 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
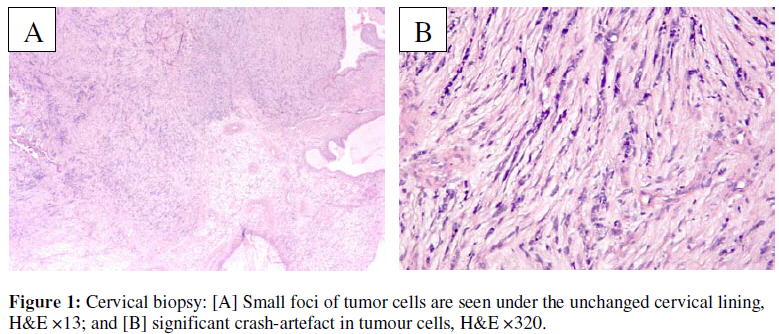
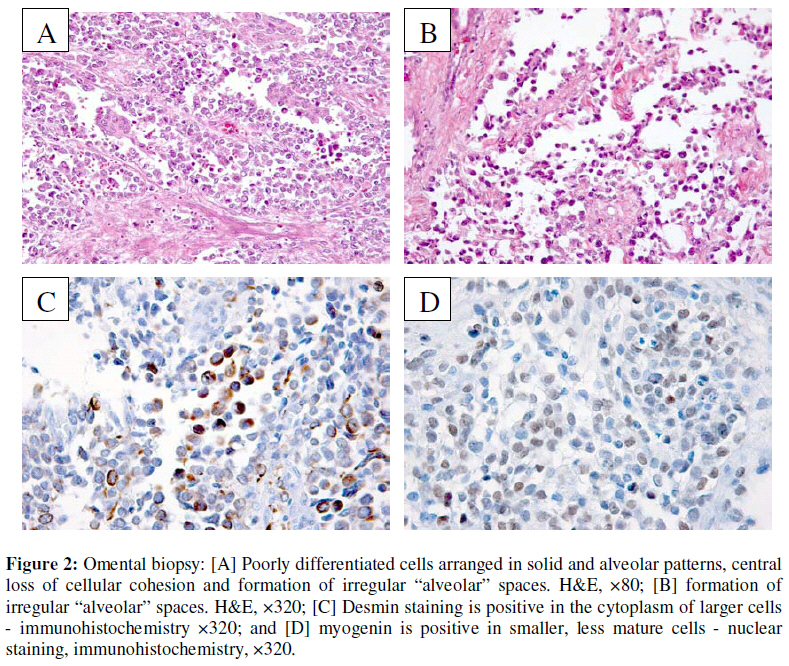
African Journal of Reproductive Health, Vol. 13, No. 1, March, 2009, pp. 167-173 Case Report Advanced Alveolar Rhabdomyosarcoma of the Uterus: A Case Report Le rhabdomysarcome de l’alvéolaire avancé de l’utérus.A.T. Odoi1, E.T. Dassah1, D.E. Darkey1, O. Owusu-Afriyie2 and A.Y. Valkov2 1 Department of Obstetrics and Gynaecology, Komfo Anokye Teaching Hospital, Kumasi, Ghana; Code Numbe: rh09015 ABSTRACT Alveolar rhabdomyosarcoma is an uncommon malignant soft tissue tumour rarely found in the female genital tract and carries a very poor prognosis especially in adults. A 44 year old premenopausal woman was evaluated for a lower abdominal mass, intermittent unprovoked vaginal bleeding and weight loss. Examination showed a huge abdomino-pelvic mass, and an irregular cauliflower mass protruding from the cervix, from which a biopsy was taken. Exploratory laparotomy revealed a widespread disseminated uterine tumour with an “omental cake” and involving virtually all the abdominal viscera. Debulking surgery was found to be non-beneficial and uterine and omental biopsies were taken. The cervical, uterine and omental biopsies were all diagnosed alveolar rhabdomyosarcoma. Neither chemotherapy nor radiotherapy could be started before the client died of fulminant neoplastic dissemination 17days postoperatively. While the optimal management of this rare tumour is unknown, early recognition and diagnosis, and a prompt multimodality treatment approach of surgery, chemotherapy and radiotherapy offers the best chance of cure (Afr J Reprod Health 2009; 13[1]:167-173). RĖSUMĖ Le rhabdomysarcome de l’alvéolaire est une tumeur de tissu mois malin rare qui n’est pas souvent trouvée dans la voie génitale féminine et porte un pronostique mauvais surtout chez les adultes. Une femme en préménopause qui est âgée de 44 ans a été évaluée pour la masse abdominale basse, l’hémoragie vaginale non provoquée et intermittente ainsi que pour la perte de poids. L’examen a montré une grande masse abdominal-pelvienne et une masse irrégulière du chou-fleur qui avance du col à partir de laquelle nous avons fait une biopsie. La laparotomie exploratoire a révelé une tumeur de l’utérin disséminée un peu partout avec un « gâteau epiploique « et touchant à peu près tous les viscères abdominal ». La chirurgie par morceaux n’a pas été salutaire et les biopsies de l’utérin et de l’épiploon ont été prises. Les biopsies du col, de l’utérin et de l’épiploon ont été diagnostiquées un rhabdomysarcome de l’alvéolaire. On n’a pas pu commencer la chimiothérapie ni la radiothérapie avant que la patiente soit mort de la dissémination néoplasique fulminante, 17 jours après l’opération chirurgicale. Alors qu’on ne connaît pas la meilleure conduite à tenir devant cette tumeur rare, si elle est reconnue et dignostoiquée tôt et si l’on adopte une approche chirurgicale fondée sur une multimodalité de traitement, la chimiothérapie et la radiothérapie offrent la meilleure chance de guérison (Afr J Reprod Health 2009; 13[1]:167-173). KEYWORDS: Advanced, Alveolar rhabdomyosarcoma, Uterus, Premenopausal Introduction Alveolar rhabdomyosarcoma of the soft tissue usually presents as a painless, non tender rapidly growing lump1 . Alveolar rhabdomyosarcoma typically occurs in adolescents and young adults1,2,3 . Of the childhood rhabdomyosarcomas, it has the worst prognosis4,5 with a very poor survival rate6 . All cervical sarcomas in adults are known to carry a very poor prognosis7,8 . The reported cases of rhabdomyosarcoma in adults have a poorer outcome compared with children9,10 . Alveolar rhabdomyosarcoma of the cervix is extremely rare and the first case was reported by Emerich et al. in 199611 . The patient was treated with radical surgery and postoperative radiotherapy but died 3 months after the surgery11 . Two other cases of alveolar rhabdomyosarcoma of the cervix12 and uterus13 in adults, which were diagnosed early and achieved complete remission following surgery, chemotherapy with and without radiotherapy respectively have been reported12,13. We report a case of alveolar rhabdomyosarcoma of the uterus that presented late, in order to draw the attention of practitioners in the sub region to an early recognition and discuss the current management options available for this rare tumour variety. Case Report A 44-year-old, para 6 premenopausal woman presented to a Ghanaian District Hospital with a lower abdominal mass of about 2 years duration and a 3-month history of intermittent unprovoked heavy vaginal bleeding and weight loss. Her last 2 deliveries were by Caesarean section, and the lower abdominal mass was noticed about 1 year after the last Caesarean section. An impression of a pelvic tumour (differential diagnosis of carcinoma of the endometrium or cervix) was formed and she was referred to our centre for further evaluation and management. Significant findings on our initial examination showed a cachectic woman with a distended abdomen and signs of free fluid (in the abdomen) and a huge firm abdomino-pelvic mass comparable to about 26 weeks gravid uterine size. The chest was clinically clear. Her baseline haematological investigations were normal. Examination under anaesthesia in theatre revealed a huge pelvic mass extending to both pelvic side walls and the abdomen. The cervix was firm and bled easily on contact, with an irregular cauliflower-like mass extending from the cervical canal. A biopsy of the cervical lesion was taken for histopathological diagnosis. Ultrasound examination revealed a markedly enlarged uterus with heterogeneous echo pattern, marked vascular flow patterns under Doppler study and moderate amount of fluid in the uterine cavity. The ovaries could not be identified separately; no clear adnexal masses were noted. The urinary bladder and both kidneys appeared normal. The spleen and liver were normal, with a lot of free fluid in the abdomen. Results of blood biochemistry, chest X-ray and electrocardiogram were unremarkable. Initial microscopic examination of the cervical biopsy showed unremarkable surface mucosa and infiltration of the underlying stroma by atypical cells with predominantly round hyperchromatic nuclei and scanty cytoplasm. In some areas tumour cells were slender or even spindle in shape. This feature however was most probably a consequence of crush artefact. A provisional diagnosis of atypical spindle cell tumour of uncertain type was made. Leiomyosarcoma, due to the location, seemed most plausible, but it was impossible to exclude other tumours without immunohistochemistry (Figure 1). Besides, the small volume of the biopsy and its imperfect quality complicated histological diagnosis. The results of immunohistochemistry did not correspond to the diagnosis of leiomyosarcoma because of smooth muscle actin negativity. Cytokeratin negativity ruled out an epithelial tumour, while that of synaptophysin and neurone specific enolase (NSE) excluded a neuroendocrine tumour. The tumour cells’ positivity for vimentin, focally desmin, myogenin and weakly myoglobin (fig 2c & 2d) tilted our suspicion towards a muscle tumour with primitive rhabdoid differentiation, consistent with alveolar rhabdomyosarcoma. Further molecular studies with fluorescence in-situ hybridisation (FISH) showed that the sample was positive for the t(2;13) translocation; PAX3-FKHR, confirming our preliminary diagnosis of alveolar rhabdomyosarcoma. At laparotomy, 6.5 litres of hemorrhagic ascitic fluid was drained. A huge uterine tumour of about 26-week gravid uterine size, an omental cake adherent to the transverse colon, stomach, posterior surface of the spleen and parietal peritoneum were noted, with numerous peritoneal, bowel and anterior abdominal wall metastatic seedlings. The liver appeared normal. After critical assessment, it was decided that a beneficial debulking surgery was not possible. Biopsies of the omental cake and uterine lesion were taken and the abdomen closed up. The omental and uterine biopsies were of sufficient volume and excellent quality, and histologically showed typical picture of alveolar rhabdomyosarcoma (Figure 2). The diagnosis was overt without immunohistochemistry, nevertheless new immunohistochemical investigation and FISH were performed and showed results identical to those on the cervical biopsy. The condition of the patient deteriorated rapidly hence neither radiotherapy nor chemotherapy could be started before she died of fulminant disseminated neoplastic disease 17 days after the surgery. Discussion Rhabdomyosarcoma has been divided into 4 histological types: alveolar, botryoid, embroynal and pleomorphic variants13. The alveolar variant which is extremely rare in the female genital tract11,13 was first described by Riopelle and Thériault in 195614 and a detailed description of its clinicopathological features was given by Enterline and Horn in 195815 . It is an aggressive and rapidly progressing tumour11 . Consequently, early diagnosis and planning of comprehensive treatment are often delayed6 as occurred in our case, where the client presented with late disease (clinical stage IV16 ). Although some promising results have been achieved mainly in chidren17,18 and a few adults12,13 the prognosis of the alveolar variant is generally poor with a vast majority of patients, like in our patient, dying of metastatic disease within a year of diagnosis1,2,3,6,15,19. Alveolar histologic type is associated with an adverse outcome even in clinical stage I patients who had complete resection of the disease12 . The most common presenting symptom of cervical sarcomas in adults is vaginal bleeding2 and vaginal examination usually reveals a polypoid mass projecting from the cervix or an expanding mass replacing it, while ulceroinfiltrative lesions are infrequent11 . The aetiology of alveolar rhabdomyosarcoma is not fully understood though a history of trauma is present in some cases15 . In sites lacking striated muscle, such as the endometrium, the tumour may arise either from persisting primitive embryonal cell nests or from the mucosal stroma by the process of metaplasia11 . Grossly, the specimens are soft with fleshy pink to yellow brown tumours often with substantial areas of necrosis. Diagnosis of alveolar rhabdomyosarcoma is typically based on the cytological and architectural features of the tumour as seen on haematoxylin and eosin stain11,13 . Microscopically, the tumour is composed of poorly differentiated cells arranged in solid and alveolar patterns, the latter being characterised by ill-defined nests of cells showing central loss of cellular cohesion and formation of irregular “alveolar” spaces. The individual nests are separated by a framework of dense, frequently hyalinised fibrous septa. The peripheral cells of the alveolar spaces adhere in a single layer to the fibrous septa while the central cells are more loosely arranged or “free floating”11 . The individual cells are small, round or oval with scanty, sometimes acidophilic, illdefined cytoplasm containing hyperchromatic nuclei with or without inconspicuous nucleoli. Sometimes, neoplastic rhabdomyoblasts with pronounced stringy or granular, deeply eosinophilic cytoplasm may be present among the less differentiated cells (fig 2a & 2b). Cross-striations are rarely observed and molecular antigens such as myogenin, desmin and sarcomeric actin may be expressed10,11 (fig 2c & 2d). Mitotic figures range from 1 to 20 mitoses per high-power field8 . Though the cytolological and architectural features of our tumour were consistent with the above features we found it necessary to confirm our diagnosis with immunohistochemistry and FISH. Due to the rarity of this tumour variety, there is no standard treatment established in the literature for adult patients and optimal management remains unknown11,12,13 . The treatment of rhabdomyosarcoma, including its alveolar subtype has markedly improved in children and adolescents over the past years mainly due to the use of a multimodality approach consisting of surgery, radiotherapy and chemotherapy11,13,20 . Ferrari et al. recommend similar treatment in adults9 . The Intergroup Rhabdomyosarcoma Study IV (IRS-IV) revealed that though VAC (Vincristine, Actinomycin and Cyclophosphamide) chemotherapy , with or without radiotherapy, remains the gold standard of treatment in children and adolescents, the alveolar subtype fared worse than other types12,13,20 . In adults, though surgery remains the mainstay of treatment, the results especially for alveolar rhabdomyosarcoma remain very poor11 . Surgical management consisting of excision with the margins free of tumour and resection of the draining lymph nodes together with pre-and postoperative radiotherapy to the tumour site and involved nodal group offers the best chance of cure11 . The risks of using radiation therapy in the management of female genital tract rhabdomyosarcomas include slipped capital femoral epiphysis, nonfusion of the pubic rami, and hypoplasia of the female genital organs including radiation castration6 . While Ng et al. used surgery, aggressive adjuvant chemotherapy (three 6-weekly cycles of VAC, etoposide, ifosfamide and mesna) and radiotherapy to treat an adult case of alveolar rhabdomyosarcoma of the cervix12 , Case et al. used five cycles each of neoadjuvant and adjuvant VAC chemotherapy and surgery to treat another adult case of alveolar rhabdomyosarcoma of the uterus13 , with both cases achieving complete remission12,13 . Our patient presented with advanced neoplastic disease (clinical stage IV), exploratory laparotomy done was of limited value due to the widespread metastases of the tumour and neither palliative chemotherapy nor radiotherapy could be started before she died of fulminant disseminated neoplastic disease 17 days postoperatively. Though there are limited recommendations for the definitive management of this rare tumour variety, due to its rapid progression, early recognition and diagnosis, and a prompt multimodality treatment approach comprising surgery, chemotherapy and radiotherapy offers the best chance of cure. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09015f1.jpg] [rh09015f2.jpg] |
| |||||||||

{kind=link}
{kind=link}