 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 159-172 Original Research Article An Assessment of the Readiness for Introduction of the HPV Vaccine in Uganda Katahoire RA1, Jitta J1, Kivumbi G1, Murokora D1, Arube Wani J1, Siu G, Arinaitwe L1, Bingham A2, Mugisha E3, Tsu Vand2 *LaMontagne DS2 1Child Health and Development Centre, Makerere University Medical School, P.O. Box 6717,
Kampala, Uganda, Code Number: rh08045 ABSTRACT Formative research assessing human papillomavirus (HPV) vaccine readiness in Uganda was conducted in 2007. The objective was to generate evidence for government decision-making and operational planning for HPV vaccine introduction. Qualitative research methods with children, parents, teachers, community leaders, health workers, technical experts and political leaders were used to capture understanding of socio-cultural, health system and policy environments. We found low levels of knowledge about cervical cancer and HPV. Vaccination and its benefits were well-understood; respondents were positive about HPV vaccination. Health systems were deemed adequate for HPV vaccine delivery. Schools were identified as a vaccination venue, given high attendance by girls aged 10-12 years. Communication and advocacy strategies to foster acceptance should provide information on cervical cancer, HPV vaccine safety, and side effects. Policymakers requested further detail on costs. Introduction of HPV vaccine could be integrated into existing reproductive health and immunization policies. RĖSUMĖ Une évaluation de l’empressement pour l’introduction du vaccin PVH en Ouganda Une étude formatrice pour l’évaluation de l’empressement du vaccin papillomavirus humain (PVH) en Ouganda a été menée en 2007. L’objectif a été de généré la preuve pour la prise de décision par le gouvernement et la planification opérationnelle pour l’introduction du vaccin PVH. Les méthodes de recherche qualificative avec les enfants, les parents, les enseignants, les leaders des communautés, les dispensateurs, les experts techniques et les leaders politiciens se sont servis pour attirer la compréhension socioculturelle, du système sanitaire et la politique des environnements. Nous avons découvert des niveaux bas du cancer du col et la vaccination de PVH. La vaccination et ses bénéfices sont considérées adéquats pour la livraison du vaccin PVH. Les écoles ont été identifiées comme centre de vaccination étant donnée la fréquentation élevée des filles âgées de10-12 ans. La communication et les stratégies de plaidoyer en cause d’encourager l’acceptation doit fournir des informations sur le cancer du col, la sûreté du vaccin PVH et ses conséquences. Les décideurs de politique ont demandé pour plus de détails sur les prix. L’introduction du vaccin PVH pourrait être intégrée dans les politiques de la santé de reproduction et d’immunisation. KEY WORDS: Human papillomavirus, vaccine, formative research, cervical cancer, Uganda Introduction Cervical cancer is the second most common cancer among women worldwide. If not detected and treated early, cervical cancer is fatal. In many regions, this is the most common cancer among women1. In Uganda, the agestandardized incidence rate (ASR) is 40.7 per 100,000 women. Trend data show that the ASR has doubled over the years from 19.7 in the 1960’s to 40.7 per 100,000 in 1994–19972.Cervical cancer survival studies show very low five-year survival rates for women in Uganda,3,4 due to delayed presentation at health facilities when the disease is in an advanced stage and radiotherapy is a less effective treatment5. Poor access to screening and treatment services, especially in low-resource settings like Uganda, makes the advent of prophylactic human papillomavirus (HPV) vaccines an attractive new opportunity to reduce the global impact of cervical cancer. As one of four countries involved in the HPV Vaccines: Evidence for Impact project implemented by PATH6,Uganda was the site of a 2007 formative research study assessing readiness for introduction of the HPV vaccine. The main objective of this project is to generate data for answering critical questions that would contribute to government decisionmaking and operational planning related to HPV vaccine introduction. Formative research seeks to gather information on a target audience’s beliefs, attitudes, knowledge, previous experience with, and behaviors related to a health problem of interest, as well as the context that influences, and is influenced by, these individual-level factors.7,8 Our formative research study comprised three interrelated components: (1) the socio-cultural milieu—the social and cultural context of health and well-being that may influence support for vaccination; (2) the health system’s capacity—those institutional factors affecting vaccine delivery; and (3) the policy environment—structures and processes required for policy formulation for HPV vaccine introduction. This paper presents key findings from each study component and discusses the implications of these results in designing effective strategies for HPV vaccine delivery, communications, and advocacy in the Ugandan context. Methods The detailed methodology used across four project countries has been described elsewhere6. In brief, our formative research study in Uganda employed a qualitative, inter-disciplinary, team-based approach, guided by an ecological conceptual framework. This ecological framework recognizes that individual health behaviors are influenced at different levels within a complex environment6.The ecological framework adapted for HPV vaccine introduction consisted of five levels of influence that formed the basic units of analysis, and defined the key target groups to be included in the formative research9. The important attributes and rationale defined at each level shaped the topics and research questions explored in our study. The outcomes of interest within each level were behaviors (individual or collective decisionmaking) that would either support a girl receiving the HPV vaccine or foster institutional decisions that would result in successful HPV vaccine delivery. A cross-sectional descriptive study design was adopted and qualitative data collection methods were used to facilitate a broad, in-depth understanding of sociocultural, vaccine delivery, and policy issues critical to the introduction of the HPV vaccine. The socio-cultural component explored social and cultural factors that could influence whether a young girl participates in an HPV vaccination program, including: an understanding of common health problems that adolescents face; knowledge about and experience with cervical cancer and HPV, its causes and cures; perceptions about and previous experiences with vaccination and the HPV vaccine; and the social context of health decision-making (including vaccination) for young adolescent girls. The health systems component gathered information on vaccine delivery options including relevant structures, processes, and capacities for vaccine delivery at the national level; readiness for vaccine delivery at the local level; suitability of existing institutional structures (e.g. schools, primary health services) for delivering the vaccine to young adolescents in communities; and likely impact of vaccine introduction activities on these institutions. The policy component reviewed the relevant health policy environment, mapping key stakeholders in decision-making processes and identifying critical issues important to national decision-making about cervical cancer prevention services, including new vaccine adoption. The research was carried out in five districts from the four major regions of Uganda, and included: Gulu in the north, Soroti in the east, Mbarara in the west, and Masaka in the central region. Kampala, the capital city, was included because of its multi-ethnic and cosmopolitan nature, reflective of national diversity. Selection criteria for study locations included regional and socio-cultural variations, major language groupings, differences in vaccination experiences, prevalence of cervical cancer, and existence of regional referral hospitals where information about cervical cancer prevention exists. The study populations spanned five levels: children aged 10–12 years (individual level), parents/primary caregivers and head teachers/teachers (interpersonal level), community and civic leaders (civil society), health professionals (institutional level), district and national political and technical leaders (policy level) (Table 1). A total of 71 focus group discussions and 107 key informant interviews were conducted with a cross-section of the population (Table 1), in addition to a large stakeholder workshop to discuss vaccine delivery options. Cold chain assessments and desk review of relevant government documents supplemented the research. Data were collated and analyzed thematically using an iterative, teambased process (A. Bingham, PhD, et al., unpublished data, June 2008). A codebook-based approach10,11 using Table 1. Study population, selection criteria, sampling procedure and data collection method
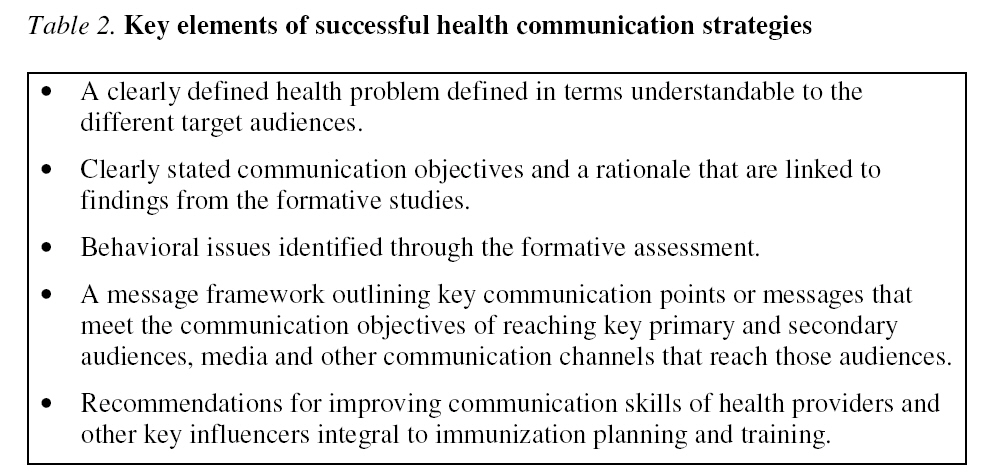
* FGD: focus group discussions; PTA: parent-teacher association; KI: key informant interview; EPI: expanded programme on immunization ATLAS.ti textual data management software (Berlin, 2007) was employed to further synthesize and summarize findings by theme, study group, and district. Results Socio-cultural findings While cervical cancer is one of the most common reproductive health malignancies among women in Uganda, there has been very little awareness about it. When asked what they knew or had heard about cervical cancer, the majority of respondents knew very little about the disease as illustrated by these extracts from focus group discussions: We mostly know about cancer of the uterus and cancer of the breasts…We have not heard about cervical cancer. (Female parent) We have heard that there is cancer of the cervix and that it affects women but we do not know what it is and what causes it. (Male parent) Cancer of the cervix was rarely mentioned spontaneously among the common reproductive health problems faced by women, nor among the cancers known to affect only women. Mention was made, however, of cancer of the uterus. In each of the four languages commonly used by our respondents (Luganda, Runyankore, Atsei and Luo), there was specific terminology used to refer to cancer of the womb. The womb was understood to be a single organ and no distinction was made in terminology between cancer of the uterus and cancer of the cervix. However, it was evident that cancer of the cervix was understood locally in terms of some of its symptoms rather than by its specific anatomical location; hence the lack of specific terminology for it. Health workers introduced to terminology that attempted to distinguish between the two cancers, whereby cancer of the cervix was translated as “cancer of the opening or mouth to the womb.” This terminology was not well known among non-health professionals, as indicated by this comment: I have never heard about cancer of the cervix. What is the difference between the cervix and the uterus; we thought it was the same thing. Anyway, what we know is that there is a uterus and that the cancer affects the uterus…since the cervix is part of the uterus then there is no difference because in both cases the uterus is affected. (Female parent) Cancer of the cervix was associated with three major symptoms: foulsmelling vaginal discharge, sores or wounds that do not heal in and/or on the womb, and abnormal vaginal bleeding. Again, we found different local terminologies were used to explain each of these symptoms. When translated to English, these local terms illustrate nuances of disease awareness that may be important for health education campaigns or messaging. For example, in the local Ateso language, the word for foul-smelling vaginal discharge literally meant that the discharge was uncontrollable, foulsmelling, and required heavy padding in order to conceal it – implications that go beyond just the symptom and extend to what to do about that symptom. In another example, in the local Runyankore language the word for abnormal bleeding literally implied a condition of continuous heavy vaginal bleeding; this same word was also used in the Runyankore Bible translation in relation to menstruation or bleeding. The majority of respondents were unaware of the fact that cervical cancer is caused by HPV, which is sexually transmitted. There was general awareness, however, that its causality may be sexually related, as illustrated by the common risk factors listed by respondents from all of our study regions: promiscuity, multiple sexual partners, early sexual debut, high parity, untreated sexually transmitted infections, intercourse during menstruation, and use of modern family planning methods (especially pills, IUDs and injections). Poor personal and menstrual hygiene, and frequent deliveries and abortions, especially those that are unsafe, were also mentioned as risk factors. The majority of respondents, including children aged 10 to 12 years, had a good understanding of the benefits of vaccination, indicating that it was for disease prevention, protection, or reduction of severity of disease. I like it because when you are immunized, nothing disturbs you in future. When I was immunized, serious disease did not affect me. I like it because there are certain diseases that could come in future that could kill you. I find immunization is good because the disease for which you are being immunized will not disturb you. (Focus group discussion comments by schoolchildren, Gulu) The observed declines in prevalence of vaccine-preventable diseases, such as polio and measles, was recognized among respondents and contributed to increased acceptance of vaccinations in the communities. Initially I refused to have my children immunized because we had been told that if your children were immunized they would die. I only had my baby immunized after I realized that those children who had been immunized against measles did not get measles; even when they did it was mild. (Female parent, Mbarara) Despite this knowledge, however, concerns were expressed in all study areas regarding issues of vaccine safety in general, adverse effects following immunization, and the use of untrained vaccinators in the communities, illustrated by these extracts from a focus group discussion with out-of-school girls in Masaka: The health worker may be vaccinating the child when the needle breaks and gets stuck inside the body. The nurse might forget and use a needle on more than one child. Some of these vaccines are sometimes bad. The nurse may give it to the child without first reading the instructions, only to notice, too late, that the drug is expired. The nurse might give a child an overdose…what if the child is immunized and they die after the vaccination? Sometimes the vaccines are transported badly and they get spoilt and when they vaccinate someone they get problems like being lame. How will we know that the vaccine is safe? The need for reassurance that the vaccine is safe and that the girls are not being used as guinea pigs for a new vaccine was emphasized, as was the need for endorsement of the vaccine by the Ministry of Health (MOH) and other health professionals. Furthermore, the need for information regarding cervical cancer, the HPV vaccine, its safety, side effects, and where HPV vaccination has been carried out previously was also emphasized. Health system findings A school-based strategy was identified by the majority of respondents as being the most convenient and effective way of reaching pre-adolescent girls given the fact that the majority of girls in this age group are enrolled in school following the enactment of the Universal Primary Education policy in 1997. Respondents did raise concerns about whether girls in school will be vaccinated by age or by grade/class. Given that girls in school are grouped by grade/class, vaccinating by age was seen as more challenging logistically, even though selection by age was commonly carried out by health workers for other vaccines. Vaccinating by age in school may also be complicated by an inability of school administrators, parents, and guardians to know the exact age of the children. On the other hand, vaccinating by grade/class had its own challenges, such as wide age range in grades/classes in rural schools, arising from children starting school late and repeating grades/classes. In the absence of health services that target 10–12-year-old children specifically, national-level policymakers suggested integrating HPV vaccine into the Child Days Plus (CDP) program. During April and October each year, the CDP delivers an integrated package of preventive services (e.g. catch-up immunizations, Vitamin A supplementation and de-worming medicine) to all children aged 14 years and younger through schools, health units and other outreach centers, such as churches, community centers and local council offices12 .Respondents noted that the CDP program is well established, is accepted by the community, has mechanisms for reaching those out of school, has some resources allocated for implementation, and has denoted the responsibilities of the different stakeholders involved. Not all respondents embraced CDP as a delivery mechanism for HPV vaccination. For example, technical and administrative staff at the district level suggested initially delivering the HPV vaccine as a stand-alone program, and only later, after it was well-established, considering integration with CDP or other existing health programs. Their argument was that new vaccine introduction necessitated more intensive community mobilization and education, which could be easier to implement if the HPV vaccine had its own program with an independent budget, enabling health staff to focus full attention and resources exclusively on HPV vaccination. Any resistance to HPV vaccine would not negatively impact other existing services or immunization programs if it was delinked from those efforts. The process of successful implementation of the HPV vaccine initiative was considered to be dependent on momentum and leadership from the national level in the MOH, and on the district commitment to the program. Policy findings Respondents participating in the policy key informant interviews noted that Uganda does not have a national cervical cancer screening program and outlined challenges in establishing one. Therefore, some policymakers and implementers expressed the opinion that HPV vaccines could be a potentially longer-term solution to cervical cancer prevention. Respondents noted that introducing the vaccine would not require a completely new policy, as existing MOH Reproductive Health division and Expanded Programme on Immunization policies were found to be sufficient to accommodate both secondary (screening and treatment) and primary (vaccination) prevention for cervical cancer. However, it was noted that policy guidelines would need to be established embodying national standards and capacities of Uganda to undertake this intervention. It would also be necessary to prioritize the intervention and to place it in the mainstream of ongoing programs. This would provide the legal and regulatory framework necessary for HPV vaccine implementation. Discussion Information gathered from the formative research was designed to inform the development of three outputs key to implementing HPV vaccine delivery demonstration projects: (1) an HPV vaccine delivery strategy appropriate to the target age group of young adolescent girls; (2) a communication strategy and materials to support a positive environment for vaccine acceptance at the individual and community levels; and (3) a national advocacy plan to achieve support for cervical cancer prevention and vaccine introduction among policymakers and key stakeholders at regional and national levels. How our results from the formative research can be used to inform these outputs is discussed below, in light of current thinking for best practice in Uganda. Acceptable HPV vaccine delivery Current WHO HPV vaccine introduction guidelines suggest that an acceptable HPV vaccine delivery strategy needs to address some key issues in its design: identify the most convenient and effective way of reaching target populations prior to HPV exposure; ensure that vaccination is viewed as an integral part of a comprehensive approach to cervical cancer prevention, including screening and treatment; develop and maintain strong partnerships between programs needed for successful delivery; and carefully plan for the most efficient use of existing, or—where necessary—strengthened, services13 .Our formative research found that the most convenient and effective way of reaching adolescent girls prior to exposure would be through school-based delivery, given the high levels of attendance in school by girls aged 10–12 years. Vaccination by age or grade was an outstanding issue and would need further investigation to more fully inform which selection criterion works best in the school setting. Stand-alone delivery and integration with CDP program activities are also potential delivery strategies that could effectively reach young adolescents prior to sexual activity. Without a clear consensus on which would be more effective in the Uganda context, studying and evaluating both delivery strategies in pilot projects may prove beneficial. Which division within the MOH should be responsible for national-level coordination of HPV vaccination requires close consideration, given that the HPV vaccination is linked with reproductive health, immunization, adolescent health and cancer. Policymakers interviewed in our study emphasized the need to include the Reproductive Health division, the Uganda National Expanded Programme on Immunization (UNEPI) and the School Health Program (which was not functional at the time of the research) in a collaborative partnership that included integration of HPV vaccination expenses and activities into their budgets and work plans. As was noted from most respondents, UNEPI was best placed to lead this partnership because of its relatively strong infrastructure, existing facilities for vaccine storage and transport, human resources, and longstanding direct links with district leaders and health workers. Integration of HPV vaccine delivery into existing systems and structures would likely be more sustainable, as suggested in WHO guidelines13 . Government and district ownership of the program were viewed as a cornerstone for the vaccine’s sustainability. This entails including the HPV vaccination in the national budget and ensuring that the HPV vaccination strategy is part of the MOH’s work plans and the medium term expenditure framework. Effective coordination and communication from the national level to districts and between the health and education sectors would be important in order to allow for adequate planning, logistics, and training. Appropriate and relevant communication strategy Research suggests that a wellplanned, adequately-funded strategic communication plan can help immunization programs keep and maintain coverage targets14 . Immunization levels sometimes drop because the quality of information is poor. Communication is essential to achieve coverage goals, especially in hard-to-reach populations, and is needed to build trust in vaccines among groups who question them.15,16 Health communication experts recommend a few key elements to successful communi-cation strategies (Table 2).13,16,17 Our findings from the formative research confirm that communication messaging needs to be clearly defined and directed given the low awareness about cancer of the cervix, its etiology and the availability of vaccines for prevention. An effective communication strategy in the Ugandan context would address issues related to delivery to girls only, the newness of the vaccine, and the unique age group solicited for vaccination, as they are outside of the usual under 5-year-olds normally about cervical cancer, HPV, and the HPV vaccine, using local terms and languages.
Directed and effective advocacy strategy The main purpose of an advocacy strategy for immunization is to generate and maintain support of vaccine programs among health policymakers and key national level decision-makers18 .Their support includes creating policies favorable for vaccination introduction activities and demonstrating financial commitment for vaccine introduction14.Key health policymakers and other stakeholders will need to advocate for immunization programs in order to persuade governments, donors, and other actors to support vaccine programs in light of other pressing health programs and priorities that are of importance to Uganda. A clear challenge for any advocacy strategy is the ability to respond to the specific information needs of national policymakers who are making decisions about whether to invest in a new vaccine in resource poor countries battling a myriad of pressing health and economic priorities19. The need for an advocacy strategy to inform and mobilize policymakers was a clear need identified by respondents in our study. This strategy should target members of parliament, MOH top management, program managers, health professional associations, line ministries’ district leadership, development partners, health activists, and the media (who are also the stakeholders for advocacy identified in other research).13,15,16,18-20 The advocacy strategy should primarily aim to solicit political will and active support that allows specifically for policy change favorable to HPV vaccine adoption, and more broadly for cervical cancer prevention.15,20 Because policymakers reported an absence of a national cervical cancer screening program in Uganda and the WHO recommends HPV vaccination as one component of a comprehensive cervical cancer prevention strategy, advocacy efforts will need to be specific as to why HPV vaccination is an option for Uganda and how screening and treatment as secondary prevention for cervical cancer can be supported. Our findings suggest some key elements of an effective advocacy strategy for Uganda, which are in line with those elements suggested by others:13,16,18
Conclusion Our formative research study was designed to guide development of a vaccine delivery strategy, a communications strategy (for outreach to communities), and an advocacy strategy (for outreach to policymakers) through the exploration of the socio-cultural milieu, health systems structures, and policy environment across a range of populations. Our research suggests that the most convenient and effective way of reaching adolescent girls aged between 10 and 12 years for HPV vaccination would be through a school-based delivery strategy. Two other strategies were suggested: stand-alone and linking with the CDP program. Furthermore, our research found that introducing HPV vaccination to a population with low awareness about cancer of cervix and the HPV virus necessitated a carefullyplanned communication strategy, and specific messages were suggested. The need for an advocacy strategy to inform and mobilize policymakers was emphasized throughout the formative research, and suggested components of such a strategy were summarized. As a next step, the vaccine delivery, communication, and advocacy strategies are being implemented and evaluated through a small demonstration project in two districts of Uganda. The findings from the demonstration project— anticipated in 2010—will help contribute to the evidence base that the government of Uganda can draw from when deliberating whether and how to introduce HPV vaccination to the country and strengthen cervical cancer prevention efforts. Acknowledgements We extend gratitude to our study contributors: Ivan Lyazi, Alex Jurua, Stephen Mawa, Majid Aziz, and all research assistants; Judith Ajeani, Godfrey Habomugisha, Musa Sekikubo, Carol Nakisige, Miriam Nakalembe, and Frank Kaharuza from the Association of Obstetricians and Gynaecologists of Uganda; Stella Ekallam, Robin Biellik, Amynah Janmohamed, and Scott Wittet from PATH; parliamentarians, senior officials from UNEPI and Ministries of Health, Education and Sports, and Gender, Labor and Social Development; officials, leaders, health providers, teachers, school administrators, religious and community leaders, and participants from Gulu, Kampala, Masaka, Mbarara, and Soroti; and other valuable external partners. Generous funding for this work was provided through a grant to PATH from the Bill & Melinda Gates Foundation. References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08045t2.jpg] [rh08045t1.jpg] |
| |||||||||

{kind=link}