 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
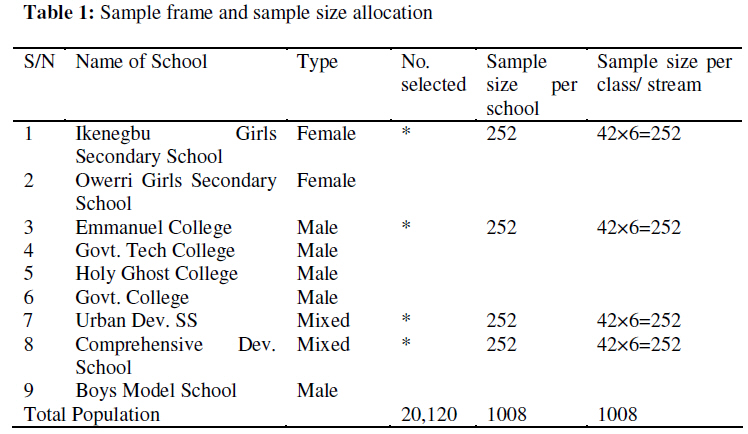
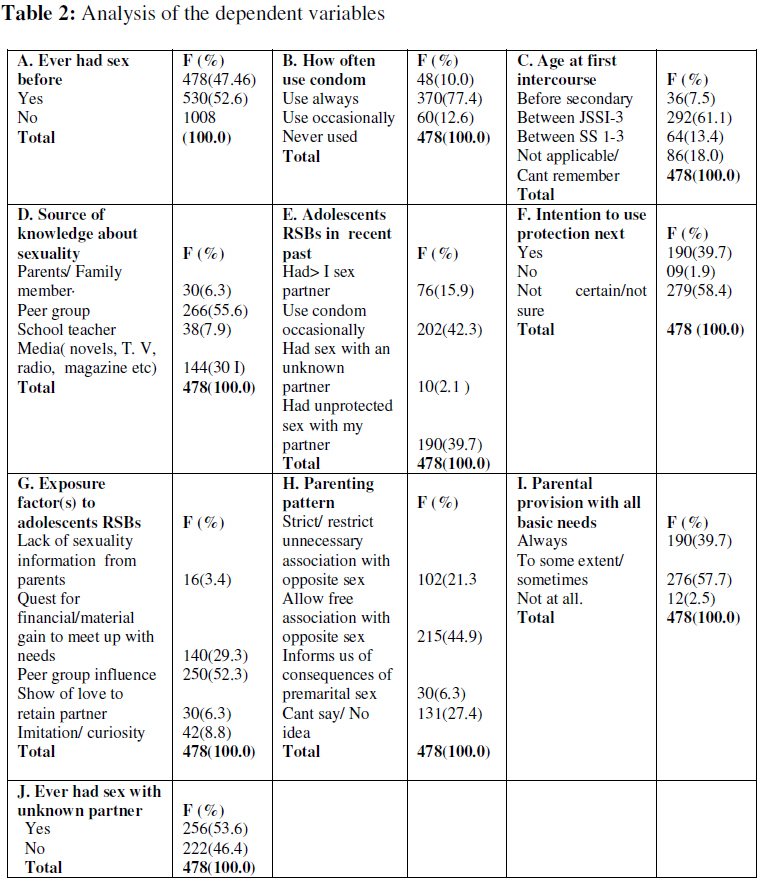
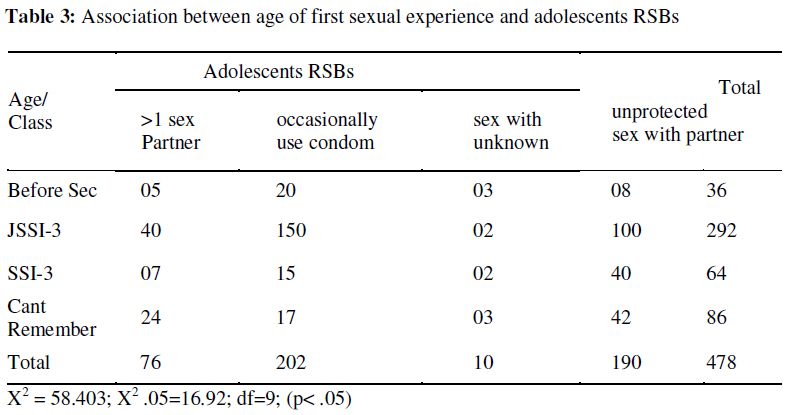
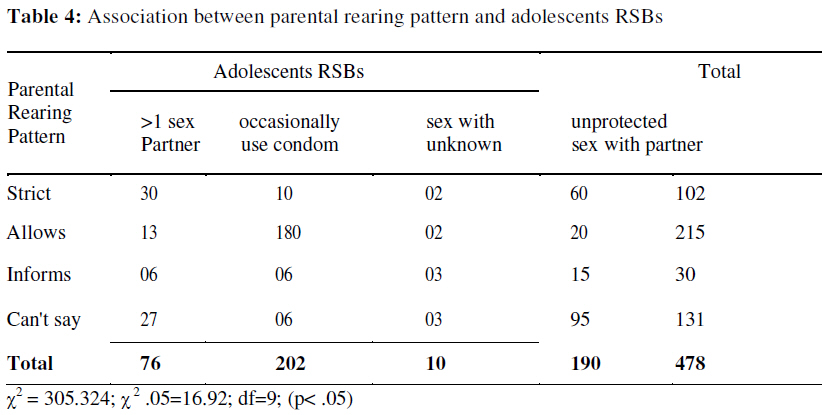
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 135-145 Original Research Article Risky Sexual Behaviours among Adolescents in Owerri Municipal: Predictors of Unmet Family Health Needs Les comportements sexuels dangereux chez les adolescents dans la ville municipale d’Owerri: Les indices des besoins sanitaires familiaux non satisfaits Benjamin O. Nwankwo* and Eunice A. Nwoke Department of Public Health Technology, School of Health Technology, Federal University of Technology, PMB 1526, Owerri, Imo State, Nigeria Code Number: rh09012 ABSTRACT This study examined the risky sexual behaviours (RSBs) of adolescents in Owerri Municipal in Imo State. Adopting the descriptive Survey research design, a stratified sampling technique was used to enroll 1008 adolescents aged 10 – 19 from 4 secondary schools into the study. A structured questionnaire was used for data collection. Result shown that majority of the adolescent (47.4%) have had sex and many have engaged in one form of RSBs or another. Peer group seem to be major source of the sexuality information (55.6%) and influencing factor (52.3%) .Significant association was found to exist between adolescents RSBs and age at first sexual experience or adolescent perception of parental rearing pattern (p<. 05). The study challenged the stake holders involved in the inculcation of values, curriculum design or policy formulation to provide appropriate, time sensitive and scientifically sound sexuality information for adolescents (Afr J Reprod Health 2009; 13[1]:135-145). RĖSUMĖ Cette étude a examine les comportements sexuels dangereux (CSD) chez les adolescents à Owerri, ville municipale de l’état d’Imo. En adoptant le modèle de recherche fondé sur l’enquête descriptive, nous avons instruit 1008 adolescents âgés de 10 a 19 ans dans 4 écoles secondaires à l’aide d’une technique d’échantillon stratifié. Pour collecter les données, nous nous sommes servis d’un questionnaire structuré. Les résultats ont montré que la plupart des adolescents (47,4%) ont eu des rapports sexuels et se sont engagés à une forme du CSD ou une autre. Le groupe de pairs semble être la source principale de l’information sexuelle (55,6%) ainsi que le facteur influant (52,3%). On a trouvé qu’il existe un lien important entre les CSD des adolescents et l’âgé de l’expérience sexuelle initiale ou la perception de l’adolescent de la manière dont les parents élèvent leurs enfants (< p > .05). L’étude a défi tous ceux qui sont impliqués dans l’inculcation des valeurs, la conception des programmes scolaires, ou bien la formulation de la politique qui puisse assurer aux adolescents l’information de la sexualité qui est appropriée, sensible au temps et scientifiquement solide. (Afr J Reprod Health 2009; 13[1]:135-145). KEYWORDS: Adolescents, Risky Sexual behavior (RSB), Predictor, Unmet needs, Health, Family, Municipality, Owerri, Nigeria Introduction Adolescence (age 10-19) is defined as a transitional stage of life during which individual reach sexual maturity1 . As a growing concern globally, the reproductive health needs of the adolescents centering on sex and human sexuality have been largely ignored 2 Studies3 confirmed that nearly half of the higher school students (9th -12th graders) have had sexual intercourse and over 60% reported having had sex by the time they graduated. Rates of pre marital sexual activity have been found to be higher in urban than in rural areas4 . The same pattern is true of some sub-Saharan Africa and Asian countries (5,6,2) . This demonstrates as in many other countries, that many adolescents are confronted at some point during their teen years with choices about whether or not to have sex, and if they do, whether or not to use condoms and or other contraceptives more so as complete sexual control of the teens by parents, elders or educators have proved almost impossible7 . As most acts of premarital sexual intercourse are unprotected or coerced2 sexually active adolescents due to gender power imbalances are increasingly at risk of unwanted pregnancy, abortion or contracting and transmitting sexually transmitted diseases (STDs), including HIV/AIDS. A recent study2 in India and Nepal had suggested that a high knowledge about contraception does not always translate into a higher level of contraceptive use. Again, even when adolescent girls know about contraceptives, they are much less likely to be using them than older women, indicating a large unmet need for contraceptives among adolescents8 Many factors have been attributed to risky sexual behaviors (RSBs) among adolescents. They include inadequate access to correct information; the limited availability of and access to youth. friendly health services; peer pressure and the erosion of the role of family as the source of information and advice on sex-related matters; economic constraints and; the gender power disparity 9,10, 11 . UNESCAP9 opined that while parents are perceived to be the logical source of information, they often do not discuss sexuality issues with their children because they are embarrassed by the subject. This is also true with health care providers12 . Again resource constraints affect the ability to buy contraceptives or seek medical services leading to youth involvement in sexual relationships for economic gain from persons perceived to be in a position to provide economic remuneration 11,13,14 or leading many adolescent girls scrambling, "perpetually" to be in the race of being "main girl friend", "hope for marriage" or face rejection. Consequences of adolescent pregnancy, childbirth or the threat of diseases resulting from risky sexual behaviors (RSBs) have significant effects on family health in general and by extension maternal and child health. Children born to adolescent mothers are likely to be premature or have a low birth weight (LBW), injured at birth or stillborn, or associated with delivery complications resulting in higher mortality 15, 16, 17 . The pregnancies may also compel them to drop out of school, be rejected by family, face harder economic conditions and contribute to perpetuating the circle of poverty 2,18 . From the foregoing, it is evident that the sexual and reproductive health needs of adolescents have emerged as an issue of great concern especially in the sub-Saharan Africa, where family morals and values have seriously been eroded, poverty deeply rooted, access to affordable health care grossly inadequate and. education and training not tailored and targeted at populations needing them 11 . These assumptions7 predict highly unmet family health needs among these teens. To this end, the study sought specifically to answer the following research objectives: ascertain adolescent sexual experience status and age at first sexual intercourse; major sources of information about sexuality; assess the sexual behavior of the adolescents considered risky; their knowledge of consequences of the risky sexual behavior; factors encouraging this behavior; the adolescents' intention to future preventive behavior and the association or relationship between adolescents risky sexual behavior and either age/class when started or adolescents parenting style. Methods The descriptive survey design was considered appropriate for a baseline study of this nature. The setting for this study is Owerri Municipal in lmo State. Owerri Municipal has all the characteristics and features of an urban life. The area is bounded proximally on all sides by Owerri North LGA. The population of the study was made up of approximately 20,120 adolescents aged 10-19 years located in 9 Government Secondary Schools in Owerri Municipal. As adolescent RSBs in this area are not well documented in the literature, therefore it was assumed to be 50%. With a 95% confidence interval, a baseline sample size for the study was calculated 19 yielding a minimum sample size of 808 which was reviewed upwards to accommodate sampling error. A total of 1008 adolescents participated in this study. These adolescents were randomly selected from 4 schools out of the total schools population frame. The schools were first stratified into 3(Government male, Government female and Government mixed), from where the random selection was done. In each school, a total of 252 adolescents were randomly selected from all the classes (JSS I-SS3), giving an average of 42 adolescents per class. In each class or level, the number of streams (a-n) and class list were obtained while potentates were polled using the systematic kth case (see Table 1). A self constructed questionnaire made up of 13 items, which were centered on the objectives of the study formed the major instrument for the study. The instrument passed through peer review and back translation to ensure validity. It was later pre tested in a secondary school in Owerri North LGA, which shared similar geo-social characteristics with Owerri Municipal. A reliability co-efficient index of r = 0.68 was achieved in both pre and post tests. With approval from school principals, the instrument was administered to the potentates before the start of days mid break period. The adolescents were assured of the anonymity of their responses as their names were not solicited. This is in accordance with guidelines of the authors’ institution, as the study was reviewed and approved by the research protocol committee of the Federal University of Technology Owerri. Three research assistants were recruited for the instrument administration which lasted two weeks. Data analysis was initially manually tallied while level of significance was set at a.05 for the two formulated hypotheses. Results and Discussion Out of the 1008 male and female adolescents enrolled into the study, only 478 representing 47.46% of respondents were considered eligible to be used for further analysis as they agreed through the questionnaire to have had sexual intercourse before. The remaining 530 (52.6%) of the respondents said they have never had sexual intercourse before. Out of the 478 (47.4%) who agreed to have ever had sex (Table 2), majority 302(63.2%) have had it more than four times in the last six months, many 106 (22.2%) said more than 3 times, some 54(11.3%) mentioned one to two times while few 16 (3.4%) said more than 5 times. On how many sex partners they have, a nearly balanced number in each case 210 (43.9%) and 204 (42.7%), mentioned more than three partners and a single sex partner respectively. A few 256 (53.6%) said yes while many 222 64 (13.4%) mentioned between 2-3 sex (46.4%) said they have not tried it. partners. Adolescents were asked their When asked frequency of condom likelihood of ever having sex with an use, majority 370 (77.4%) said they use it unknown partner. Interestingly, majority occasionally, some 60 (12.6%) never used it while only few 48 (10.0%) said they always use it thereby concluding that adolescents in this part of the globe have been involved in premarital and RSBs. Studies in other sub-Saharan African and Asian countries 5,6,2 , demonstrates that many adolescents are confronted at some point during their teen years with choices about whether or not to have sex, and if they do, whether or not to use condoms and/or other contraceptives. On age at first sexual intercourse or experience, majority 292 (61.1 %) have had sex when they were in the junior (JSS 1-3) class, many 86 (18.0%) however said they couldn't remember, some 64 (13.4%) had the experience in their senior secondary class (SSI-3), while few 36 (7.5%) had it when they were still in primary school. This findings also corroborates what the CDC ,3 had earlier confirmed that nearly half of higher school students (9th -12th graders) have had sexual intercourse and over 60% reported having had sex by the time they graduate. Again rates of pre marital sexual activity among adolescents were found to be higher in urban than in rural areas4 . It was important to document how these adolescents sourced sexuality information. Concerning this trend, majority 266 (55.6%) implicated their peer groups, many 144 (30.1%) got their information from the media comprising magazines, novels, radio, television etc. Only 38 (7.9%) of the adolescents mentioned their school teachers while a small number 30 (6.3%) mentioned either parents or older adults at home. This result showed a widening and disturbing gap in accessing sexuality information (Peers Versus Parents). This is so because while parents are perceived to be the logical source of information, they often do not discuss sexuality issues with their children because they are embarrassed by the subject. As a result, the family is no longer the prime reference group in reproductive health related decisions, since teenagers tend to value the opinions of their friends more highly9 . Again, adolescents were probed to ascertain the type of sexual behaviors they have recently engaged in which could be adjudged "risky". They were requested to select the best option from the list (Table 2). In response to this, majority 202 (42.3%) occasionally use condom, many 190 (39.7%) have had unprotected sex with their main partners, some 76 (15%) have had more than one sex partner while few 10 (2.1 %) have had sex with an unknown partner in the recent past. The lesson drawn here is that most adolescents in this study engage in one RSB or another and that a high knowledge about contraception does not always translate into a higher level of contraceptive use as a recent study in India and Nepal suggested2 . On whether they know the consequences of RSBs, all respondents 478 (100.0%) agreed to all the options listed such as STD/ HIV/ AIDs, Unwanted pregnancy leading to drop out from school, Parental abandonment and Abortion which may lead to death. This is in sharp contrast to other findings that, ascertained that sexually experienced adolescents are typically unaware of the consequences of unprotected sexual intercourse and are also poorly informed of their sexuality and means of protecting themselves, often leading to unwanted pregnancy and abortion. As a follow up, respondents were probed to ascertain their readiness and intention to engage in protected sex in future. Unfortunately majority 279 (58.4%) were either uncertain or not sure whether they will engage in protected sex next time. Many 190 (39.7%) however said they will, while a small but important number 9 (1.9%) were certain they will not consider using any form of protection during future sexual contact. The Trans theoretical Model (TTM)20 provides us with an in-depth understanding of not why people change but how (called Stages of change). They concluded that current intentions may be proxy indicators of future behavior. On factors likely to have been responsible for exposing the adolescents to RSBs, here again (referring to the result of major source of sexuality information), majority 250 (52.3%) of the respondents mentioned peer group. Quest for financial and material gain to meet up with needs was mentioned by many respondents 140 (29.3%) as responsible for exposing the adolescents to RSBs. Insignificant few respondents mentioned either imitation/ curiosity 42 (8.8%), show of love to retain partner 30 (6.3%) or lack of sexuality information from parents 16 (3.4%). Peer pressure influence among adolescents 9,10,11 increases where there is little or no traditional parental care. The adolescents were further asked to judge their parents rearing patterns seen either from the angle of freedom given to the adolescents or the parent’s provision of adolescent’s basic needs. On freedom, most respondents 215 (44.9%) said their parents allowed them freedom of association with opposite sex, many 131 (27%) could not say anything. 102 (21.3%) of the respondents however, said their parents were strict and restrict unnecessary association with the opposite sex. Few respondents 30 (6.3%), claimed their parents informed them of the consequences of premarital sex. On the provision of need, majority of the adolescents 276 (57.7%) said their parents provided all their basic needs only sometimes or to an extent, many 190 (39%) said they were provided for always, while few 12 (2.5%) said their parents did not provide at all. Where some parents do not restrict their children’s association with the opposite sex and few parents provide their children with sexuality information, it merely confirms 9,10,11 the erosion of traditional parental control. Again parents inability to provide their wards with their basic needs consequently 14,11,13 , leads the vulnerable adolescents to involvement in sexual relationships for economic gain from persons perceived to be in a position to provide economic remuneration in exchange for sex. As seen in Table 3, a null hypothesis stating that an association does not exist between adolescents RSBs and the age of first sexual intercourse or experience was advanced. The table revealed that majority of respondents who had their first sexual experience at the JSS 1-3 class also used condom occasionally or even had unprotected sex with main partner. Subjecting the hypothesis to a chi squared (χ2) test showed that χ2 54.403 > χ2.05=16.92 (df = 9). The hypothesis was rejected leading to the conclusion that a significant association exit between adolescents RSBs and the age of first sexual intercourse or experience (p < .05). As earlier reviewed (3) nearly half of higher school students (9th -12th graders) have had sexual intercourse and over 60% report having had sex by the time they graduate while the rates of pre marital sexual activity among adolescents(4) have been found to be higher in urban than in rural areas In Table 4, another null hypothesis stating that an association does not exist between adolescents RSBs and their parental rearing pattern was put forward. Here again, we observed that majority (180) of those whose parents allowed freedom of movement and association with opposite sex occasionally used condoms indicating a high RSB. Conversely, adolescents who claimed parents were strict or restricted unnecessary association with opposite sex; majority (60) had unprotected sex with their main partners, while many (30) have had more than one sex partner. Studies7 had confirmed that the complete sexual control of the teens by parents, elders or educators have proved almost impossible. The hypothesis was Subjected to a chi squared (χ2) test, which showed that χ2 305.324 > χ2.05=16.92 (df =9). The hypothesis was rejected leading to the conclusion that parental rearing pattern was significantly associated with the adolescents RSBs (p < .05). Conclusions Of the 1008 male and female adolescents enrolled into the study, a significant number have had sex before. Of those who agreed to have ever had sex, majority have had it more than four times in the last six months. Many have had more than one sex partner. While majority have had it with an unknown partner, many said they use condom occasionally. On future intention to use any form of protection, majority were uncertain. Majority started their sexual experience when they were in the junior (JSS 1-3) class. Many of the adolescents sampled implicated their peer groups as major source of sexuality information. Again, the adolescents in the study area have engaged in one form of RSB or the other. All the respondents agreed knowing the consequences of risky sexual behavior (RSB), such as STD/ HIV / AIDS, unwanted pregnancy leading to drop out from school, parental abandonment and abortion which may lead to death. On factors likely to have been responsible for exposing the adolescents to RSBs, majority of the respondents mentioned peer group. On adolescents perception of parents rearing pattern and provision of basic needs, most respondents said their parents allows them freedom of association with opposite sex, while majority of the adolescents said their parents provides all their basic needs only sometimes or to an extent. A significant association was found to exit between adolescents RSBs and the age at first sexual intercourse or experience or parental rearing pattern ( p < 0.05) . Recommendations Two important issues have emerged in this study. Firstly majority of the adolescents had engaged in one form of RSB or the other within the secondary school age and reviewed literature have confirmed that the complete sexual control of the teens by parents, elders or educators have proved almost impossible 7, it is therefore necessary to let parents including the significant others to know their primary responsibility as role models and being authoritatively assertive. Secondly, peer group was a major source of adolescent’s sexuality information, while peer group pressure was a major factor promoting adolescents RSBs. Here parents should be encouraged to moderate their wards’ companies and not shy away from maintaining a disciplinary standard. All stake holders such as educators, curriculum planners, counselors etc involved in the design of curriculum or policy formulation for this vulnerable group (the adolescents) , are challenged to provide through the curriculum appropriate, time-sensitive, scientifically sound and evidence -based sexuality information to the adolescents. Governments both at the Federal and state levels can sensor and place sanctions on media messages, which have the potential of misinforming the adolescents and youth’s sexual information. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09012t1.jpg] [rh09012t2.jpg] [rh09012t3.jpg] [rh09012t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}