings lasted one hour. Refreshments were served because the meetings occurred during lunch break. The researcher facilitated all sessions and followed a structured discussion guide to introduce the major segments of the discussion, but topics were allowed to deviate as participants shared diverse breastfeeding experiences. A total of 35 women were involved in six focus group discussions. Three groups consisted of women from the private sector (bankers, a Catholic-run facility, and teachers from a private school) while another three groups included those from the public sector (teachers from a public high school, employees of a public university, and employees of a public hospital). All discussions were audio-recorded and recordings were subsequently transcribed. Data management involved thematic analysis of transcripts to classify content segments into coherent categories. This paper focuses on quantitative variables addressing the effect of age, first time motherhood and breastfeeding difficulties on the duration of exclusive breastfeeding. In addition, relevant focus group discussion findings are used to bolster quantitative findings and discussion. Measures and Analysis Table 2 shows how study variables are coded for analysis: duration of exclusive breastfeeding (in months); age groups as young (<20 years), middle aged (20 to 30 years) and older mothers(>30 years); marital status (married=1, others=0); education level (1=primary, 2=‘O’ level, 3=‘A ’level, 4=postsecondary certificate, 5=postsecondary diploma, 6=degree); motherhood (first time mothers=1, others=0); and experiences of breastfeeding difficulties (breastfeeding difficulties=1, none=0). After selection of variables of interest from the quantitative data, all cases with missing values were dropped from the analysis resulting in a total of 1,017 cases. Descriptive statistics are used to present univariate and bivariate findings. Further analysis involves use of three regression models. Duration of exclusive breastfeeding is examined and expected to differ with different age groups. As shown in Table 5, the variables are used in the models as follows: duration of exclusive breastfeeding (in months); age, (youngest mothers as the reference category); marital status (married mothers versus others); education (level of schooling); motherhood (first time mothers versus others); and difficulties (mothers with breastfeeding difficulties versus others). The base Model has duration of exclusive breastfeeding regressed on age groups. In Model 2 demographic variables are introduced including marital status and education. In Model 3, first time motherhood and breastfeeding difficulties are added to the model. Results Descriptive statistics in Table 2 show that, young mothers (below 20 years of age) comprise 21% (N=216) of the total 1,017 cases in analysis. More than half are middle aged (69%), married (87%) and on average have some secondary level education. First time mothers comprise 36% (N=362) of the sample, and at least 44% (450) of all mothers report that they experienced breastfeeding difficulties (Table 2). Eldoret mothers (Table 3) are aware of key advantages and disadvantages of breast milk. Nonetheless, the mean duration of exclusive breastfeeding in the survey sample is 2.4 (SD = 1.05) months (see Table 2). Among those who have introduced supplementary feeds, some popular foods noted in the survey include; cow milk (60%), porridge (76.8%), potatoes (12.4%), fruits (5.2%), Cerelac -a highly nutritious, easily digested instant cereal (4.2%), and formula milk (2.4%). In Table 4, mothers participating in the focus group discussions explain why these foods are popular. They also add pumpkin leaves to the list of infant feeds (Table 4). About 72% (N=156) of young mothers are married and they comprise 42% (N=153) of first time mothers in this sample. Concerning difficulties, 47%% (N=102) of young mothers report experiencing breastfeeding difficulties. Starting with the most prominent, the following breastfeeding problems are mentioned by mothers: delayed milk production, insufficient milk supply, engorged breasts, post caesarean recovery, sore or cracked nipples, and small or flat nipples. During focus group discussions, mothers shared personal experiences with regard to specific problems including: having a ‘boil’ on the breast, painful initiation of breastfeeding, painful contracting uterus, cracked and small nipples, leaking breasts, engorged breasts, ‘disappearing milk’ after a mother’s illness, and difficulties attaching the nipple properly for the feed. The regression models show that the duration of exclusive breastfeeding increases with age (Table 5). Estimates for middle aged and older mothers are higher as compared to younger mothers in all models, all else equal. In Model 1, exclusive breastfeeding among mothers between 21-30 years of age increases by a factor of .29 (t=3.56, p ≤.001) all else equal. This estimates drops slightly to .27 (t=3.08, p ≤.01) when marital status and education variables are added to the model. However, in the last model, the estimate goes up again to .36 (t=4.02, p ≤.001) when first time motherhood and breastfeeding difficulties are taken into consideration (Table 5). Table 3. Eldoret mothers’ opinions on advantages and disadvantages of exclusive breastfeeding (Focus group discussions, N=35)
Being an older mother (31 years and above) is also associated with higher duration of exclusive breastfeeding. Results in Model 1 show that exclusive breastfeeding among the oldest cohort increases by a factor of .28 (t=2.26, p ≤.05) all else equal. This estimates drops slightly to .24 (t=1.85, p ≤.10) in Model 2. In Model 3, we observe the highest positive association between age and exclusive breastfeeding; compared to young mothers, the oldest cohort bears an estimate of .41 (t=2.91, p ≤.01) all else equal. First time mothers are breastfeeding longer than all other mothers (p ≤.001) and as would be expected, breastfeeding difficulties have a negative association with exclusive breastfeeding by a factor of -.18 (t=-2.81, p ≤.01) all else equal. Discussion Age Cohorts and Exclusive Breastfeeding Past studies suggest that duration of breastfeeding is generally associated with demographics18. As McKinley and Hyde argue19 , education, income, and age may represent differences in attitudes as well as access to different structural supports. Similarly, it is apparent in this study that duration of exclusive breastfeeding Table 4. Alternative feeds used by Eldoret mothers and reasons why they are preferred (Focus group discussions, N=35)
increases with age. This finding is consistent with the expectation that older married women would have a longer duration of exclusive breastfeeding due to a number of possible propositions. First, with increasing education, socio-economic change is inevitable, thereby instigating inter-cohort variation20. Increasingly, younger Kenyan cohorts have access to more educational opportunities resulting in higher possibilities for work outside the home. In Witwer’s21 analysis on the mean duration of breastfeeding in Africa, he notes that women with seven or more years of education report shorter Table 5. Exclusive breastfeeding regressed on demographics, first time motherhood and breastfeeding difficulties in Eldoret, Kenya (N=1,017)
Standard errors in parentheses durations of breastfeeding than those with none. Like other African women, Kenyan women are increasingly joining the labour force and experiencing changing gender relations15. Secondly, the finding that older women have longer durations of exclusive breastfeeding may be due to differences in life experiences and advancement in the life cycle. Middle aged and older women may be at liberty to exclusively breastfeed for longer breastfeeding techniques. Cross tabulation of first time mothers and education (not shown in tables) reveals that first time mothers have a secondarylevel education similar to that of middle aged mothers (mean = 2.1 ) who happen to be breastfeeding longest in all models. This postulation is supported by earlier studies that show a positive correlation between increasing education and longer durations of exclusive breastfeeding23. Most (75%) of the first time mothers are married. This implies that spousal supply of household needs during the first months may increase the duration of exclusive breastfeeding as was observed in other studies22. Lastly, first time mothers may feel obliged to conform to breastfeeding norms more than older women who may already be established in other social statuses besides motherhood. Since 42% of first time mothers are in the young cohort, their entry into the parenting role may be characterized by ‘socially ideal’ mothering activities. For example, in Mali, very few women use breast milk substitutes, in fact, young women seldom can be said to “choose” whether or not to breastfeed. Instead, they grow up surrounded by older women nursing babies and are expect to be successful at nursing their own children24. Hence, the desire to conform to social norms may influence first time mothers’ breastfeeding decisions. This need to conform to prevalent social norms was also an animated part of the focus group discussions in this study (see Table 4) as mothers stress that they give infants alternative foods that are “traditionally considered best for infants” and what “mothers are advised to feed infants.” Predictably, breastfeeding difficulties have a negative association with exclusive breastfeeding for all mothers. These findings may be attributed to inadequate prenatal and postnatal breastfeeding education. This association is supported by a study which found that inadequate breastfeeding information is given to mothers in the same town of Eldoret25. This study has several limitations that require caution in making generalizations. It was limited to selected health clinics in one Kenyan town. Findings are therefore viewed as indicative of general breastfeeding patterns rather than population estimates. Notwithstanding the foregoing limitations, this study adds to a much needed literature on breastfeeding patterns in Sub-Saharan Africa. Implications and Conclusions Study findings show that Eldoret mothers are not achieving the recommended six months of exclusive breastfeeding because the mean duration for exclusive breastfeeding in this sample is 2.4 months. This implies that Eldoret mothers are giving infants alternative feeds at an early age. Early alternative feeding has been associated with poignant disadvantages; infants may be in danger of infirmity, over-diluted milk feeds, and inadequately prepared or poorly stored foods26, 27, 28. For instance, in Nigeria, alternative feeds have resulted into higher incidences of infant diarrhoea27. In another study from Guinea-Bissau, the incidence of diarrhoea was higher in weaned children than in partially breastfed children, and children aged 12-35 months who were not breast fed had a 3.5 times higher mortality than breast fed children. Termination or reduced breastfeeding may signify that infants do not get all the valuable nutrients required for proper growth. Indeed, earlier studies in Africa reveal that easily available weaning foods have high carbohydrate content and intake of vitamins and animal products is irregular29, 30 . Given the high cost of commercial weaning foods, lack of sufficient knowledge in preparing well balanced diet from the limited available foods can lead to malnutrition31. This study suggests that duration of exclusive breastfeeding increases with age; younger mothers (below 20 years) have shorter durations of exclusive breastfeeding when compared to older cohorts. There are many plausible explanations for this trend such as an increase education among Kenyan girls (hence an increase in employment outside the home) and a lack of parenting skills. Another key finding is that higher durations of exclusive breastfeeding are associated with first time parenthood. Since breastfeeding in common in Kenya, new mothers’ entry into the parenting role may be characterized by a desire to conform to the prevailing social norms on infant feeding. Mothers may also have limited alternative feeding options because nutritious infant feeds are costly31 . The role of the health care providers cannot be overemphasized. As a study in Nairobi Kenya showed, the tradition of separating mother and child in hospital wards, breastfeeding on a rigid schedule and introducing pre-lacteal feeds reduces prevalence of breastfeeding32. Management of the newborn baby and the mother in the maternity ward and on arrival at home should not interfere with breastfeeding. Some of the issues health workers should discuss with mothers include the advantages of breastfeeding, size and nature of breasts, suckling after delivery, and emotions that come after delivery26. This study also highlights breastfeeding difficulties that are associated with lower durations of exclusive breastfeeding. This further emphasizes the need for more breastfeeding education during and after pregnancy. The media, health workers, and older experienced mothers can all provide the necessary information and emotional support required. Notwithstanding the fact that HIV is transmissible through breastfeeding33 breast milk is nourishment for infants in resource-poor Sub-Saharan Africa. A mother’s HIV infection should not be an automatic hindrance to breast feeding especially in contexts where quality alternative feeds are scarce. For example, in a South African study, infants exclusively breastfed for three months or more had no excess risk of HIV infection than those who were never breast fed, and exclusive breastfeeding was associated with reduced risk of HIV transmission when contrasted to mixed feeding34. Thus, irrespective of the HIV pandemic in Sub-Saharan Africa, breastfeeding remains a vital source of infant nutrition -though clearly, caution is required. Given the value of exclusive breastfeeding, more large scale studies should examine current breastfeeding patterns in resource constrained countries. Moreover, more research should focus on improving our understanding of women’s breastfeeding decisions and related experiences. Future research can also investigate how young mothers from different social groups balance demands of young adulthood and mothering. Acknowledgement I am indebted to the busy mothers who shared their experiences, and the dedicated research assistants for their commitment to the study. References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08042t2.jpg] [rh08042t4.jpg] [rh08042t5.jpg] [rh08042t1.jpg] [rh08042t3.jpg] |
| |||||||||

{kind=link}
{kind=link}