 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
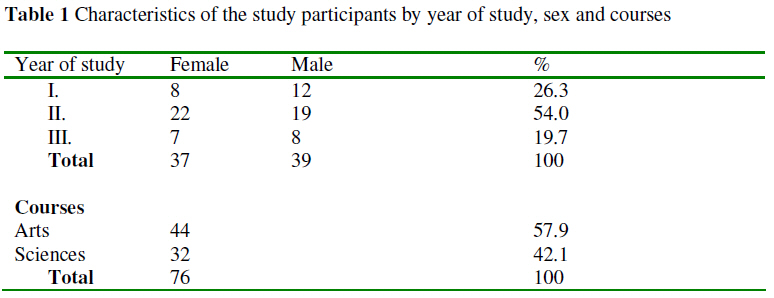
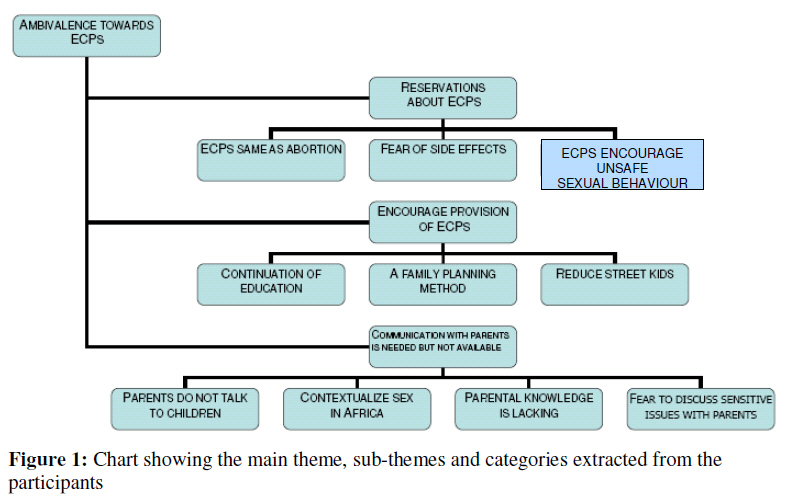
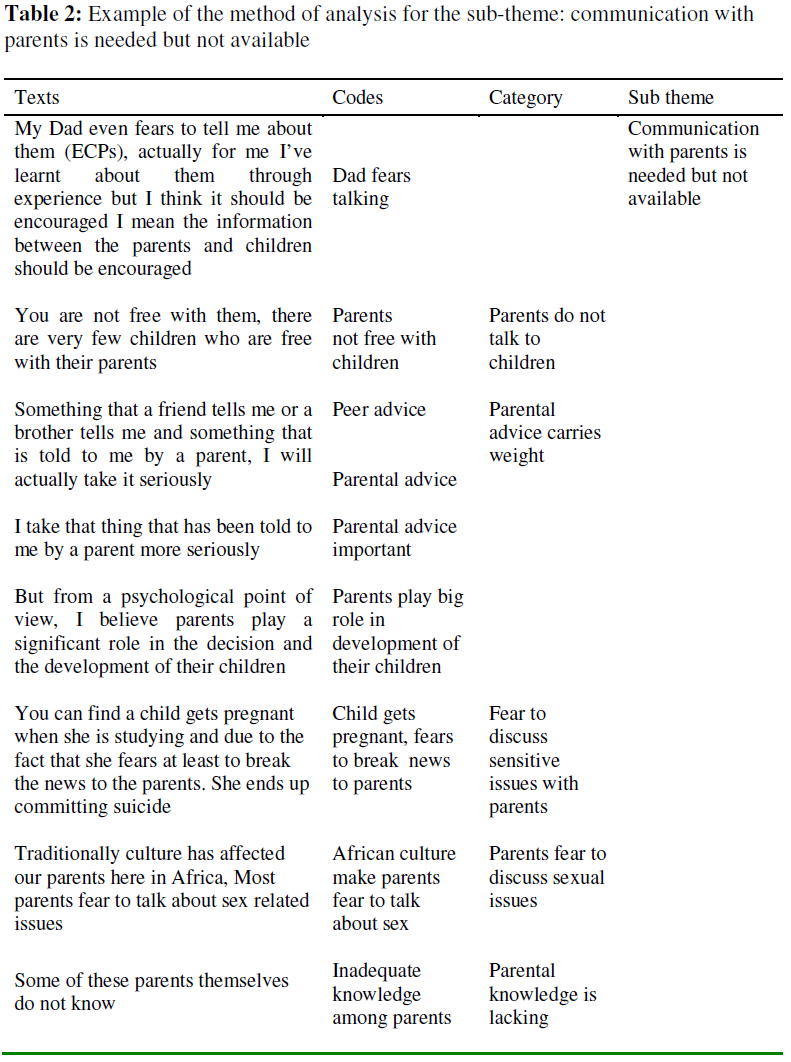
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 47-59 Original Research Article Faced with a Double-Edged Risk: Ugandan University Students’ Perception of the Emergency Contraceptive Pill in Uganda Face à un risque à double tranchant : La perception des étudiants ougandais de la pilule contraceptive d’urgenceJosaphat K Byamugisha¹, ³ Florence M Mirembe¹, Kristina Gemzell-Danielsson² and Elisabeth Faxelid³ ¹Makerere University Faculty of Medicine, Dept of Obstetrics and Gynecology; ²Karolinska Institutet, Dept. of Woman and Child Health, Division of Obstetrics and Gynecology; ³Karolinska Institutet, Dept. of Public Health Sciences, Division of International Health (IHCAR). Code Number: rh09006 ABSTRACT Whereas in high-income countries potential users of Emergency Contraception (EC) have information and access to emergency contraceptive pills (ECPs), it has remained secretive in low-income countries like Uganda. Although several studies have been conducted in relation to EC, few have addressed users’ perceptions. The objective of our study was to explore perceptions of EC by university students in Kampala, Uganda. Seven focus group discussions and four key informant interviews were conducted at Makerere University, Kampala. The transcribed data was analyzed for content and recurrent themes. Participants expressed ambivalence about ECPs. The method was generally recommended but only to the “right people”, in this context being those aged eighteen years and more. There were reservations surrounding provision of ECPs like similarity with abortion and fear of side effects. Users’ and potential-users’ perceptions are crucial in the accessibility and utilization of ECPs (Afr J Reprod Health 2009; 13[1]:47-59). RĖSUMĖ Alors que dans les pays à hauts revenus les utilisateurs potentiels de la contraception d’urgence (CU) sont renseignés et ont accès aux pilules du contraceptif d’urgence (PCU) dans les pays à faibles revenus tel que l’Ouganda, elle est restée un secret. Bien que plusieurs études aient été faites sur la CU, très peu de ces études se sont occupées des perceptions des usagers. Notre étude avait pour but d’explorer les perceptions de CU par les étudiants universitaires à Kampala, Ouganda. Sept discussions à groupe cible et quatre interviews par des principaux informateurs ont été menées à l’Université de Makerere, Kampala. Les données transcrites ont été analysées pour déterminer le contenu et les thèmes récurrents. Les participants ont exprimé des idées ambivalentes à l’égard des PCU. La méthode a été recommandée en général, mais seulement aux gens appropriés, dans ce contexte, il s’agit des gens âgés d’au moins dix-huit ans. Ils ont émis des réserves sur la provision des PCU telle sa similarité avec l’avortement et la crainte des effets secondaires. Les perceptions des usages et des usagers potentiels sont cruciales à l’égard de l’accessibilité et l’utilisation des PCU (Afr J Reprod Health 2009; 13[1]:47-59). KEYWORDS: Emergency contraception, Focus group discussions, University students, Uganda Introduction Emergency contraception (EC) is used after coitus but before pregnancy occurs. 1 For centuries, women have used a variety of devices and preparations to prevent pregnancy. Emergency contraception was once labeled “the best kept secret”. 2 Various names have been used including “post coital contraception” and “morning after treatment”. Other terms, restricted to the pill like the “morning after pill” and “after sex pill” have also been used but these terms can cause confusion regarding timing and purpose. For example some people interpreted the “morning after pill” literally and thus delayed an opportunity to use the method. Therefore it has been proposed that these names should be avoided. 3 The effectiveness of EC ranges from 75-99 percent depending on the method used and the interval between sexual intercourse and commencement of the EC method. Current evidence suggests that the levonorgestrel-only pill is the most effective of the available hormonal methods of EC and also has less side effects than the other hormonal methods. 3 Emergency contraceptive pills are not abortifacients. If a woman is pregnant, the pills will not have an effect on the pregnancy. Furthermore, ECs are not effective as a regular form of contraception. Therefore, these methods are only recommended as back up for occasional use. 4 According to the Uganda demographic Health Survey (UDHS), knowledge of any contraceptive method was 96 percent for all women and 98 percent for all men. The overall contraceptive prevalence rate was 23 percent. The unmarried sexually active women aged 15-49 had a higher level of use of modern methods than married women (38 % vs. 14%). The UDHS further indicated that EC was hardly known, probably because it had just been introduced at the time of the survey. Young peoples’ knowledge and perceptions were not specifically addressed. 5 Each year, an estimated 297,000 induced abortions are performed in Uganda, and nearly 85,000 women are treated for complications. Abortions occur at a rate of 54 per 1,000 women aged 15-49 and account for one in five pregnancies.6 On international women’s day (March 8th 2001), the EC pill was introduced in Uganda by a publication in the prominent Government newspaper. There was a full page of officials’ signatures endorsing the introduction of the EC pill containing levonorgestrel.7 It was followed by a number of protest letters from religious leaders and other members of the public in the press in the month of April 2001.8 They protested because they thought that an abortion pill was being brought in a country where abortion was restricted. Anecdotal evidence indicates that selling of the pill stalled thereafter. No studies about the potential users’ and the providers´ perspectives were done prior to the introduction. In the last three years, however, the selling of the pill has again increased in the pharmacies and clinics. The maternal mortality ratio (MMR) in Uganda is very high and stands at 505/100,000 live births5 . A study carried out in 1992-1993 in three Kampala hospitals found that 21 percent of maternal deaths were due to abortion related complications. 6 Of these deaths the majority were young women. It is hoped that through promotion of EC the number of unwanted pregnancies and thus the MMR can be reduced. According to the guidelines for introduction and use of ECs, the potential users’ views should always be considered. This qualitative study was, therefore, undertaken to explore the perceptions of EC by university students, who could be considered an important potential user group. Materials and Methods This exploratory qualitative study was carried out among Makerere University students in Kampala, Uganda between January and April 2005. During this time about 30,000 students were registered at the University. The students came from all parts of the country and a few came from the neighboring countries. These students resided in ten halls and each hall had a secretary (minister) for health. The study participants were purposively selected to provide a diversity of characteristics including age, sex, courses, year of study and district of origin (Table 1). A study conducted between January and march 2005 in the same population had revealed that mean age of the participants was 21 years. Less than half (45.1%) had ever heard about emergency contraceptive pills (ECPs).The most common sources of information about EC were friends (34%),media (24.8%) and schools (19.4%), .The ever pregnancy rate was 2.6, 3.4 percent and 42 percent were in a steady relationship of three or more months. The contraceptive ever-use rate was 14.5 percent. Among the users the most common contraceptive methods ever used were condoms (48.9%) and withdrawal (23.4%) Data collection Seven focus group discussions (FGDs) were conducted. A FGD is defined as a carefully planned discussion designed to obtain perceptions on a defined area of interest in a permissive non-threatening environment10 . Two of the FGDs comprised of males only, two were girls only and three were a mixture of both boys and girls. For each there were 9-12 participants. The only information participants received before the discussion was that they were to discuss issues related with reproductive health. Three FGDs were conducted in the common rooms of halls of residence; one in the garden at the Institute of Languages and the rest were conducted at the freedom square within the university campus. A trained moderator and a note taker conducted the FGDs using a FGD guide. The duration of the FGDs ranged from 50-90 minutes. The content was based on results from research done about EC among students9 . and the guide was pilot tested on a group of students in order to have a better idea about the flow and clarity of the questions. Thereafter the guide was slightly revised. The guide covered the following areas; methods of contraception available in Uganda, understanding of EC, mechanism of action, efficacy, time limit after unprotected intercourse, side effects, availability of ECs, menstrual cycle and discussion of EC with parents. The FGDs were carried out until there was information saturation and that is why a total of seven was done. All FGDs were tape recorded. The FGDs were transcribed verbatim. University students’ perception of the ECP In addition to the FGDs, four key informant (KI) interviews were conducted. A key informant is a member of the social or cultural group in the research context who provides information and assistance with interpretation of the setting. The key informants in this study were thus purposefully selected and included the Guild president (students’ overall leader), an interior secretary and two secretaries for health of halls of residence. Three of the key informants were interviewed at their halls of residence. One preferred to be interviewed in the city centre. Three of the interviews were tape-recorded. One KI did not want the interview to be tape-recorded. For the latter, notes were made during the interview and we relied on this for analysis. The recorded interviews were transcribed verbatim. Method of analysis The data was analyzed by content analysis. What is referred to as manifest content analysis deals with the visible and obvious components. In contrast, analysis of what the text talks about deals with the relationship aspect and involves an interpretation of the underlying meaning of the text, referred to as the latent content11 . The latter method was used in this study. After reading through each transcript several times, the answers to the various questions included in the FGD guide were extracted, put together and constituted the unit of analysis. The condensed meaning units were abstracted and labeled with a code as discussed by Graneheim and Lundman12 outlined in Figure 1 and Table 2. Initial coding was done and numerous codes generated. Special vocabulary that the respondents used was noted. The codes were then focused to eliminate less useful ones. Repeating ideas and large themes that connected the codes were identified. The data relevant to each category was identified and examined using a process called constant comparison, which means that each item was checked and compared with the rest of the data. The latter were added to include as many of the nuances as possible. Ethical clearance was obtained from Makerere University higher degrees research committee and the ethics research committee at Karolinska University Hospital, Stockholm, Sweden. Written informed consent was obtained from each participant. Results The main theme that emerged was ambivalence towards ECPs. The subthemes were: reservations about ECPs, encourage provision of ECPs and communication with parents needed but not available. There were several categories under each sub-theme (Figure 1). Ambivalence towards EC In many of the discussions the participants showed mixed reactions about EC. They would on one hand encourage use and on the other hand hesitate on full scale use as illustrated in the following quote:
Ambivalence towards EC was reflected throughout the results, not only in the categories but also in the sub-themes. Encouraging use of ECPs was usually followed by nuances of hesitation. As young people they are faced with the temptation to have sex and this would subject them to the risk of unwanted pregnancy as well as sexually transmitted infections (STIs) including HIV. The participants indicated that induced abortions were taking place among students and at times with fatal consequences. This was a reason for availing contraceptives not only to save lives but also to assist students to continue their education. The categories were externally heterogeneous (different) but internally homogeneous and shadows of mixed reactions could still be seen in the texts. Encouraging provision of EC was surrounded by reservations about the methods used and how ECPs act. The data also indicate the ambivalence in relation to communication with parents. On the one hand, parents´ advice was considered very important and valuable but on the other hand parents were said to fear communication with their children about EC. Encouraging provision of ECPs was thus sandwiched by reservations about EC for example the risk of encouraging unsafe sexual behavior and by the lack of communication with parents. Reservations about ECPs There were reservations about ECPs mainly related to the participants´ views that ECP was similar to abortion, the participant’s fear of side effects, and their views that there was a risk that ECPs might encourage unsafe sexual behavior. Many of the participants were not certain about when exactly ECs should be used. They had different views of how EC pills work to prevent pregnancy. Some of the responses centered on inhibiting implantation as in the following example:
Other participants believed that ECP is similar to abortion as shown in the following quote:
Local herbs used as abortifacients were mentioned and included Ruhoko (Phytolacca dodecandra family phytolacca-ceae) and Mururuza (vernonia amygalina family Asteraceae). These are taken orally in liquid form. Abortion was mentioned as something dangerous and hence some participants thought EC a better alternative. Fear of side effects were commonly mentioned in the FGDs, ranging from immediate ones like feeling weak to long term effects such as infertility later in life or if there was conception the risk of delivering an abnormal baby as indicated below.
The A (abstinence), B (being faithful) and C (condom use) strategy for HIV prevention was re-echoed either wholly or in parts during the discussions. The participants thus feared that the availability of ECs could encourage promiscuous behavior and reduce the use of condoms, which would then increase HIV transmission.
Furthermore, in most FGDs and also among the KIs it was mentioned that students are more worried about pregnancy than HIV/AIDS and other STIs.
It was felt that ECPs which only prevent pregnancy may increase the risk of STIs. Encourage provision of ECPs It was a general view that ECPs should be provided because they have a number of advantages. But the participants were skeptical about the availability of EC pill over the counter because of fear of misuse and side effects. Both the KIs and the FGD participants reiterated that EC should be given to the “right” people. The issue of age 18 years and above was re-echoed. The participants were aware that young people have sex but that this is due to “moral decay”. They discussed that adolescents before the consent age are not yet “ready” to have sex as in the following quote
However, some participants said that ECP should be viewed as any other type of contraceptive method and that the provision of ECP was good since young people could then continue their education. Furthermore, it was highlighted that some male students, who impregnate fellow students or women in the slums, leave their offspring, who then become street children. Providing ECP could thus be a way of reducing unwanted children, who are not looked after properly. Communication with parents needed but not available Parents were mentioned as an occasional source of ECs and this was followed further to find out whether the participants actually discuss EC with their parents. In most of the FGDs it was mentioned that in the African context it is difficult for parents to discuss issues concerning sex and contraception with their children. Parents do not talk to children as indicated in the following quote.
Fear to discuss sensitive issues with parents was highlighted and was at times detrimental.
It was considered important to look at parental communication about sex in the African context where sex is considered something secret. Parents were also said to lack knowledge about sexual and reproductive health issues. Although some parents were said to act as commanders instilling fear into their children, many participants said that the parents should talk to their children because a child is likely to accept and follow parental advice. The participants who had discussed EC and other sex related issues with their parents were happy and recommended it for others. Discussion The participants in the FGDs were active, jovial and everybody contributed to the discussion. The open ended format of the questions allowed participants to bring in new issues and that’s how the ABC strategy kept coming up in various ways. Including the interviews with the KIs in the study ensured method and data triangulation. The participants encouraged availability and provision of ECPs especially to the right people. The right people were taken as those older than eighteen years. In Uganda the consent age is eighteen years and anybody above this age can be independent in both decisions and actions including those about sex. In a study done to understand contraceptive use, the results showed that the EC users were more positive, perceived greater support from their partner for EC use, rated themselves more at risk of pregnancy, and felt more confident about asking for EC than non users13 . In our study, participants indicated that abortions were occurring and had grave consequences. Some studies have indicated that about 40 percent of women who go for induced abortion have had one or more abortions previously14 . Emergency contraception utilization can potentially reduce unwanted pregnancies and thus the risks related to unsafe abortions. Some of the respondents thought that EC was the same as abortion. They indicated that the pills were destroying something in the woman’s body not necessarily in utero. The perception of something being destroyed within one’s body shows the complexity that surrounds EC in this study population. This has been reported in other studies and can have a negative impact on the use. Since friends are some of the sources of information, the negative effect can have multiple implications15 . There were considerable concerns that availing ECs would promote irresponsible sexual behavior and thus increase sexually transmitted infections including HIV/AIDS. The major reason given was that the women in particular are concerned with the risk of unwanted pregnancy rather than with HIV infection. They would thus use ECPs but not condoms and thus be at risk of contracting STIs. However, studies done elsewhere have not shown increased risk when EC is supplied in advance 16, 17 compared to when it is provided as need arises. It would thus be good to provide EC with other sexual and reproductive health services. At the time of the study there had been a lot of debate going on in Uganda about the ABC strategy and its impact on reduction of HIV/AIDS infection. (18, 19) It was discussed that if ECPs were made available it means a leeway is being allowed for sex, since some of the participants are more worried about pregnancy than STIs. However, interventions have indicated that even in the era of AIDS concurrently talking about condoms, abstinence and EC will not increase risky behavior. (20) The participants agreed that in reality many people have sex and thus need protection from both pregnancy and STIs including HIV/AIDS. It is important to note that the Uganda Government is currently implementing the presidential initiative on AIDS strategy for communication to youth (PIASCY)21 and this is mainly about abstinence and health related issues. Thus a sector wide approach would be needed in scaling up availability and utilization of ECPs. In this study no fears were discussed about failure to use regular methods of contraception if EC became more available, which has been in some other studies. 21, 22 This could be due to the fact that the percentage of the contraceptive users is low in this group (15%) and most of the methods used were condoms and withdrawal9 . However, previous studies have not shown decreased use of regular contraceptives when ECP use and access have increased. 23, 24 Participants expressed concern over the side effects. The major worry was about side effects related to infertility in the future and risks of teratogenicity. Fertility is very important in Uganda hence this is a point to address when counseling clients about EC and should be included in the relevant information education communication (IEC) materials. This concern has been shown in other studies done in the East African region25 . Our study indicates that there is need for EC counseling services for young women and their partners. Much as the final decision is for the woman, the male partners need to get involved in the whole process since after all they were involved in the sexual act. This necessity has been expressed in other studies26-28 . Faced with the risk of pregnancy and infections if they engage in sex, young people should have reliable information to turn to. This is where parents would come in as a useful and trusted source. However, the relationship between parents and their children seems to be of master and subject rather than parent and son/daughter. African culture encourages children to respect their parental advice and this is passed on from generation to generation. Young children who do not respect their parents are usually not accepted by the local communities. Conclusions It is very important to consider the societal and cultural context at the time of introduction and scaling up provision emergency contraceptives. The users’ and potential-users’ perspectives are crucial in EC method utilization. Parents should be equipped so that they can enhance the life skills of young people. Acknowledgements The authors would like to thank the students and student leaders who accepted to participate in the focus group discussions and the interviews. We acknowledge the transcription skills of Ivan and John Michael and Department of Botany Makerere University. The study was supported by grants from Sida/SAREC and from the Swedish research council. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09006t1.jpg] [rh09006t2.jpg] [rh09006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}