 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
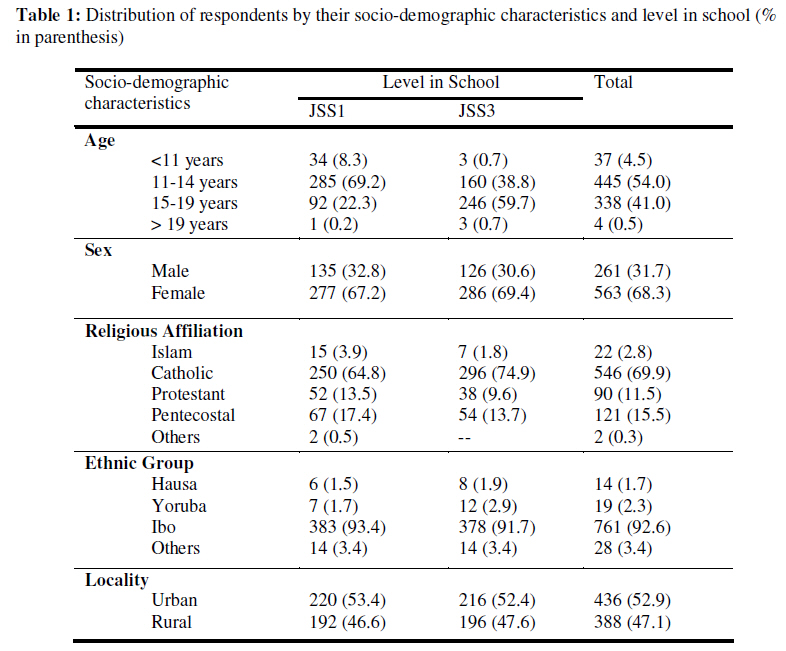
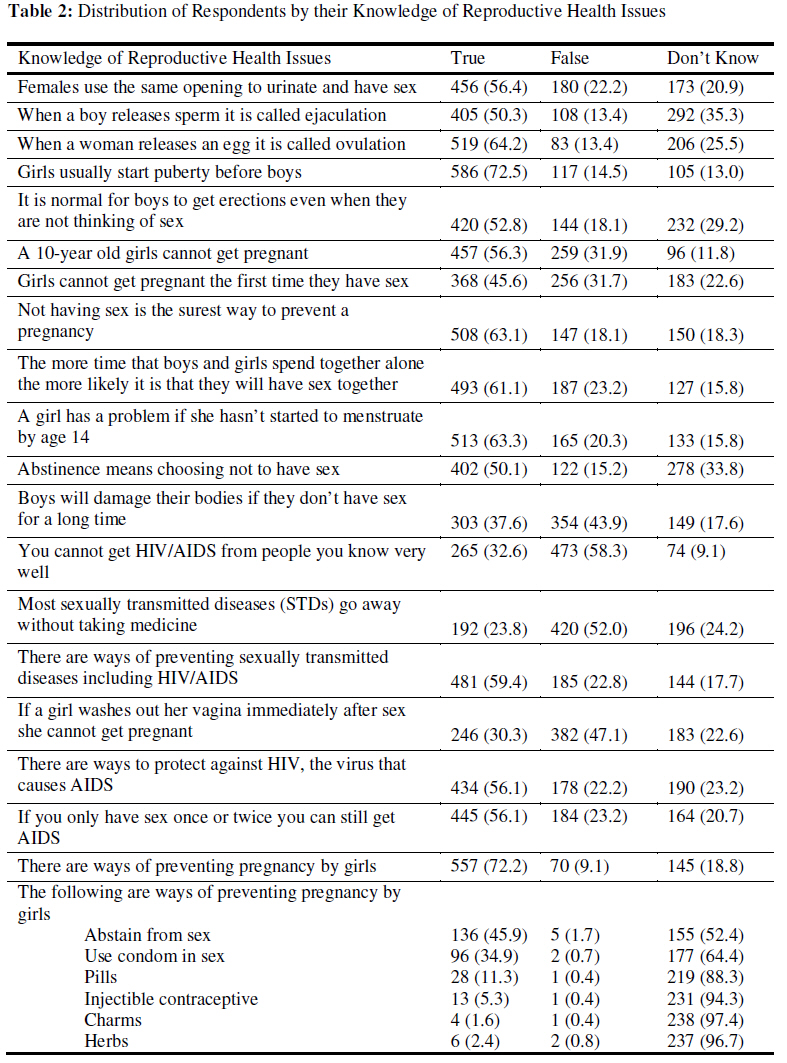
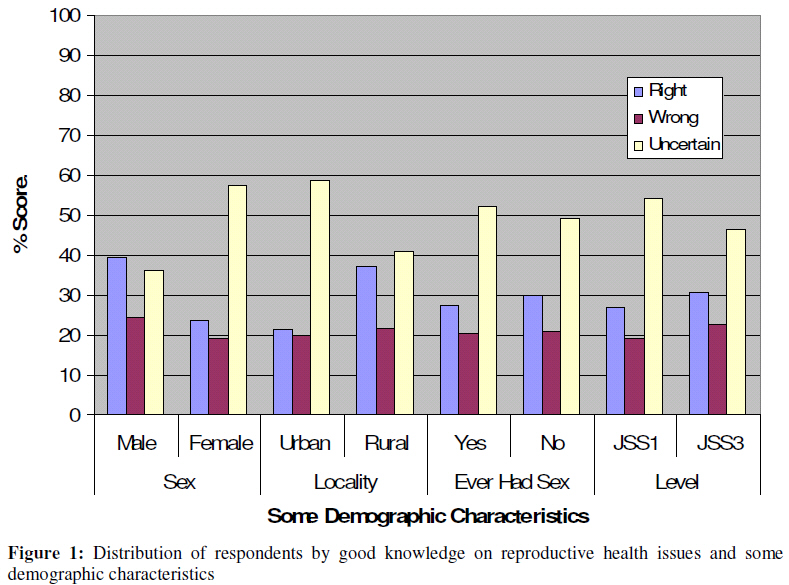
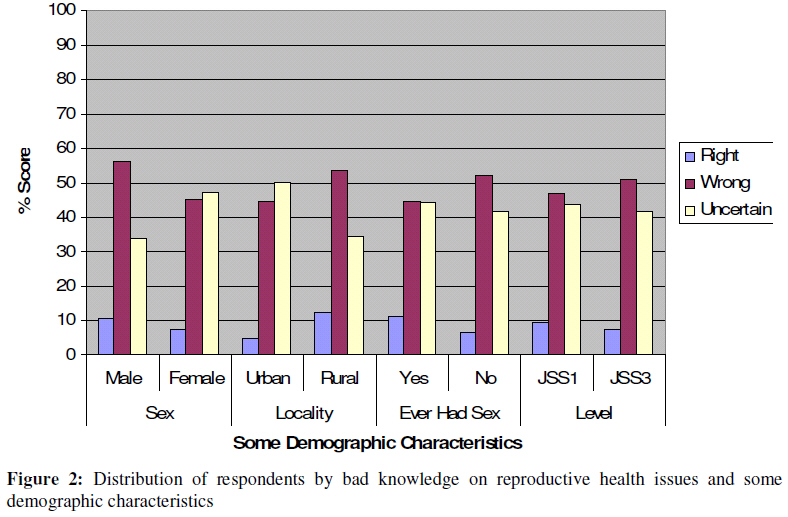
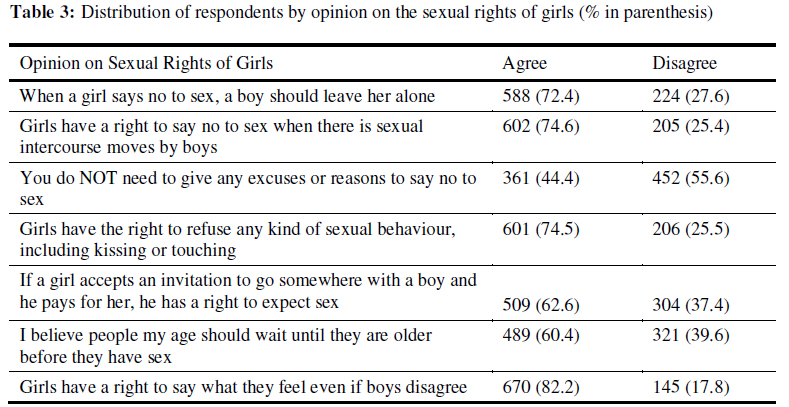
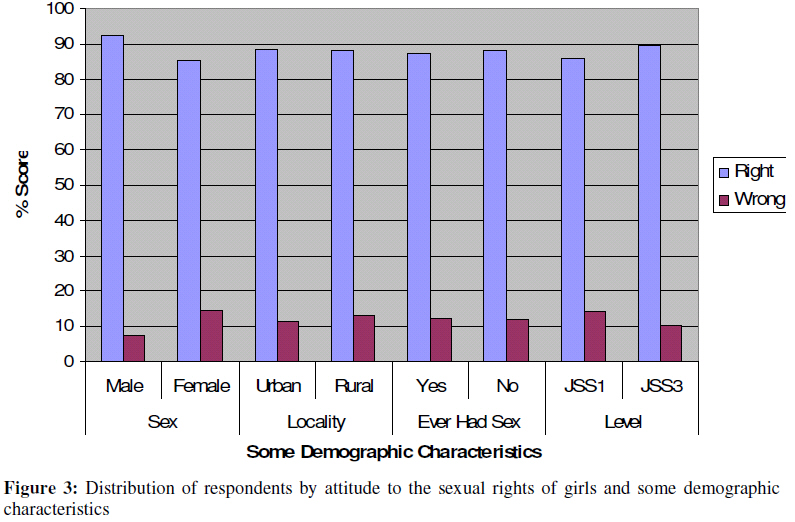
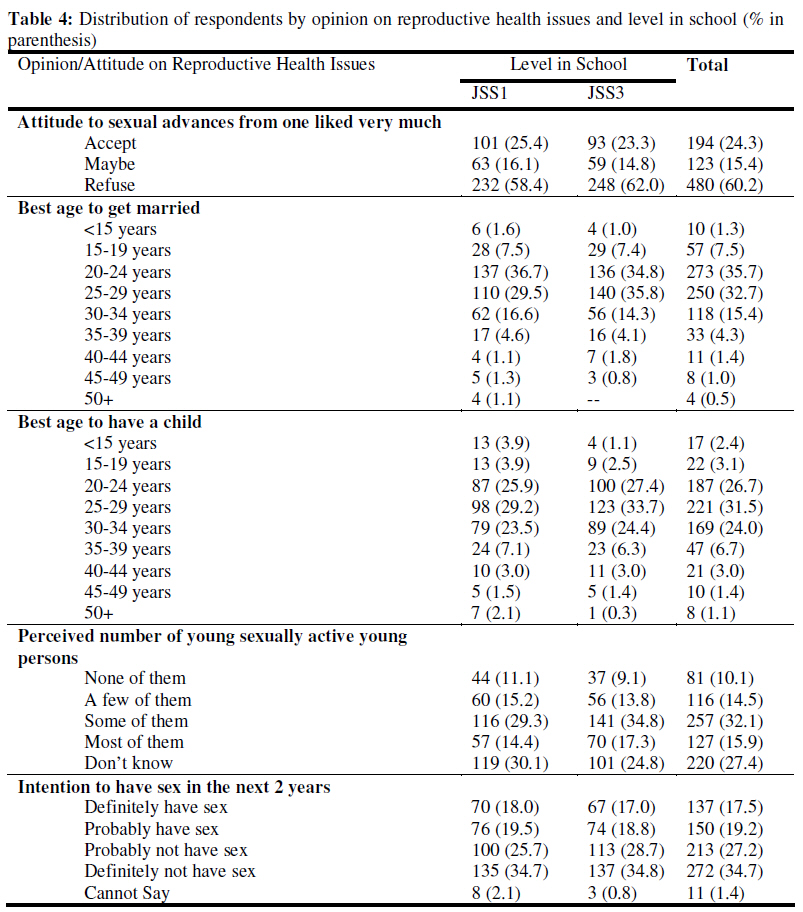
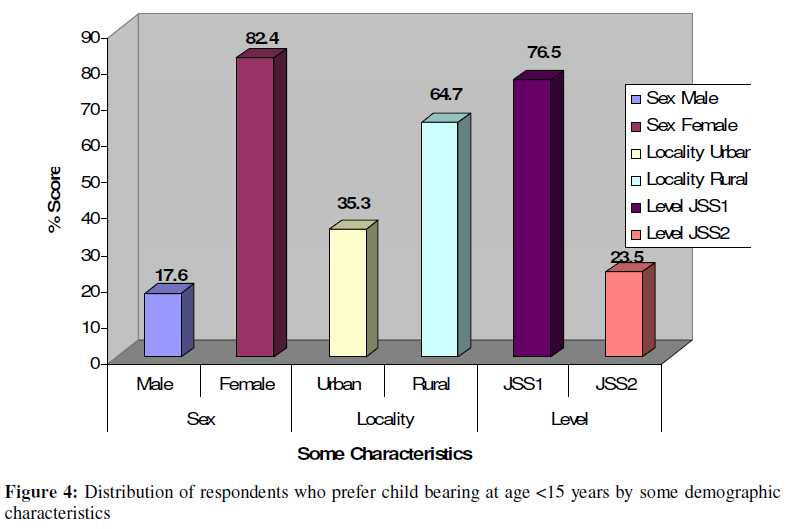
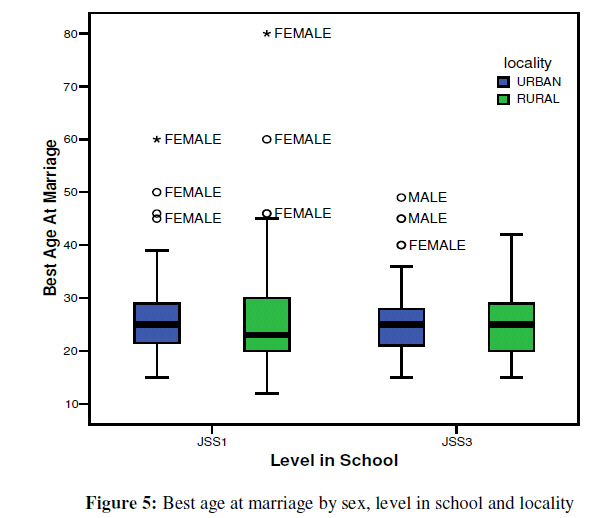
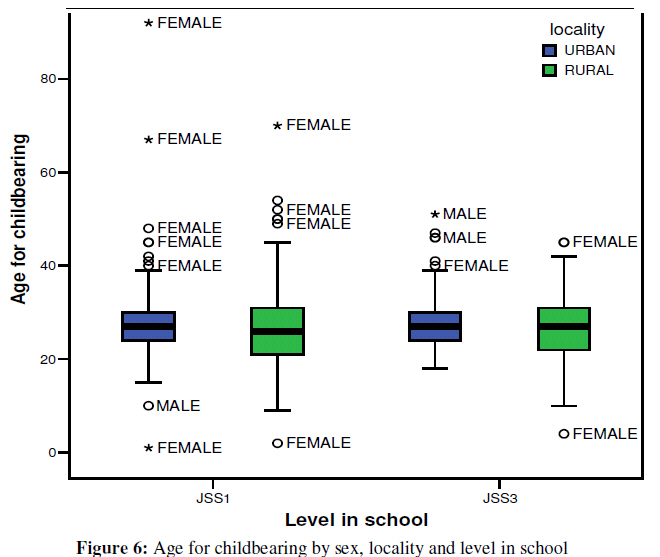
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 17-32 Original research article Family Life and HIV/AIDS Education (FLHE) in Schools in Enugu State: Baseline Study of Reproductive Health Issues among In-School Adolescents in Enugu State Vie familiale et l’éducation sur le VIH/SIDA (VFEV) dans les écoles de l’Etat d’Enugu : Etude de ligne de base sur les questions de la santé de reproduction chez les adolescents qui fréquentent l’école dans l’Etat d’EnuguObioma C. Nwaorgu1; Nkechi G Onyeneho2*, Nkeadi Onyegegbu3, May Okolo4 , Obadike Ebele4, Gladys Ugochukwu4, Chinyere Mbaekwe4 1Department of Parasitology & Entomology, Nnamdi Azikiwe University, Awka; 2 Department of Sociology/Anthropology, University of Nigeria, Nsukka; 3 Institute of Education, University of Nigeria, Nsukka; 4 Global Health Awareness Research Foundation (GHARF), S/34 Edward Nnaji Park, Enugu Code Number: rh09017 ABSTRACT We studied the sexual and reproductive health (SRH) knowledge and practices among junior secondary school grades 1 and 3 students Enugu State, preparatory to incorporating family life and HIV/AIDS education (FLHE) into the school curricula in the state. Results show that over 90% of the respondents were regularly involved in sexual activities. More than seventeen per cent (17.5%) indicated that they would definitely have sex in the next two years while 19.2% may have sex in the next two years. The students lacked proper knowledge of protection and knowledge scores on SRH issues was low especially among the urban dwellers (p<0.001). Some respondents (64.4%) did not know if condoms prevent pregnancy. Some indicated that charms and herbs are effective ways of preventing pregnancy. Against this background, the opinion leaders and community members welcome the FLHE for improving youth knowledge on SRH issues and pledge their support for the programme (Afr J Reprod Health 2009; 13[2]:17-32). RĖSUMĖ Nous avons étudié la connaissance et les pratiques de la santé sexuelle et de reproduction (SSR) chez les étudiants de collège (première et troisième années) dans l’Etat d’Enugu, en vue de l’incorporation de la vie familiale et de l’éducation sur le VIH/SIDA (VFEV) dans le programme éducatif dans l’Etat. Les résultats ont montré que plus de 90% des enquêtés ont participé de façon régulière aux activités sexuelles. Plus de dix-sept pourcent (17%) ont indiqué qu’ils ont la ferme intention d’avoir des rapports sexuels dans les deux prochaines années, alors que 19,2% auraient peutêtre des rapports sexuels dans les deux prochaines années. Les étudiants n’avaient pas une bonne connaissance de comment se protéger et les cotations concernant les questions portant sur la SSR étaient bas surtout chez les citadins (p<0,00001). 64,4% des enquêtés ne savaient pas si les préservatifs préviennent la grossesse. Dans ce contexte, les dirigeants d’opinions et les membres de la communauté apprécient la VFEV pour l’amélioration de la connaissance chez la jeunesse sur les questions concernant la SSR et font la promesse de soutenir le programme (Afr J Reprod Health 2009; 13[2]:17-32). KEYWORDS: Education, Family-Life, HIV/AIDS, Reproductive-Health, Sexual, Enugu Introduction As the threat of reproductive health hazards confronting the youth in Nigeria become a focus of research, advocacy, policy and legal initiatives, the problems associated with youth sexuality, such as unprotected sexual activities, low contraceptive use and inability to negotiate safe sex as well as clandestine abortion become readily apparent 1 . Moreover, HIV/AIDS is hitting the youth hard as studies in Africa show that about 7 in every 10 new HIV infections among females occur among those aged 15 to 24 years2 . The Population Reference Bureau3 notes that one third (36.5 million) of Nigeria's total population of 123 million in 2000 are youths between the ages of 10 and 24.4 The United Nationsprojected that by 2025 the number of Nigerian youth will exceed 57 million. Health concerns of government and individuals were for a long time circumscribed to people outside this age interval, that is the aged and children, to the detriment of this important segment of the society. The adolescent age is a period of numerous changes, including physical, biological, social and psychological. The adolescents, in their quest for information, which is often unavailable from the adults, ostensibly for moral and ethical reasons, resort to experiment with their peers to discover themselves. Lack of planned sexual health information and services places these young people at risk of unwanted pregnancy, abortion, sexually transmitted infections (STI), and HIV/AIDS. Effective and innovative programs can provide youth with the sexual health information and services they need, in recognition of the high level of sexual activities among the youth.5 A survey by the National Population Commission6 revealed that over 16 percent of teenage females in Nigeria reported first sexual intercourse by age 15. Among young women aged 20 to 24, nearly half (49.4 percent) reported first sex by age 18. Among teenage males, 8.3 percent reported first sex by age 15. Among those aged 20 to 24, 36.3 percent reported first sexual intercourse by age 18. A survey of post secondary school girls in Enugu State revealed that 21 per cent of the girls surveyed have had unwanted pregnancies and 18 per cent indicated that they have had induced abortion7 . The young people indulge in sexual activities for both pecuniary and nonpecuniary benefits such as just fun, wish to belong with the joneses and outright ignorance of their escapade. In one survey of sexually experienced teens in Nigerian rural and urban centres, over 13 percent of women and over 27 percent of men reported exchanging money, gifts, or favours for sex in the previous 12 months.6 The implication of this practice is enormous. In 1999, Nigeria's adolescent fertility rate was 111 births per 1,000 women ages 15 to 19. Teenage mothers were more likely than older women to suffer from serious complications during delivery, resulting in higher morbidity and mortality for both mothers and infants.6 Moreover, early childbearing limits youth's educational and employment opportunities. Performing or seeking an abortion is illegal in Nigeria, except to save a woman's life. Yet, experts estimate that more than 600,000 Nigerian women obtain abortions each year.8 A hospital based study found that one-third of women obtaining abortions was adolescents.9 The study revealed that up to 80 percent of Nigerian patients with abortion-related complications were adolescents. The young people lacked knowledge of contraception, and where they know, they use them inconsistently because of the fear for social and cultural sanctions from the adults and teachers in society. Among sexually active, single youth, reasons for non-use of contraception included fear of complications (46.7 percent of males and 48.5 percent of females) and religious beliefs (12.0 percent of males and 21.2 percent of females). Forty percent of youth believed that condoms would reduce sexual pleasure 10 . To address the vulnerability of young people, research and programme attention has focused on giving them correct information. This is in recognition of the fact that while the youth may be ‘protected’ from sexual knowledge, they are being laid open to the risks of avoidable reproductive health hazards. This calls for a change in the old attitude of teachers teaching only that aspect of reproductive biology that is required for passing examination1 to giving the adolescents family life education in schools. This is expedient if the millennium development goal, which has the improvement of reproductive health as one of its main thrusts, will be realizable in Nigeria. In this direction, the MacArthur Foundation funded the incorporation of family life education (FLE) into school curricula in Nigeria. The Global Health Awareness Research Foundation (GHARF), an Enugu-based nongovernmental organization, was mandated to facilitate the programme in Enugu State, Southeast Nigeria, in collaboration with the State government. In pursuit of this, a baseline study was conducted to provide the necessary data for planning and implementing the programme in the State. This paper therefore presents results of the survey of sexual and reproductive health knowledge and practice among young people in schools in Enugu State before the introduction and implementation of family life and HIV/AIDS education in school curriculum in the state. Methods Study Area and Design The study was located in Enugu State, southeastern Nigeria. The people are predominantly Igbo with strong attachment to traditionalism. Though highly Christianized and civilized, the people attach great importance to certain acts considered abominable and sinful against the earth11 . Some of such acts are premarital sex and pregnancy out of wedlock. Here adults do not discuss sexuality with the young persons with the fear that they might be exposed to immorality and commit the abominable. Ironically, the adults prevent the young persons from receiving correct knowledge on sexuality and reproductive health issues and expose them to the dangers of the ubiquitous reproductive health hazards through sexual experimentation. The young people access Western cultures through the cyber cafes, found mainly in the urban areas and to some extent in the semi urban communities. A cross sectional design was employed in the study with focus on young people in secondary schools as the main unit of analysis. Survey method was used to obtain information from the young people. Qualitative data were also collected from members of the communities housing the study schools. This is because literature shows that knowledge and attitudes about reproductive health issues are socioculturally determined and can be influenced by multiple extra-personal factors. Population and Sampling In estimating the sample size for the study, 50% probability score at 95% confidence interval was assumed because there is no known publication on the level of knowledge on reproductive health among in-school adolescents in Enugu State. The formula gave a minimum sample size of 384 students. Since the study area is comprised of rural and urban communities, which is presumed to dispose the students to varying cultures, the sample size was doubled to cover rural urban difference. This thus brought the sample size to a minimum of 768 for the entire State. However, a total of 824 students were interviewed. Enugu State is divided into six educational zones, namely Agbani, Awgu, Enugu, Nsukka, Obollo-Afor and Udi zones. There are a total of 285 secondary schools with a total student population of 156,800. The schools are run at two major levels Junior and Senior Secondary Schools levels. The target population was students in JSS1 and JSS3. This population would allow for follow-up and evaluation of the intervention. Two schools were randomly sampled (one urban and one rural) from each of the six educational zones in Enugu State, this giving a total of 12 schools. Seventy respondents, that is, 35 each for JSS1 and JSS3 were selected by balloting from each of the study schools. In addition to this, the head teachers of the selected schools as well as community leaders and members of the communities harboring the school provided the qualitative data. Data Collection Three sets of instruments were employed in the study, each targeting different sources of information. These included: a self-administered questionnaire to obtain data from the in-school youth; focus group discussions (FGDs) with community members; in-depth interview for head teachers and community leaders. Results Socio-demographic Characteristics of the In-school Adolescents More than sixty per cent (68.3%) of the respondents were females. The ages of the respondents ranged from 10 to 20 years with a mean age of 14.25 years and a standard deviation of +/-1.841 years. Christians dominated the study area see (Table 1). Knowledge, Perceptions and Attitudes about Reproductive Health More than half of the respondents gave correct responses to questions on the male and female reproductive organs (Table 2). About fifty percent (50.1%) correctly indicated that, “abstinence means choosing not to have sex”, while (33.8%) of the respondents were ignorant of this. Worse still, on the ways of preventing pregnancy by girls, very high proportions of the respondents were ignorant about this. For instance 52.4% and 64.4% of the respondents indicated that they did not know if abstinence and condoms were effective ways of preventing pregnancy in girls. Some also indicated that charms and herbs are effective ways of preventing pregnancy in girls. A further analysis of the knowledge level of the respondents led to the development of knowledge index on all the issues raised for the respondents. The right knowledge questions were cumulated and the wrong knowledge statement cumulated together. The results show that only 28.7% of the respondents correctly recognized the right knowledge information. More than fifty per cent (50.5%) got the right knowledge statements wrong. On the other hand, only 8.4% of the respondents were able to correctly identify the wrong knowledge information. A majority of the respondents, cumulatively, were uncertain on what is right or wrong about the issues raised. The influence of some demographic variables on the students’ knowledge about reproductive health issues was examined in Figures 1 and 2. Figure 1 revealed that a higher percentage of girls than boys were uncertain on the correct options to the reproductive health question (p<0.001). Similarly, it was observed that rural dwellers had better knowledge on reproductive health issues than the urban dwellers (p<0.001). Figure 2 also revealed that the boys were more certain about what constitutes the wrong knowledge about reproductive health issues than the girls (p=0.002). In the same vein, more of the rural residents, vis-à-vis their urban counterparts could correctly identify the wrong ideas about human reproduction (p<0.001). Figure 2 also revealed poorer knowledge among those who have ever had sex (p=0.03). Table 3 shows that high proportions of the respondents agreed with all the statements made to gauge their opinion on the sexual rights of girls. Interestingly, however, some of these ideas were manifestations of poor recognition for the sexual rights of girls. For instance, 62.6% of the respondents agreed that girls who accept male invitation and sponsorship to a function should recognize the right of the boy to demand sex. On the other hand, 44.4% of the respondents hold the opinion that girls do not need to give any excuses or reasons to say no to sex. Further more, 39.6% of the respondents disagreed with the idea that school age persons should wait until they are older before they have sex. Figure 3 shows that the respondents, irrespective of their demographic characteristics, were largely in agreement with ideas that promote the sexual rights of girls. However, there was a statistically significant difference in attitude towards the sexual rights of girls However, the respondents espoused by sex (p=0.006). More male respon-different opinion on broad reproductive dents held positive attitudes on ideas that health issues when probed further. Some promote the sexual rights of girls. of the issues and the opinions of the respondents are presented on Table 4 below. Less than two-thirds (60.2%) of the respondents would refuse sexual advances if someone they liked a lot wanted to have sex with them. Much as this sounds good more than a third (39.7%) stand the risk of accepting. About a quarter (24.3%) would definitely say yes to the sexual request and have sex with the person. On the best age to get married, the respondents differed greatly. The ages indicated as proper for marriage ranged from less than 10 years to as much as more than 50 years, with a median of 25 years, a mean of 25.1 years and a standard deviation of +/-6.16 years. More than a third (35.7%) of the respondents mentioned ages 20-24 years as the best age for marriage. It is important to note that some of the young persons, in junior secondary schools interviewed indicated that the best age for marriage is before 10 years. The Table further reviewed the ages considered as the best for child bearing by the respondents. It shows, for instance that the ages ranged from less than 15 years and extends beyond 50 years, with a mean of 27.44 years, a median of 27 years and a standard deviation of +/-7.306 years. Less than a third (31.5%) of the respondents think that the best page for childbearing is between 25-29 years. More than half (58.2%) of the respondents however indicated the period 20-29 years as best for childbearing. Ironically, the feamle respondents, who should be most threatened with the problems of early child bearing subscribed more to the notion of having children at ages less than 15 years as shown in Figure 4 below. Figure 4 shows that more females than males subscribed to early childbearing age. Similarly, more of those from the rural segment of the study supported child bearing to start as early as less than 15 years. Further review of the situation using box plot show the actual distributions of the respondents with respect to the perceived best age for child bearing and marriage. See Figures 5 and 6 below. The preferred age for getting married ranged from as low as ten years among the respondents with urban background. For those with rural background the recommended age at marriage start from as low as age 12 years. All the same the Figure shows that the median age for marriage recommended by both the boys and girls is lower among the JSS1 students with rural background than any other group. An important finding, here, however is that there were female outliers recommending ages much lower than 10 years for child bearing. When this is juxtaposed on the recommended age for marriage one finds a worrisome situation that may promote child bearing out of wedlock. Table 4 further revealed the respondents’ perception of the level of sexuality among school-aged persons. Six in every ten persons interviewed think the young persons of school age are having sex or getting involved in sexual intercourse while the others were ignorant. About a third (32.1%) were definite that some of the young persons are involved in sexual intercourse. More than seventeen per cent (17.5%) of the respondents indicated that they would definitely have sex in the next two years while 19.2% indicated that they would probably have sex in the next two years. More than twenty-seven per cent (27.2%) indicated that they probably would not have sex within this period. Perceptions/Opinion of Head Teachers, Community Leaders & Members about FLE Results from the FGDs and in-depth interviews with community members and their leaders respectively indicated awareness of the reproductive health hazards threatening the lives of young persons in the communities. The worry for most of them stems from the apparent, though hidden sexual exploits of the young ones in the community. According to the community leader for Uda, in Obollo Afor Educational zone, “we are aware of these problems and many of our children are today falling victims of such problems as gonorrhea, syphilis and HIV/AIDS, unwanted pregnancies, unsafe abortions. We only know of a victim when the problem begins to manifest”. In Awgu educational zone the response was very similar. The response of a community leader in this zone typified the mood here when he emphasized, “yes an unsafe abortion that leads to ruptured wombs and fallopian tubes is common among our young girls. The other problems are sexually transmitted disease especially HIV/AIDS which is ravaging our people now”. One of the head teachers of the school in this zone noted that, “the problem of teenage pregnancy is more rampant in the rural areas. They manifest mostly after festive seasons like Christmas or any such festivity that bring the boys from the town”. People almost spontaneously gave a long list of reproductive health hazards that threaten the lives of the young people in FGD sessions irrespective of the zone or communities. “We have seen young people suffering from these diseases” they often mentioned. They also mentioned that though parents educate their children this is not often detailed because the parents would not tell the children everything. Opinions about the FLE expressed by community leaders in an in-depth interview and in FGDs by community members were generally positive. They noted that it is a good idea and requested that everything should be covered under this subject if the young ones are to be saved. Yes, it is good to teach them because, it will help to prevent the spread of AIDS. We support the idea very well, please go on with the programme. We like the programme and want the government to follow it up for proper implementation (Adult women, Iva Valley) It is good to divide the FLE & HIV education into different categories of teaching primary & secondary school level of teaching as well as the higher institutions. A few minority voices against the FLE were however noticed. They cautioned against giving the wrong signal to the young people when they are made to know everything about sexuality in their early ages. For instance, in an FGD with adult males in Agugbowa, a participant argued that, “each level (education) should have a limit to what is to be taught. If you teach the same thing to those in University and Secondary School we may not be able to take the consequences”. Another member of the group however countered quickly. “When you fail to let the young know all they should know in an organized manner they get untaught by the peers who give them the wrong ideas like “boys will damage their bodies if they don’t have sex…” or “you cannot get HIV/AIDS from people you know very well”. A male community leader in Udi noted, “I have never heard of it, but I know that the church and some parents give moral instructions. The schools do too but this will be more organized and help us a lot. I welcome it in my community” Similarly, another community leader observed, “It is easy for those teaching the children to teach them these things”. In a number of the rural communities it was lamented that the young people are left on their own with no knowledge on how to conduct themselves as they begin to witness changes in their life. In Obe community for instance, a community leader noted that, “parents attempt to sex educate their children but according to him this is only among the educated parents. Villagers do not do it because our culture sees such education as taboo. Another community leader noted that his people do not even attempt doing so. According to him, “they don’t. They are always busy for what to eat and also not all are enlightened. But if the parents educate their children, there will be fewer stories of sexuality problems among the youth” Discussion The study revealed that substantial knowledge about reproductive health issues exist among the young persons in schools. These may be due to the efforts of the numerous Non-governmental Organizations working on health issues in the State through informal peer education clubs. However, young people from the urban areas tend to be poorer in knowledge than their rural counterparts. Though this is curious, the poor knowledge among the students with urban background may be linked to the numerous avenues they have for unguarded ‘novel ideas’ outside the school. The rural segment may have depended more on the civic and religious education they get and less on wrong knowledge through peer influence. A good number of the youths, especially the boys recognize the sexual rights of the girls. However, the number that holds wrong idea about very critical elements of reproductive health should a source of worry to teachers, parents and practitioners of reproductive health among young persons. The young persons are sexually active. Many of those who are sexually active lack correct knowledge or information on reproductive health issues and worse still engage in unprotected sex for different reasons. The results show that young people who have ever had sex had very low knowledge score about reproductive health issues. Some of them rely on charms to protect them from unwanted pregnancy and sexually transmitted diseases. High proportions of the young persons interviewed were uncertain of ways of protecting themselves. The level of knowledge was particularly worse among the young persons with urban background and this is attributable to the level of interaction with peers in the urban areas as well as exposure to Western cultures through cyber cafes and movies. These are very serious lessons for programming. It shows that the quality of knowledge would is responsible for the actions taken by the young persons, most of whom get the wrong information from peers, especially in the urban areas. The boys also seem to have better knowledge than the girls. The qualitative data show that reproductive health hazard is a very big problem among young people in most communities in Nigeria. Many suffer from unsafe abortion related reproductive health problem. Others suffer from sexually transmitted diseases like gonorrhea and HIV/AIDS. The population is greatly threatened by the possibility of HIV/AIDS, which has no cure. Parents and schools teacher give moral instructions to the young people even though these were judged insufficient. The young persons receive wrong information from their peers. Some of which include “boys will damage their bodies if they don’t have sex…” or “you cannot get HIV/AIDS from people you know very well”. Some youth also argue that it is natural and normal to have sex. It is therefore recommended that there family life education should be integrated into the school curriculum young persons. This will be delivered as part of their routine schoolwork. This type of teaching will not be changed easily in the informal setting because the young persons would see it as one of the subjects essential in passing through school. It is hoped that this will gradually lead to behaviour change and thereby reduction in sexuality and reproductive health problems including HIV/AIDS among the youth in the state. Acknowledgements The study received financial support from the Catherine T. and John D. MacArthur Foundation. We also acknowledge the contributions of the authorities and students of schools visited from data collection as well as the leaders and members of the school communities who provided information for the study. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09018t4.jpg] [rh09018f4.jpg] [rh09018f3.jpg] [rh09018f1.jpg] [rh09018t3.jpg] [rh09018t1.jpg] [rh09018f6.jpg] [rh09018t2.jpg] [rh09018f2.jpg] [rh09018f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}