 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
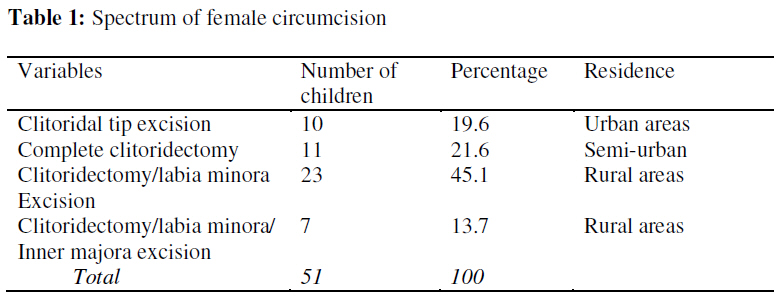
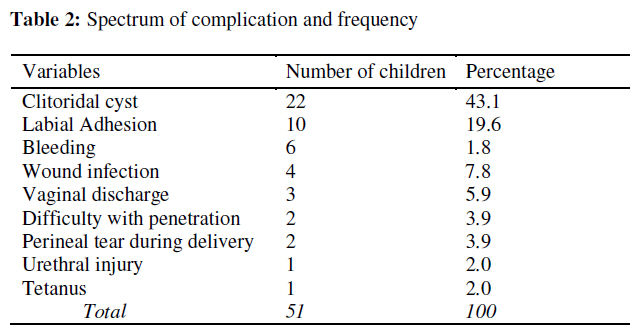
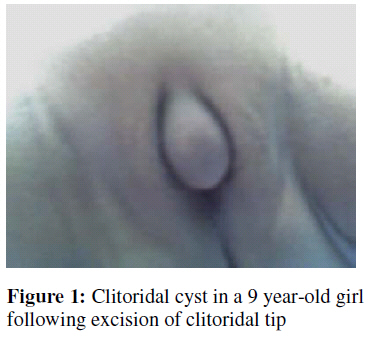
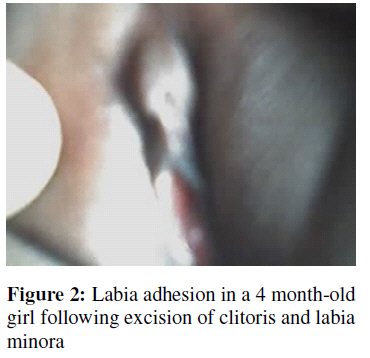
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 17-25 Original Research Article Female Genital Mutilation among Edo People: The Complications and Pattern of Presentation at a Pediatric Surgery Unit, Benin City La mutilation génitale féminine chez le peuple Edo : Complications et la manière dont elles se présentent dans un centre de chirurgie pédiatrique à Bénin City.David Osarumwese Osifo1 and Iyekoretin Evbuomwan1 Pediatric Surgery Unit, Department of Surgery, University of Benin Teaching Hospital, Benin City, Nigeria Code Number: rh09003 ABSTRACT This prospective study on female genital mutilation among Edo people was based on female children and parents who presented on account of it at the University of Benin Teaching Hospital, Benin City, Nigeria, between January 2002 and December 2007. During the period, 51 female children aged 10 days and 18 years presented with complications following genital mutilation. Twenty-nine were brought by their parents for mutilation while 67 parents interviewed believed strongly on female genital mutilation with 47 mothers mutilated. Religio-cultural and superstitious beliefs were the main indications and the type of mutilation ranged from excision of clitoridal tip in 10 (19.6%) children to complete excision of the clitoris, labia minora and inner layer of majora in 7 (13.7%). Complications ranged from clitoridal cyst formation in 21 (41.2%) to life threatening infections with one mortality due to tetanus infection (Afr J Reprod Health 2009; 13[1]:17-25). RĖSUMĖ Cette étude prospective sur la mutilation génitale féminine chez les Edos a été basée sur les jeunes filles et des parents qui se sont présentés à ce sujet au Centre Hospitalier Universitaire de Bénin City, Nigeria entre janvier 2002 et décembre 2007. Au cours de cette période, 51 jeunes filles âgées de 10 jours et 18 ans se sont présentées à l’hôpital avec des complications suite à la mutilation génitale. Vingt-neuf parmi elles ont été amenées par leurs parents pour la mutilation alors que 67 parents qui ont été interviewés croyaient fermement en la mutilation génitale féminines et 47 mères ont subi la mutilation. Les croyances religio-culturelles et superstitieuses ont été les principales indications et le type de mutilation variait de l’excision du bout du clitoris de 10 (19,6%) enfants jusqu'à l’excision totale du clitoris, de petites lèvres et de la majora interne chez 7(13,7%). Les complications variaient de la formation du kyste clitoridien chez 21(41,2%) jusqu’aux infections dangereuses, un décès étant causé par le tétanos (Afr J Reprod Health 2009; 13[1]:17-25). KEYWORDS: Female, Circumcision, Mutilation, Complications, Presentation Introduction Circumcision, the surgical excision of the prepuce, is one of the oldest and most commonly performed operations1 . In sub-Saharan Africa, both male and female circumcisions were practiced as religious and cultural rites and sometimes as one of the initiation rituals to manhood and womanhood2 . The uncircumcised was regarded as taboo, uncultured and uncivilized and as such treated with contempt. Although the Christian and Islamic religions encouraged only male circumcision, both male and female circumcisions were widely practiced in this subregion before and after the advent of these religions3-5 . Female circumcision (genital mutilation) has been widely condemned by both government and non-governmental organizations worldwide. The international and local outcry against female circumcision led many governmental agencies across Africa to prohibit the practice in government and private health institutions6 . Rather than stemmed this cultural menace, the practice became underground and is widely carried out today by traditional health providers which led to resurgence of complications following female genital mutilation. The Edo people are the main ethnic group in Edo State, Nigeria, and like other ethnic groups in Africa, female genital mutilation is done for various religious and cultural beliefs which have been difficult to eradicate despite western education 7,8 . The types and extent of genital mutilation is a spectrum from clitoridal tip excision (type I) to complete clitoridal excision with labia minora/inner layer of majora excision (type III). Many community practice neonatal circumcision while others do it at any age as part of initiation rites. These result in a spectrum of complications, and the pattern of presentation depends on the extent of tissue excised, place of residence, the intensity of outcry against female genital mutilation in the community where the victim resides as well as cultural belief that saw complication arising from circumcision done as initiation rites as blessing from the gods which does not require medical attention3-8 . Even though earlier researchers7-9 debunked cultural claims and revealed that female uncircumcision was safe, and many literatures 3-8,10-14 have documented various forms of circumcision related complications including deaths, particularly in sub-Saharan Africa, the practice is still widely embraced. The need to eradicate this cultural menace, therefore, cannot be overemphasized. In the past six years we managed many female children who presented with complications after genital mutilation. The aim of this study is to draw attention to the fact that female genital mutilation is still rampant in this subregion, highlight the spectrum of complications and the mode of presentation so as to increase awareness and heightened public and government campaign against it. Patients and Methods This prospective study was undertaken among the Edo people, the main ethnic group in Edo State, at the University of Benin Teaching Hospital, Benin City, Nigeria. Consecutive cases of female children who presented with complications after genital mutilation, between January 2002 and December 2007 were recruited for the study. Records were taken of their age, type and extent of mutilation, complications and place/personnel that carried out the mutilation. Also, female children that were brought to the unit hopefully for genital mutilation were noted. Available parents/caregivers were interviewed to know their socioeconomic status, place of residence, level of education, reasons for presenting their children for mutilation/why their children were mutilated, and to know if the mothers themselves had genital mutilation. Thereafter, the parents and the grown up girls were recruited for counselling and the children were treated based on the complications they presented. Statistical analysis The data obtained were analyzed using SPSS and presented as count, frequency and percentage. Continuous data were expressed as mean/standard deviation while categorical data were analyzed using Chi-square test and p-values less than 0.05 were regarded as significant. Results During the period, 51 female children aged 10 days and 18 years (mean 5 years ± 1.6) presented with complications after mutilation, while 29 female children were brought by their parents or caregivers for mutilation. Cultural practice was the major indication for circumcision among the Edo people who accounted for 49 (96.1%) of the 51 children treated. Of the 67 parents available for interview, all (100%) believed uncircumcised female was a taboo, 42 (62.7%) mutilated their daughters or brought them for mutilation as a mark of cultural identity, 24 (35.8%) to prevent promiscuity, 21 (31.3%) believed circumcision was done for hygiene purposes as the uncircumcised female was filthy and the vagina/vestibule aesthetically poor. Ten (14.9%) parents brought their daughter for circumcision so as to have safe delivery during reproductive age, 8 (11.9%) believed babies would die on making contact with the clitoris during delivery and 4 (6.0%) as initiation to womanhood. All the 47 mothers, aged 20 and 59 years (mean 37 years ± 1.9) interviewed, admitted they themselves were mutilated as children. The parents of 30 (58.8%) children that presented with complications were of low socioeconomic group and resided in rural areas with their children, 14 (27.5%) were semi literate parents while 7 (13.7%) were educated elites. Traditional healers were responsible for the mutilation of 48 (94.1%) children while 3 (5.9%) were mutilated by paramedical staff. The types of genital mutilation as shown in Table 1, was a spectrum from excision of clitoridal tip in 10 (19.6%) children to complete excision of the clitoris, labia minora and inner layer of majora in 7 (13.7%). These operations (mutilations) were performed without anaesthesia and analgesia, surgical instruments used were recycled without sterilization and the environment was usually septic. Also, many female children during ritual circumcision were assembled and circumcised the same day with the same unsterilized surgical instruments. The majority of children from rural areas had more complications because complete excision of clitoris, labia minora and inner layer of majora was the common procedure. Medical attention was sought very late and first aid treatments given before presentation were native concoctions application which usually led to introduction of infections. Therefore, an extremely significant statistical difference was observed when life threatening complications recorded among the rural dwellers were compared with other children (P<0.0001). The complications recorded (table 2) also reflected the extent of tissues excised from the vestibule during the procedure. Clitoridal tip excision and clitoridectomy were complicated by clitoridal cyst formation in 21 (41.2%) children with a significant statistical difference observed (P=0.0021) and this required cystectomy and total clitoridectomy (Figure 1). Hemorrhage from clitoridal arteries recorded in 6 (11.8%) children was controlled by pressure dressing in 2 and ligation of the bleeding vessels in 4 children. Labia adhesion diagnosed in infants (Figure 2) were treated by breaking down the adhesion with artery forceps because 8 of them were flimsy fibrous tissues, but 2 children had dense adhesion that required examination under general anaesthesia and labia separation. Adhesions that were not diagnosed in infancy were the cause of difficulties with penetration in 2 girls during sexual intercourse. These girls were anxious because of pressures from their spouses and friends and apart from surgical procedure that was done, they needed and had counselling. Two had perineal tear during delivery as a result of vestibular scars from childhood circumcision which were not diagnosed until delivery at traditional birth attendant homes. They presented following uncontrolled bleeding which required examination under general anaesthesia and repair of the tear. Although the 6 children that presented with infections and vaginal discharge responded to antibiotics, the 3-month-old child from rural area that had tetanus, died on the second day on admission because she was presented very late. Counselling of the parents was not easy during the period. Majority of them attributed the complications to unseen forces as they argued that the traditional healers who did the mutilations were trusted hands who had circumcised many females in their community without complications. However, paying hospital bills to treat the complications was not easy for many of them especially the low socioeconomic group and this served as a deterrent to many of them. In addition, counselling at every opportunity was done. Those who brought their female babies for mutilation as well as those whose babies had complications were not allowed home until they were counselled by nurse counsellors. Whereas of the 67 parents interviewed and counselled 61 (91.0%) agreed to stop female genital mutilation, 6 (9.0%) refused on the ground that their culture/custom shall not be broken in their time and subsequently defaulted from counselling sessions. On the whole, one death was recorded following female genital mutilation during the period. Discussion The results from this study are similar to results from previous studies1-7 in this subregion which showed that female genital mutilation is still very rampant. Of the 67 parents interviewed, all (100%) believed strongly in female genital mutilation, 47 mothers were mutilated, 51 children had complications and 29 female children were brought for mutilation during the period. Religiocultural and superstitious beliefs were the main indications for female genital mutilation despite the long contact with western civilization. The beliefs: that uncircumcised female is a taboo, circumcision is a mark of cultural identity, to prevent promiscuity, circumcision is hygienic as the uncircumcised female was filthy and the vagina/vestibule aesthetically poor were common. Also, many believed that circumcision allow safe delivery during reproductive age, babies wound die on making contact with the clitoris during delivery and as part of initiation rites to womanhood. Although ridiculous, these were strongly believed by the Edo people which tally with the results of earlier researches 7,8 conducted among other ethnic groups in Nigeria. Moreover, the educated elites were involved as shown in this study even though the low socioeconomic rural dwellers presented late with more life threatening complications with a significant statistical difference observed (P<0.0001). From the interview conducted among available parents in this study, there are no scientific evidence to support these beliefs and researches by previous authors 7,15,16 showed that these beliefs are myths that have been handed over from one generation to the other and there was no proof that female genital mutilation controlled promiscuity; affected fertility or increased female hygiene. The type and age at circumcision varied from one community to the other, hence the children presented between the ages of 10 days and 18 years (mean 5 years ± 1.6) with mild to very severe life threatening complications. Previous studies 17,18 done in Nigeria in the 80’s suggested a decline in female genital mutilation with consequent drop in the numbers presenting with complications. The international and local outcry against female genital mutilation only succeeded in making it underground practice and is now performed secretly by traditional healers who have no knowledge about female genital anatomy. Therefore, there is resurgence of complications which present very late after traditional remedies have failed. Majority of the children with clitoridal cyst presented themselves after many years of traditional treatment. Self reporting following persistent complication in a grown girl was the more common pattern of presentation as also reported by similar author19 . Therefore, profuse uncontrolled bleeding, difficulty with penetration during sexual intercourse and perineal laceration during delivery made most of them sought medical attention. Conversely, those circumcised who could cope with the complications never sought medical attention. However, many female who had gynaecological complications were treated by the Gynaecologists and this partly explained the fewer number of patients seen in this series compared with that reported earlier by Gynaecologists3-5 in a similar setting. The risk of infections and transmission of infections following female genital mutilation, particularly when it is done with unsterilized instruments and in septic environments, documented by authors20,21 and which is the common practice by traditional healers, have been many these agreed with the results of this present study. Of the children that had infection after circumcision, the 6 children that presented with pelvic inflammatory disease and vaginal discharge responded to antibiotics. Unfortunately, the 3-month-old child who was brought from rural area with tetanus, which commenced few days after circumcision, died on the second day on admission because she presented very late after traditional remedy had failed. Previous authors 10,19 also reported the transmission of HIV following female circumcision. Counselling played a pivotal role during management, every opportunity was used to counsel the parents, caregivers and the grown up girls. Although there was initial resistance, cooperation has increased as many pastors now preach against female genital mutilation. Traditional chiefs and priests are also now convinced of the hazards of female genital mutilation as many of them now counsel people against it..This approach is very rewarding because Edo people respected their opinion more than orthodox doctors as previously reported22 . Also, the nursing counselling unit of the hospital was alerted each time there was a case of female genital mutilation and they followed up with home visits after thorough counselling in the hospital. Nevertheless, of the 67 parents interviewed and counselled within the hospital during the period, 61 (91.0%) agreed they would stop the practice while 6 (9.0%) refused and were lost to followup. In conclusion, female genital mutilation is still a common practice among the Edo people in particular and in sub-Saharan Africa in general. Complications following female genital mutilation which ranged from clitoridal cyst to life threatening infections were concealed until very late for fear of possible prosecution, and assurance by traditional healers that circumcision related complications do not require orthodox medical attention. The victims only sought orthodox medical attention themselves either as a result of uncontrolled complications or due to life threatening complications which failed to respond to traditional medications. Counselling through traditional rulers, priests and pastors as well as nursing staff were very rewarding. There is need to improve health awareness campaign and government policies which will increase women and female children awareness of the hazards of female genital mutilation. Those with complications should have access to free medical treatment. There is also a need for international collaboration to stop this cultural menace that has caused suffering and death of many innocent female children. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09003t1.jpg] [rh09003f2.jpg] [rh09003f1.jpg] [rh09003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}