 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
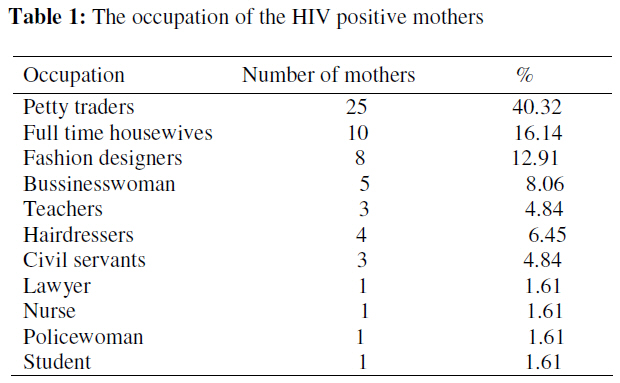
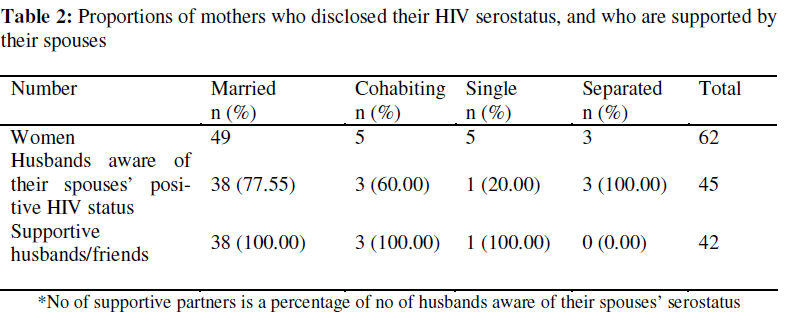
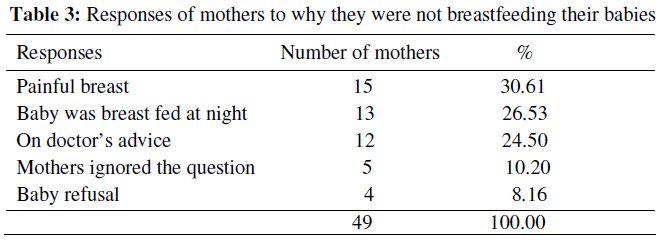
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 27-35 Original Research Article Experiences of HIV positive mothers who chose not to breastfeed their babies in Nigeria Les expériences des mères séropositives qui choisissent de ne pas allaiter leurs bébés au NigériaWilson E. Sadoh1* and Ayebo E. Sadoh 2 1 Lecturer/ Consultant Paediatrician, Dept of Child Health, University of Benin/ University of Benin Code Number: rh09004 ABSTRACT HIV positive mothers, who choose not to breastfeed their babies in a predominantly breastfeeding community would face a number of barriers. This study looked at the experiences of HIV positive mothers who chose the no breastfeeding option. Consecutive HIV positive mothers who opted not to breastfeed their infants after infant feeding counselling and whose infants were attending the HIV programme at the University of Benin Teaching Hospital, Benin City, Nigeria were recruited for the study. Disclosure of HIV serostatus and adherence to no breastfeeding options were evaluated using an interviewer administered structured questionnaire. Of the 62 mothers recruited for the study, 57 (91.94 %) had disclosed their serostatus to at least their partners. Most partners 42 (93.33%) were supportive while three mothers were divorced following disclosure. Thirteen (20.97%) mothers could not comply with no breastfeeding. Non disclosure of serostatus, pressure from extended family and token breastfeeding mitigate against adhering to no breastfeeding by HIV positive mothers (Afr J Reprod Health 2009; 13[1]:27-35). RĖSUMĖ Les mères séropositives qui choisissent de ne pas allaiter leurs bébés dans une communauté qui pratique principalement l’allaitement rencontreraient des obstacles. Cette étude a examiné les expériences des mères séropositives qui ont choisi de ne pas allaiter. Les mères séropositives consécutives qui ont choisi de ne pas allaiter leurs bébés après l’orientation sur l’allaitement au sein et dont les enfants suivaient le programme sur le VIH au Centre Hospitalier Universitaire à Bénin City, Nigeria ont été recrutés pour l’étude. La révélation de la séropositivité et l’adhérence aux options de ne pas allaiter ont été évaluées à l’aide d’un questionnaire structuré administré par un interviewer. Sur les 63 mères qui ont été recrutées pour l’étude, 57(91,94%) avaient révélé leur séropositivité au moins à leurs partenaires. La plupart des partenaires 42 (93,33%) ont soutenu leurs femmes, alors que trois mères ont subi le divorce suite à la révélation. Treize (20,97%) mères ne pouvaient pas respecté le non-allaitement. La non-révélation de la séropositivité, la pression de la part de la famille étendue et l’allaitement symbolique font que les mères séropositives n’acceptent pas de ne pas allaiter (Afr J Reprod Health 2009; 13[1]:27-35). KEYWORDS: Barriers, Disclosure, Breastfeeding choices, Support Introduction HIV/AIDS has profound effects on physical, emotional, social and economic wellbeing and addressing these dimensions of life is an integral part of HIV care1 . When confronted with a chronic and serious illness like HIV/AIDS, fear of stigmatization and social isolation can be great sources of suffering for some affected individuals.2-4 Thus psychological support which include counselling to practical assistance is required for people living with HIV/AIDS (PLWHA).1,5 While this support is often sought from close relations/ friends, disclosure of the serostatus to these persons would be most likely required in order to elicit their support. The process of disclosure is stressful, largely because of uncertainty of evoking a positive response. Thus, initial individual and or group counselling, for spiritual /religious support maybe necessary.2,6 A group of PLWHA who especially require support are mothers infected with HIV.7 This is with specific regards to feeding choices. Feeding recommendations for HIV infected mothers range from no breastfeeding at all to exclusive breastfeeding for short periods and mothers are to be supported in their choice of infant feeding option.8 For a community that predominantly breastfeeds,9 the decision by a mother not to breastfeed will be met with challenges especially in creating an enabling home environment to adhere to no breastfeeding options and prevent postnatal maternal to child transmission. An enabling environment in terms of financial resources and social support to carry out replacement feeding will often require disclosure of serostatus to elicit a positive response from family members/ partners. It is against the foregoing that we decided to look at some of the challenges faced by mothers infected with HIV who chose a no breastfeeding option, and to determine the form of support received and evaluate the effect of serostatus disclosure on support and adherence to no breastfeeding option by HIV infected mothers attending an HIV treatment programme. Subjects and Methods The subjects were amongst consecutive HIV infected mothers attending the paediatric antiretroviral therapy programme of the University of Benin Teaching Hospital (UBTH). The mothers had been counselled during the antenatal period or intrapartum on the infant feeding choices using the Nigerian National guidelines on infant feeding choices.10 The options were exclusive replacement feeding with breastmilk substitutes if it is acceptable, feasible, affordable, sustainable and safe (AFASS) or exclusive breastfeeding for three to six months if AFASS cannot be achieved. Those who opted for exclusive replacement feeding (no breastfeeding option) were recruited for the study. The adherence to no breastfeeding option and challenges faced by the mothers were evaluated using an interviewer administered, structured questionnaire. The authors interviewed all cases and the interviewee was the mother in all cases. Verbal consent was obtained from the interviewees. The Study was carried out between July 2005 and February 2007. The questionnaire sought information on biodata; which included age, marital status and level of education attained by the mother. Information on disclosure of their HIV status to other(s), presence or absence of financial and/or moral support and source of the support were also obtained. Financial support consisted of financial assistance towards the care of the HIV positive mother while moral support was taken as empathy and practical support of the infected mother. Mothers were asked if they had been counselled on infant feeding choices, while their knowledge of and satisfaction with the reason for their choice not to breastfeed was evaluated. The mothers adherence with and barriers to the no breastfeeding option were determined. The reasons for non adherence including token breastfeeding defined as an occasional breastfeeding usually to pacify the child were evaluated. Information was also sought on whether mothers’ choice not to breastfeed had been questioned and by whom. The responses of the mothers to such queries were noted. The socioeconomic class of the mothers was determined using the methods described by Olusanya et al.11 Information on maternal antiretroviral therapy, sources of water, adequacy of preparation and other infant feeding practices are the subject of a previous publication.12 Statistical analysis Data was analysed using the SPSS for windows 10.0 (SPSS Inc. Chicago, IL). Simple Proportions were expressed in percentages. Differences in proportions were evaluated using Fisher’s exact test. Differences in means were determined using one-way ANOVA with turkey-Kramer multiple comparison tests. Level of statistical significance at 95% confidence interval was set at <0.05. Results During the study period, 62 mothers who had chosen the no breastfeeding option following infant feeding counseling. Of which 59 (95.16%) were counseled during antenatal period and 3 (4.84%) during labour. All 62 mothers opted to exclusively formula feed their babies. The programme did not offer free infant formula to HIV exposed infants. The mothers were aged 16 – 41 years with a mean of 30.63 ± 4.27 years. Most mothers 49 (79.04 %) were married, 5 (8.06 %) were co-habitating with a male partner whom they were still living with, 5 (8.06 %) were single and 3 (4.84 %) were separated from their husbands. The mean ages in years of the mothers that were married, cohabitating, single and separated were 31.04 ± 4.15 (range, 22 – 41), 29.00 ± 2.65 (range, 23 – 33), 28.86 ± 4.14 (range, 24 – 37) and 24.33 ± 7.37 (range, 24 – 37) years respectively. The differences in the means was significant, p = 0.045. Intra group multiple comparison showed that the married women were significantly older than the women who were separated from their husbands, p = 0.05. The reason for the separation in the three cases was because of HIV infection in the child and mother. Almost equal numbers of mothers came from the different socioeconomic classes, with 19 (30.65 %), 21 (33.87 %) and 22 (35.48 %) mothers from low, middle and high socioeconomic classes respectively. Almost half 27 (43.55 %) of the mothers had up to secondary school education, 21 (33.87 %) attained tertiary school education and 14 (22.58 %) of mothers had primary school education. Most mothers 25 (40.32 %) were petty traders. The distribution of the occupation of the other mothers is shown in Table 1. Most mothers 57 (91.94 %) had disclosed their HIV status to somebody. Of which majority 45 (78.95 %) were husbands/ partners, 5 (8.77 %) were parents, 3 (5.26 %) sisters and 4 (7.02 %) pastors. Single mothers (20.00%) were least likely to disclose their status to their partners, Table 2. Secondary disclosure was made to parents by 16 (28.07 %) mothers, to sisters in 5 (8.77 %) cases, pastors in 6 (10.53 %) cases and motherin-law in one (1.75 %) case. The other 5 (8.06 %) mothers did not disclose their HIV status to anybody. Fear of stigmatization and divorce were cited as reasons for nondisclosure. Of the 45 husbands/ partners who were aware of their spouses serostatus, 42 (93.33 %) were supportive both financially and morally while the other three became separated from their wives. All the parents gave both financial and moral support, while all the sisters and pastors provided moral support. The only mother-in-law that knew of her daughterin-law’s HIV status provided moral support. Of the 62 mothers who opted not to breast feed, 13 (20.97 %) could not adhere with no breastfeeding. Three (23.08 %) of these mothers had to recommence breastfeeding at 4 to 6 months of their infant’s life. The reasons given were family pressure (extended family) in two cases and a case where the infant was said to have refused formula. The three mothers who recommenced breastfeeding did not disclose their serostatus to their partners. The other 10 (76.92 %) mothers gave their babies “token” breastmilk to pacify the child especially in public. Of the 10 mothers, 3 (58.82 %) mothers had disclosed their serostatus to their partners while 7 (41.18 %) mothers did not disclose their serostatus. This difference was statistically significant, p = 0.0128. All the mothers correctly identified risk of HIV transmission to their babies as reason for being against breastfeeding. While all the mothers were satisfied with the reason given not to breastfeed, many 53 (85.48 %) were however unhappy not breastfeeding their babies. Of the other 9 mothers, six (9.68 %) felt inadequate not breastfeeding, three (4.84 %) expressed their feeling as bad, pained or bitter. All 62 mothers had however decided not to breastfeed to prevent HIV infection in their babies. A significant proportion of the mothers 49 (79.03 %) reported to being asked why they did not breastfeed their babies by mostly friends 25 (51.02 %) and mothers-in-law 24 (48.98 %). All 49 mothers gave evasive responses ranging from maternal ill health, painful breast, doctors advice to baby refusing to feed (Table 3). Discussion The maternal instinct to protect the young is exemplified by the mothers in this study opting not to breastfeed and thus prevent transmission of HIV to their children. In opting to formula feed, financial support would be required in these mothers who were mostly petty traders and full time housewives with limited resources. The need for financial assistance may have prompted the disclosure of their serostatus to their partners. Most partners were supportive of their infected spouses irrespective of the type of relationship. Thus, creating an enabling environment psychosocially and financially for replacement feeding to take place. Similar high rate of serostatus disclosure to partners and reason for the disclosure has been reported in a study done in Johannesburg, South Africa.13 We find in this study, that of those who could not adhere to the no breastfeeding option, majority did not disclose their HIV status to their partners. It has been shown that disclosure of HIV status to the partner is usually a major condition for successful replacement feeding.14 The disclosure of mothers’ HIV serostatus to close persons such as parents and sisters is understandable. Close relations are more likely to be empathetic, maintain confidentiality and less likely to stigmatize. They are also prime sources of psychosocial and practical support as shown by this study. This preference for close family members especially sisters is consistent with findings in previous works.15,16 Not disclosing to family members had negative impact on adherence to the no breastfeeding option in this study as two mothers bowed to family pressure to breastfeed. A Ugandan study showed that women who succeeded with replacement feeding had family support.17 The disclosure to pastors is perhaps because of perceived need for spiritual intervention for an incurable disease. Clergy men are assuming increasing role in the psychosocial support of HIV positive persons.18 The positive impact of spiritual support has been documented in previous studies.19,20 Although adverse reactions to disclosure was reported in a minority of the mothers studied, the fear of family disruption and even divorce/ end of relationship may continue to be a barrier to disclosure. Such fears have been reported in other studies.14 This may be more compelling if the situation is further compounded by serodiscordance with the male partner being seronegative to HIV. There have been reports on HIV serodiscordant couples in which the male partner is negative.21 This situation provides a basis for the partner to press for separation or divorce, on the grounds of infidelity. This negative response to disclosure has been reported in a previous study.15 The fear of disclosure may infact be an impediment to choosing the option of replacement feeding since the support of the partner has been identified as being important for successful replacement feeding. Continued counselling before and after disclosure may help ameliorate the situation. The finding of significantly younger mothers being separated from their partners is worrying. These younger mothers who are still active and mobile, may spread the illness as they may seek for more stable relationships and being often left with the care of the children, the need to support the family may lead to prostitution as a means of livelihood. Although HIV infected mothers are constantly encouraged to disclose their serostatus to their partners, the reluctance to do so by a third of the mothers raises some moral and ethical issues. The needs to prevent HIV infection of the possible HIV negative partner and the ethical responsibility of the managing healthcare team to both partners’ wishes are difficult issues in the management of HIV. Extended family pressure on mothers to breastfeed theirs babies was identified as reason for recommencing breastfeeding in most of the mothers who had earlier decided not to breastfeed. Extended family concern though noted to be prevalent and helpful in most African settings,22 may constitute a barrier to no breastfeeding option in HIV positive mothers. Breastfeeding is the norm in the study locale. The perceived deviation from the breastfeeding norm may also have led to most (77.33%) mothers being questioned about not breastfeeding their babies. Not only are questions potentially embarrassing, but they may constitute a barrier to adherence with the no breastfeeding option. In one study from Tanzania, a mother picked up her baby and breastfed just to show her friends that she was actually breastfeeding when indeed she had opted not to. In the present study, mothers gave socially, medically and culturally acceptable reasons for not breastfeeding. Culturally, giving token breastfeeding to pacify a crying infant especially in public is the expected behavior. The HIV positive mothers would have been under great pressure to do that. The moral support created by the partners may have encouraged the majority of mothers in this study to resist the pressure to give token breastmilk in public. The effect of token breastfeeding on possible mother to child transmission of HIV needs to be evaluated. Majority of the mothers expressed various kinds of negative feeling about not breastfeeding their infants. Similar feelings were reported in a study from Tanzania. The expression of such feelings indicates the emotional and psychological strain in the infant feeding choice. This underscores the need for continuing psychologic and emotional support of women who opt not to breastfeed. The preference for and reasons why all the mothers in the study opted for no breastfeeding options was discussed in our previous publication.12 Conclusion Mothers who disclosed their HIV serostatus to family members especially husbands/ partners received both moral and financial support in most cases. They also seemed better able to adhere to the no breastfeeding option in the supportive atmosphere created by family members. The expected compliance with the community norm of breastfeeding babies by nursing mothers and pressure from extended family to do so constitute barriers to adhering to no breastfeeding by HIV positive mothers. As part of infant feeding counselling, women should be empowered to cope with questions and pressures in culturally and socially acceptable ways. It is also important that more support be offered to infected mothers who opt not to breastfeed to enable them have better self esteem and to prevent negative feeling from not breastfeeding. It is recommended that HIV positive mothers should be encouraged to disclose their serostatus to close family members especially their spouses, having been counselled, to elicit support. Perhaps caution should be exercised when young mothers are involved. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09004t3.jpg] [rh09004t2.jpg] [rh09004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}