 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
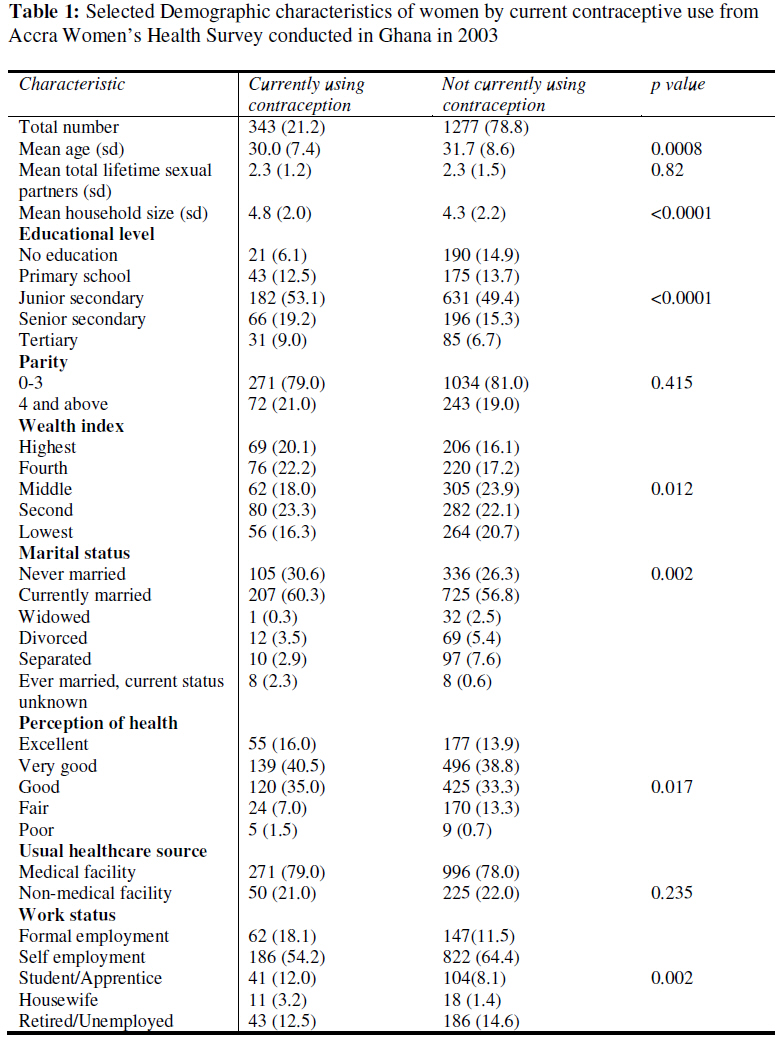
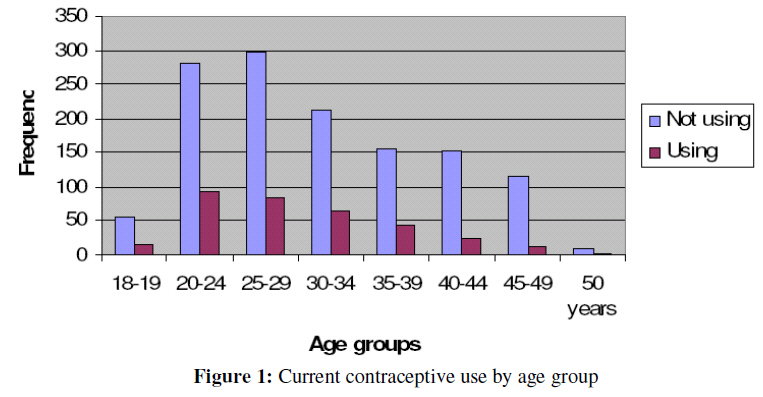
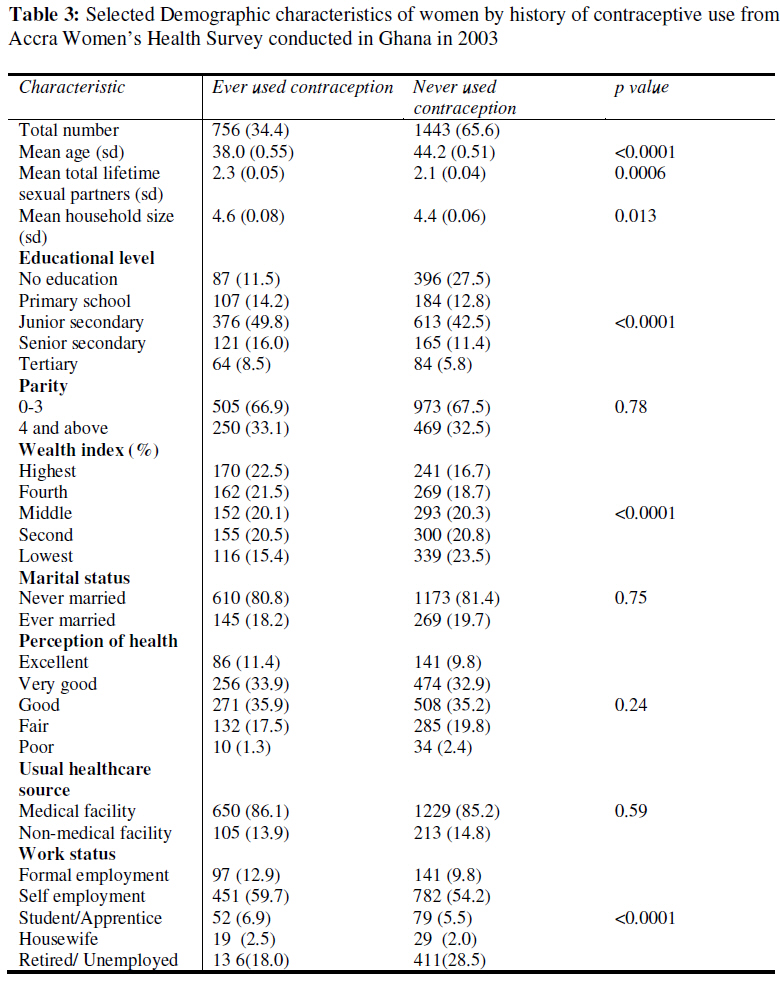
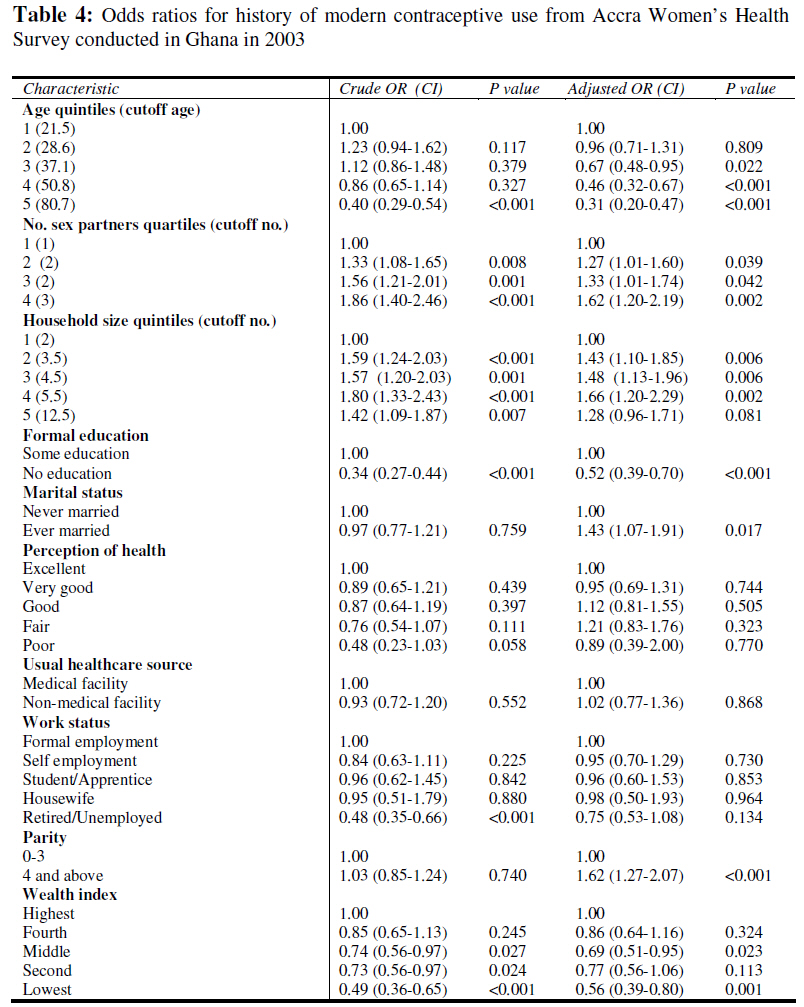
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 123-133 Original Research Article Contraceptive Use by Women in Accra, Ghana: Results from the 2003 Accra Women’s Health Survey L’emploi des contraceptifs par les femmes à Accra, Ghana : Résultats recueillis de l’enquête menée en 2003 sur la santé des femmes d’AccraRichard MK Adanu1, Joseph D Seffah2, Allan G Hill2, Rudolph Darko3, Rosemary B Duda4 and John K Anarfi5 1 Department of Obstetrics and Gynaecology, University of Ghana Medical School, Accra, Ghana; Code Number: rh09011 ABSTRACT The study was to determine the predictors of use of modern contraception among women in Accra, Ghana. Data were collected by trained interviewers using questionnaires. Complete data for 2199 women were analysed using Stata 8.2. The study showed that educational status was the most significant predictor of contraceptive use. Women with no formal education had a 48% reduction in the odds of having ever used contraception and a 66% reduction in the odds of currently using contraception. Regular use of health facilities did not affect contraceptive use. Female education should continue to be a priority of the Ghanaian government. Education about family planning and the effects of having large families should be integrated into the school curriculum. Ghanaian health workers need to be active in promoting the use of modern contraceptive methods (Afr J Reprod Health 2009; 13[1]:123-133). RĖSUMĖ L’étude avait pour objectif, de déterminer les indices de l’emploi de la contraception moderne chez les femmes à Accra, Ghana. Des données ont été collectées par des enquêteurs professionnels à l’aide des questionnaires. Les données compréhensives pour 2199 femmes ont été analysées à l’aide du state 8,2. L’étude a montré que le niveau de l’éducation acquis constitue l’indice le plus important de l’emploi du contraceptif. Les femmes qui n’ont pas acquis une éducation formelle avaient une réduction de 48% pour n’avoir jamais utilisé le contraceptif et une réduction de 66% s’agissant de l’emploi actuel de la contraception. Le fait de fréquenter les établissements de santé n’a pas affecté l’emploi du contraceptif. L’éducation de la femme devrait rester une priorité pour le gouvernement ghanéen. Il faut que l’éducation sur la planification familiale et les effets d’une famille nombreuse soient intégrés dans le programme scolaire. Il faut que le personnel de la santé soit actif dans la promotion de l’emploi des méthodes du contraceptif moderne (Afr J Reprod Health 2009; 13[1]: 123-133). KEYWORDS: Family planning, Modern contraception, Ghana, Africa Introduction Ghana is a developing country which, like many other developing countries, has a high fertility rate1 . The maternal mortality ratio in Ghana is high at 500 per 100,000 live births2 and one way of indirectly reducing this is to lower the fertility rate3 . Although the total fertility rate in Ghana is one of the lowest in sub Saharan Africa1 , the contraceptive prevalence rate of 20%1 is low when compared to the rate in North African countries like Tunisia 4;5 . Family planning has been an important area in the plan of the ministry of health in Ghana and many international organizations have been involved in promoting family planning in Ghana. Family planning in Ghana started as far back as 1956. The Planned Parenthood Association of Ghana was formed in 1967 and in 1970 the Ghana national family planning programme was launched. The programme is currently being managed by the Ghana Health Service with support from development partners. There have been studies that have investigated the determinants of modern contraceptive use in many different countries6-9 . Some of the factors that have been reported to promote the use of modern contraceptive methods are formal education, high socio-economic status and easy access to family planning services 6;10-12 . Identified barriers to contraceptive use include religious and social restrictions, low socio-economic status and lack of formal education11 . Accra, the capital city in Ghana has the highest reported contraceptive prevalence rate in the country1 . Access to family planning services in Accra is reported to be good1 and there is a lot of public advertisement of modern contraceptive methods. Women in Accra have different educational and socioeconomic levels. The extent to which these play a role in the urban setting of Accra with relatively easy access and the highly subsidized costs, which exist throughout Ghana, has not been extensively researched. This knowledge would be helpful in designing effective programs to improve the contraceptive prevalence rate in Accra and the rest of Ghana as well. The aim of this study is to determine the major demographic predictors of the use of modern contraceptive methods among women in Accra. Methods Study design The Women’s Health Study of Accra was a population-based cross-sectional survey that was conducted in 2003. Using the data from the Ghana 2000 census, the 1731 enumeration areas in Accra were stratified by socio-economic status and 200 were selected with probability proportional to population size within the socio-economic strata. Each household in the selected strata was visited in order to compile a list of women aged 18 and older who were usually resident in the household. A random sample of 17 women per enumeration area was selected for the survey. A total of 3183 women were interviewed at home, with a questionnaire, by trained interviewers between March and September 2003. The interview included questions on demographic characteristics, lifestyle habits, living conditions, general health and reproductive health. The analysis of contraceptive use was restricted to the 2835 women in the sample who were sexually experienced. Of these 2199 (77.6%) had complete data on contraceptive use and the demographic factors that were investigated as possible predictors of contraceptive use. Statistical analysis Contraceptive use was analyzed at two levels. The first level of analysis looked at the predictors of having a history of ever using a modern method of contraception and the second examined the predictors of current use of a modern method. Respondents were classified as either users or non-users at both levels of analysis. Analysis of history of contraceptive use was performed using the whole sample. However the analysis of current contraceptive use excluded women who were above 50. The independent variables that were investigated in this analysis were age, educational status, socio-economic status, ethnicity, religious affiliation, household size, total number of lifetime sexual partners, use of medical facilities for regular healthcare, self-assessment of health status, occupation and parity. Visit to a medical facility or pharmacy within the past year were additional variables that were used in determining the predictors of current contraceptive use. Scatterplot matrices13 were used to visualize how the variables of interest varied across the different levels of contraceptive use. Log linear graphs13 were used to explore how continuous variables varied with contraceptive use in order to decide whether to model these variables as discrete levels on a continuous scale or as quintiles. Contraceptive users and non-users were compared with regard to demographic characteristics. The chi square test and the two tailed t test13 were used to assess differences across the groups. Simple logistic regression13 was used to obtain unadjusted odds ratios of contraceptive use for each variable. Multiple logistic regression13 was then used to obtain adjusted odds ratios. Interaction between educational status and each of the following: socioeconomic status, quintiles of age, quintiles of number of lifetime sexual partners and quintiles of number of people living in the household were assessed using multiple logistic regression 13 . Likelihood ratio tests13 were used to compare models with interaction terms to models without interaction terms. Analysis was performed using Stata 8.214 . A p value of <0.05 was considered to be significant in each of the statistical tests that were performed. Results The mean age of the 2199 respondents was 42.1 years (sd 18.2). The age range was from 18.0 to 102.0 years. Current use of modern contraception Women who were currently using contraception lived in larger households and were significantly younger than those not using contraception (Table 1). The educational status of current users of modern contraception was significantly higher that that of the women who were not using contraception (Table 1). Stratifying the respondents by current contraceptive use also showed significant differences between users and non users in wealth index, marital status, perception of health status and work status (Table 1). Multiple regression for current use (Table 2) showed a significant reduction in the odds of using contraception above age 45. Figure 1 shows that contraceptive prevalence is highest among women between the ages of 20 and 29. The odds of using contraception were increased by over 100% for women living in households of more than 5 people compared to those living in households of 2 or lower although increasing parity did not show a significant increase in the odds. Lack of formal education reduced the odds of using modern contraception by 66%. Women who were selfemployed were significantly less likely to be using contraception compared to those in formal employment. Women who had never used contraception were more likely to have had no formal education compared to those who had a history of contraceptive use (Table 1). The differences in parity, marital status and perception of health status were however not significant when respondents were stratified on history of contraceptive use (Table 2). Women with a history of contraceptive use had a significantly higher number of lifetime sexual partners. History of modern contraceptive use Tables 3 and 4 show the results from the analysis of history modern contraceptive use. Figure 2 also shows how the history of contraceptive use varies with age. Women who had used modern contraception before were significantly younger and better educated than those who had never used contraception. There were also significant differences in both groups in terms of household size, socioeconomic status and number of lifetime sexual partners (Table 3). Educational status was a significant predictor of a history of ever using contraception. Women with no formal education had a 48% (OR:0.52 CI:0.39-0.70) reduction in the odds of having ever used contraception. In addition to educational status, household size and age, marital status, parity and lifetime number of sexual partners were significant predictors of a history of contraceptive use. Interaction terms were added to the multiple regression model to test for interactions between educational status and each of the following variables: age, wealth index, lifetime number of sexual partners and household size. There was no significant interaction in either the model for current contraceptive use or that for history of contraception use. Discussion These results show that educational status is the most significant predictor of a woman currently using contraception in Accra. Educational status was also a significant predictor of a woman having a history of past contraceptive use. This finding is in agreement with other studies 6;11 that have highlighted the importance of female education in promoting the use of family planning methods. This study looked at the use of modern contraceptive methods and a prevalence rate of 21.2% was obtained. This figure is comparable with the rate of 26% reported in the 2003 Ghana Demographic and Health Survey for use of modern methods.1 Although women of the middle wealth index quintile were significantly less likely to use contraception than women in the highest quintile, there was no consistent trend in contraceptive use by differing wealth index quintiles. There was also no significant difference in contraceptive use by the different socioeconomic residential strata. Use of contraception has been shown to increase with increasing socio-economic status12 . It is possible that the effect of socioeconomic status on contraceptive use is not obvious in Accra because it is the urban center of Ghana and access to family planning services in Accra is uniform across social strata. The cost of contraceptive methods is highly subsidized in Ghana, as in many other developing countries, and this could further explain the absence of a significant difference in contraceptive use across the different socio-economic groups. Religious affiliation and cultural norms have been cited as factors that negatively affect the use of contraception 11;15 . Among women in Accra, contraceptive use was not significantly affected by religious affiliation or ethnicity. This observation is probably due to the fact that the urban influence of Accra leads women to be able to make decisions, regarding family planning, which are not strongly influenced by religion or culture. Women with a high number of lifetime sexual partners were more likely to have a history of contraceptive use but not significantly more likely to be current users. It is recommended that women with multiple sexual partners use a barrier method of contraception such as the condom16 . Although having a high number of lifetime sexual partners does not mean that a woman has current multiple sexual partners, there is possibly a high correlation between number of current partners and number of lifetime partners. Considering the threat of HIV infection, this finding raises concern about women’s risks of acquiring sexually transmitted infections in Accra. An interesting finding was that although high parity did not significantly increased the likelihood of a woman using contraception, a high number of household members did. It is possible that living in a large household makes people more aware of the social consequences of large families. Another possibility is that living in a large household increases the opportunity for women to get information about family planning. The effect of formal employment on contraceptive use is shown by the finding that women who have their own businesses (self-employed) are less likely to use contraception. This could be due to the fact that such women are not affected by maternity leave restrictions and can also more easily combine childcare with work. Self-employed women may therefore be less concerned about fertility regulation. A limitation of this study is that the reasons women have for not using contraception in Accra was not investigated. Analyzing these reasons would be very helpful in designing targeted programs to increase contraceptive use. Based on the study findings, it is recommended that female education should continue to be a priority of the Ghanaian government and education about family planning and the effects of having large families be integrated into the school curriculum. Ghanaian health workers need to be active in promoting the use of modern contraceptive methods. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09011t2.jpg] [rh09011t1.jpg] [rh09011f1.jpg] [rh09011t4.jpg] [rh09011t3.jpg] [rh09011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}