 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
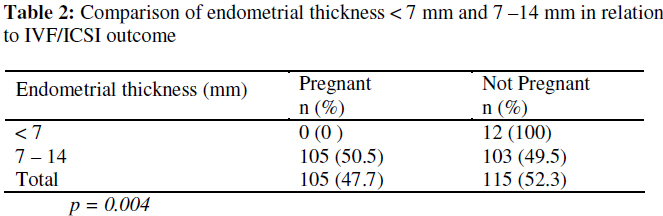
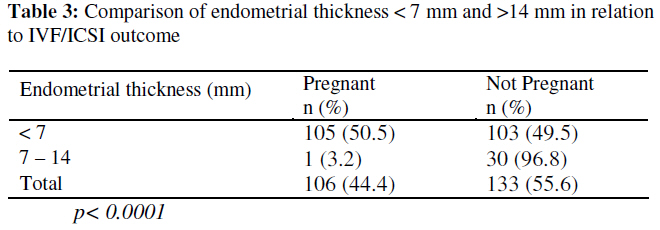
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 113-121 Original Research Article The Effect of Endometrial Thickness on In vitro Fertilization (IVF)-Embryo Transfer/Intracytoplasmic Sperm Injection (ICSI) Outcome L’effet de l’épaisseur endomètre sur la fécondation in vitro (FIV) le transfert de l’embryon/le résultat de l’injection intracytoplasmique du sperme.Okohue JE1,2, Onuh SO1,2, Ebeigbe P3, Shaibu I1,2, Wada I1,2, Ikimalo JI4 and Okpere EE5 1 Nordica Fertility Centre @ Nisa Premier Hospital, Jabi Abuja; 2 PortHarcourt Fertility Centre, PortHarcourt Rivers State; 3 Department of Obstetrics and Gynaecology, College of Health Sciences, Delta State University, Abraka; 4 Department of Obstetrics and Gynaecology, University of PortHarcourt Teaching Hospital, Rivers State; 5 University of Benin Teaching Hospital, Benin city, Edo State. Code Number: rh09010 ABSTRACT The value of measuring the endometrial thickness and studying the endometrial receptivity in the context of assisted conception remains a contentious issue. A prospective analysis was carried out to determine the effect of endometrial thickness on IVF -embryo transfer / ICSI outcome in dedicated Assisted Reproductive Technology (ART) units in Abuja and Rivers State, Nigeria. Two hundred and fifty one patients who met the inclusion criteria were analysed. They were grouped on the basis of endometrial thickness into 3 groups; <7 mm, 7 – 14 mm and >14 mm. The main outcome measure was clinical pregnancy. There were significantly more pregnancies in the 7 – 14 mm endometrial thickness group compared to the <7 mm and >14mm groups, p=0.004 and p<0.0001 respectively. The findings suggest that following IVF/ICSI, significantly more pregnancies occurred when the endometrial thickness was between 7 and 14 mm (Afr J Reprod Health 2009; 13[1]:113-121). RĖSUMĖ La valeur obtenue quand on mesure l’épaisseur d’endomètre et quand on étudie la réceptivité d’endomètre dans le contexte d’une conception assistée reste un problème controversé. Une analyse prospective a été menée pour déterminer l’effet de l’épaisseur d’endomètre sur la FIV-le transfert de l’embryon/IIS dans les centres de la Technologie de la Reproduction Assistée à Abuja et dans l’état de Rivers, au Nigéria. Deux cent cinquante patientes qui ont satisfait les critères d’inclusion ont été analysées. Elles ont été regroupées selon l’épaisseur d’endomètre en trois groupes : < 7mm, 7-14mm et > 14mm. Le résultat de la mesure le plus important était la grossesses parmi le groupe de < 7mm et > 14mm, p=0,004 et p<0,0001 respectivement. Les résultats indiquent qu’à travers la FIV/IIS, ils se produisaient de manière significative, plus de grossesses quand l’épaisseur d’endomètre était entre 7 et 14mm (Afr J Reprod Health 2009; 13[1]: 113121). KEYWORDS: Endometrial thickness, IVF/ICSI, Pregnancy Introduction The endometrium is the inner lining of the uterus and has receptors for gonadotrophins and ovarian hormones. In response to estradiol from the ovaries (or exogenously) the endometrial lining grows in a typical pattern which is recognizable by transvaginal ultrasound scan. During the menstrual cycle, the endometrium undergoes cyclic proliferative and secretory changes in preparation for implantation1 . The endometrial growth has been found to be at the rate of 0.5 mm/day in the proliferative phase and 0.1mm/day in the luteal phase2 . The endometrial thickness on transvaginal scan is usually taken as the maximum distance between the echogenic interfaces of the myometrium and the endometrium measured in a plane through the central longitudinal axis of the uterus2 . Implantation is the most crucial stage in the establishment of pregnancy3 .It is defined as a process by which the embryo attaches to the uterine wall and first penetrates the epithelium and then circulatory system of the mother to form the placenta.4,5 Throughout the menstrual cycle, changes take place that prepare the endometrium for implantation. The value of measuring the endometrial thickness and studying the endometrial receptivity in the context of assisted conception remains a contentious issue6-9 . In one study, the authors reported that endometrial thickness on the day before oocyte recovery was significantly greater in pregnant than in non pregnant women and suggested that it may predict the likelihood of implantation10 . Another retrospective analysis studied the impact of endometrial thickness on the day of embryo transfer on in vitro fertilization (IVF) outcome. It found that increased endometrial thickness was significantly associated with higher pregnancy rates1 . This finding supported those of Yakin et al.11 In a more recent study, clinical pregnancy was found to be positively associated with increased endometrial thickness and peak estradiol concentrations in serum and negatively associated with advanced age.12 Using leuprolide acetate with Human Menopausal gonadotrophin (hMG) for ovarian stimulation, Sher et al13 also described a positive outcome between a thicker immature endometrium with a matured grade as opposed to a thinner immature endometrium. A more recent Turkish study concluded that endometrial thickness of at least 6.5 mm correlated with a higher rate of conception14 while no pregnancy occurred in a similar study when the endometrial thickness was less than 6mm15 . Bergh et al16 concluded that an endometrium of at least 9 mm before oocyte retrieval was required for pregnancy, while Oliveira et al17 put the cut off at 7 mm. On the other hand, several researchers found that measurement of endometrial thickness had no predictive value for pregnancy18-20 . Eichler et al21 failed to relate endometrial thickness or grade with outcome using either clomiphene citrate with hMG or gonadotrophin releasing hormone agonist and hMG. One study prospectively evaluated the predictive value for pregnancy of the endometrial thickness and pattern assessed by vaginal ultrasonography on the day of human chorionic gonadotrophin (hCG) injections and the day of embryo transfer in 74 stimulated cycles for IVF. The presence of a ‘poor quality’ endometrial pattern on the day of hCG administration, while associated with lower pregnancy rates compared to those with ‘good quality’ endometrial pattern, was not statistically significant.22 Another prospective study found that endometrial growth and its pattern transformation during the stimulation did not influence the pregnancy outcome. 23 Weissman et al24 in their retrospective analysis found that patients with endometrial thickness greater than 14mm on the day of hCG administration, had significantly reduced implantation and pregnancy rates with an increase in the rates of miscarriage contrary to a more recent report25 . Yaman et al26 also concluded that sonographic measurement of endometrial thickness on the day of hCG treatment is not useful in predicting IVF outcome. Although De Geyter et al27 had adviced against cancellation of treatment cycles for the simple reason of inadequate endometrial thickness, treatment cycles have been known to be abandoned for the above reason with the attendant losses to the patients. This study therefore aims to evaluate whether or not there exist a relationship between endometrial thickness and pregnancy rates in an African population. This becomes relevant considering other studies, which have shown some differences in the response to ovarian stimulation and complication rates between an African population (Yorubas) and their Caucasian counterparts.28 Methods A prospective analysis of pregnancy rates in women undergoing IVF/ICSI between May 2005 and April 2006 at Nordica Fertility Centre, a dedicated IVF centre in Abuja Nigeria and its subsidiary in Rivers State, Nigeria was carried out. An average of 60 and 15 cycles per month are carried out at the Abuja and Rivers State centres respectively. Ovarian stimulation was achieved using the standard long protocol, of pituitary desensitization with GnRH-a followed by administration of hMG. Endometrial thickness was measured with a Transvaginal scan on the day of hCG administration, 36 hours before oocyte retrieval. Measurement was taken as the maximum distance between the echogenic interfaces of the myometrium and the endometrium measured in a plane through the central longitudinal axis of the uterus. All measurements were done by the same physician. Embryos were transferred after 48 hours. Pregnancy tests were done 15 days after embryo transfer. Transvaginal ultrasound scans were done three weeks after a positive pregnancy test. The uterine ultrasonographic scoring system by Baruffi et al29 was used to grade the endometrial thickness. Cycle parameters were compared between pregnant and non pregnant patients. Exclusion criteria included women who were above 35 years of age and those using donor eggs. Those with abnormal FSH, LH and Prolactin levels were also excluded. Main outcome measures were endometrial thickness and clinical pregnancy. Results obtained were recorded on a data collection sheet designed for the study. The coded data was then fed into the computer using Epi Info programme and analysed. Observed differences were evaluated for statistical significance using the Chi square test and the Fisher’s exact test. Level of significance was set at p < 0.05. Results Overall, 298 patients met the inclusion criteria during the study period. Fourteen patients had their treatment cycles cancelled due to poor follicular response to stimulation with GnRHa. Two patients were found to be pregnant on day 14 of down regulation following transvaginal ultrasound scan. Two patients had no oocyte retrieved from any of their developing ‘follicles’. Three patients had no embryo transfer carried out as there was failure to fertilize following incubation for IVF. One patient had no embryo transfer as no spermatozoon was extracted following Percutaneous Epididymal Sperm Aspiration (PESA), Testicular Sperm Aspiration (TESA) and Testicular Sperm Extraction (TESE) on the day of ovum pick up. Twenty one patients had biochemical pregnancies while 4 had ectopic pregnancies. They were all excluded from the study leaving a total of 251 patients that were subsequently analysed. The age range of the patients in this study was 20 – 35 years. There was no statistically significant difference in the age of the patients, between the pregnant and the non pregnant groups: 30.22 years (±3.97) and 30.84 years (±2.79) respectively (p=0.1475). One hundred and sixty eight patients (66.9%) had male factor infertility while 73 patients (29.1%) had female factor infertility. Forty patients (15.9%) had unexplained infertility. Overall clinical pregnancy rate was 42.2%. Table 1 shows that there was no statistically significant difference between the pregnant and non pregnant groups, when age, duration of infertility, number of oocytes retrieved and embryos transferred were analysed; p = 0.1475, p = 0.5224, p = 0.5032 and p = 0.16 respectively. Also, the endometrial thickness values between the pregnant and non pregnant women were 11.82 mm (±1.90) and 11.88 mm (±3.17) respectively. This difference was not statistically significant (p = 0.85221). In Table 2, the pregnancy rate in women with endometrial thickness <7 mm was compared with that in women with endometrial thickness 7 – 14mm. No pregnancy occurred at <7 mm (0%) while 105 pregnancies (50.5%) occurred in the 7 – 14 mm group. This difference was statistically significant (p = 0.004). Furthermore, as shown in Table 3, the pregnancy rate in women with endome-trial thickness 7 – 14 mm was compared with the rate in those with thickness >14 mm. The rates were 50.5% and 3.2% respectively and was statistically significant (p<0.0001). Discussion Technology with IVF and embryo transfer has improved over the years and most IVF centres report far higher pregnancy rates than 10years ago when the first cases recording endometrial thickness and echo pattern at the time of hCG injection were documented.31 There was no statistically significant difference in the age of the patients, between the pregnant and the non pregnant groups (p=0.1475). Yaman et al26 had found the age of non pregnant women to be significantly higher than in the pregnant group. However unlike in our study, no upper age limit was set for their patients. Overall 66.9% of all cases had male factor as the sole cause or as a contributor to the infertility. Studies have suggested that male factor accounts for between 20 and 50% of the causes of infertility in different parts of Nigeria.32,33 It will be difficult to comment on the contribution of the female partners to infertility in this study. This is because the centre usually starts its investigation of the infertile couple with a seminal fluid analysis. This generally will determine the extent to which the female partner is investigated. Cases in which there is mild oligozoospermia, result in the female partner having the full complement of investigations including a tubal patency test to determine the suitability or otherwise for intrauterine insemination (IUI). Those with severe oligozoospermia or azoospermia do not usually have a tubal patency test done, except where this had been done previously before presentation. Notwithstanding however, 29.1% of the patients had female factor as a sole cause or as a contributor to the infertility and as expected all were tubal in origin. 15.9% of the cases had unexplained infertility. It is known that about 5 – 15% of adult couples in African countries have unexplained infertility.34 Overall, endometrial thickness ranged between 5.6 mm and 21mm. The average endometrial thickness in the pregnant and non pregnant groups was 11.82 mm (±1.90) and 11.88 mm (±3.17) respectively. This was not statistically different (p = 0.8521). No pregnancy occurred in the 12 patients who had endometrial thickness below 7mm. When this was compared to the 50.5% pregnancy rate in the 7 – 14 mm group, it was statistically significant (p=0.004). This finding is consistent with that of Oliviera et al17 where no pregnancy was found in patients with endometrial thickness less than 7mm. The number of patients in this group was rather small as many patients (14 or 53.8%) had their treatment cycles cancelled for poor follicular response. This finding would suggest that follicular response could determine endometrial thickness. However, Okonofua et al35 in their study concluded that serum estradiol showed a better positive correlation with endometrial thickness than with total number of developing follicles. They also showed that estradiol value per follicle and estradiol/progesterone ratio both weakly correlated respectively with endometrial thickness. Patients who had endometrial thickness between 7 – 14 mm had 105 (50.5%) pregnancies. This was significantly greater than the 1 (3.2%) pregnancy in the group of patients with endometrial thickness greater than 14mm (p < 0.0001). Previous studies in support of a role for endometrial thickness in determining pregnancy outcome concluded that “increased endometrial thickness was significantly associated with higher pregnancy rates”.1,10-12 Other studies which did not show a stastistically significant difference in endometrial thickness between pregnant and non pregnant patients had equally concluded that measuring endometrial thickness on the day of hCG injection had “no predictive value for conception in IVF/ICSI cycles” 18-20 or “not useful in predicting IVF outcome”.26 From our study even though there was no statistically significant difference in the endometrial thickness between those who achieved pregnancy and those who did not, we found that a critical endometrial thickness has to be attained for pregnancy to occur.14-17 . Similar to Weissman24 ,we found that patients with endometrial thickness greater than 14 mm on the day of hCG administration had significantly reduced chances of conception (p<0.0001). The above findings have important clinical implications. On the day of hCG administration, less than 7mm or greater than 14mm from our study would mean reduced chances of pregnancy occurring in that treatment cycle. Some studies have shown that there is no statistically significant difference in pregnancy rate following single or double embryo transfer.36,37 A case could therefore be made for either transferring one embryo and freezing the others when such “unfavourable” endometrial thickness is encountered or totally avoiding any transfer during that cycle and freezing all the embryos. Later embryo transfer could be done preferably using a natural cycle, for this age group, to avoid the discomfort of repeated injections during another attempt at down regulation. This is practicable as there are reports that pregnancy and live birth rates following natural cycle frozen embryo transfer and a down regulated cycle frozen embryo transfer in regularly menstruating women are statistically the same.38 This is more so considering studies done by Wada et al which showed that birth characteristics of babies conceived from cryopreserved/thawed embryos were similar to those from fresh embryos with significantly fewer congenital malformations in the cryopreserved group. 39 In conclusion while there was no statistically significant difference in the endometrial thickness between pregnant and non pregnant patients following IVF/ICSI, pregnancy would likely not occur in patients with endometrial thickness less than 7 mm. Significantly less pregnancies are likely to occur in those with endometrial thickness greater than 14 mm. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09010t3.jpg] [rh09010t1.jpg] [rh09010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}