 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
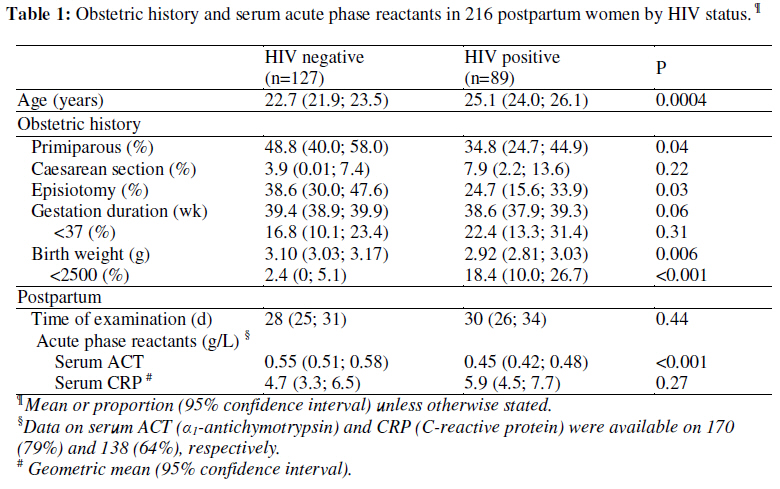
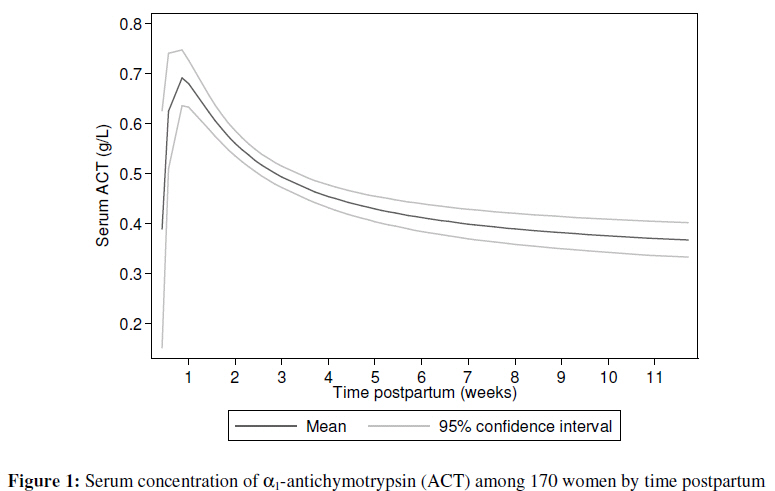
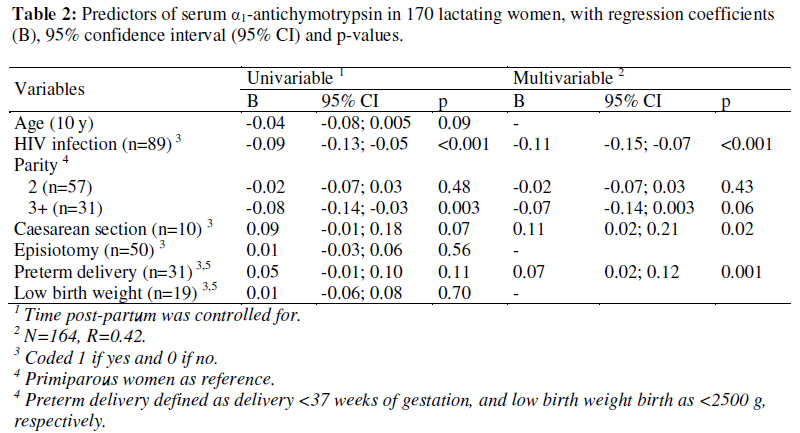
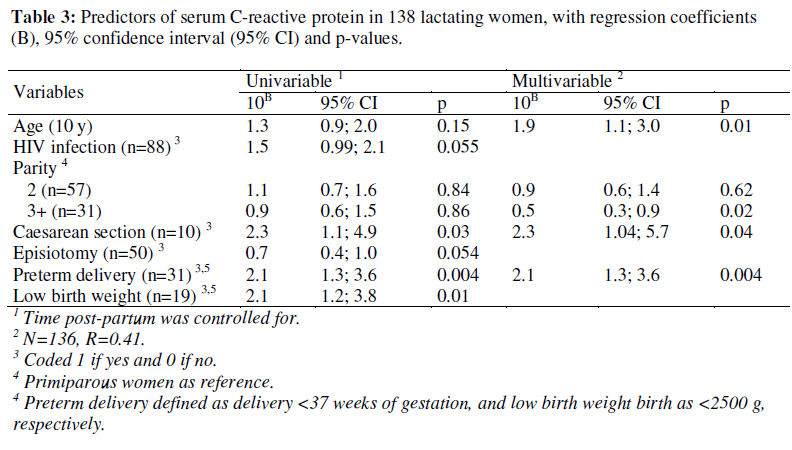
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 61-68 Original research article The Acute Phase Response to Parturition: A Cross-Sectional Study in Zimbabwe Réponse de la phase aiguë a la parturition: une étude transversale au ZimbabweHenrik Friis 1, Exnevia Gomo 2, 3, Wilson Mashange 3, Norman Nyazema 4, Pernille Kæstel5 , Frank Wieringa6 , Henrik Krarup 7 1 Department of Human Nutrition, University of Copenhagen, Denmark; 2 Research Support Centre, College of Medicine, University of Malawi, Malawi; 3 National Institute of Health Research (formerly Blair Research Institute), Ministry of Health and Child Welfare, Zimbabwe; 4 Department of Clinical Pharmacology, University of Zimbabwe, Harare, Zimbabwe; 5 Department of Human Nutrition, Faculty of Life Sciences, University of Copenhagen, Frederiksberg, Denmark; 6 Nutrition, Food and Societies, Institute of Research for Development, Montpellier, France; 7 Department of Clinical Biochemistry, Aalborg University Hospital, Aalborg, Denmark. Code Number: rh09022 ABSTRACT Parturition triggers an acute phase response, but its magnitude, duration and predictors are not well described. We determined serum α1-antichymotrypsin (ACT) and C-reactive protein (CRP) among 216 women attending postpartum services in south-eastern Zimbabwe. Serum CRP peaked during the first week and serum ACT around 9 days postpartum. Serum ACT, but not serum CRP, was lower among HIV infected women. Multiparity was a negative, and preterm delivery and caesarean section were positive predictors of both serum ACT and CRP. There is a need for a better understanding of the acute phase response to parturition (Afr J Reprod Health 2009; 13[2]:61-68). RĖSUMĖ La parturition déclenché une réponse de la phase aiguë, mais son ampleur, sa durée et ses indices ne Sont pas bien décrits. Nous avons détermine la sérique alpha-antichymotrypsin (AAT) et la protéine C-réactive (PCR) chez 216 femmes qui fréquentaient les services du post-partum au sud-est du Zimbabwe. La sérique PCR a atteint le maximum au cours de la première semaine et la sérique AAT après un post-partum d’à peu près neuf jours. La sérique AAT (non pas la sérique PCR) était moins élevée chez les femmes séropositives. La multiparité était un indice négatif, tandis que l’accouchement avant terme et l’opération césarienne étaient des indices positifs de la sérique AAT et PCR. Il faut une meilleure compréhension de la réponse de la phase aiguë à la parturition (Afr J Reprod Health 2009; 13[2]:61-68). KEYWORDS: Acute phase response, α1-antichymotrypsin, C-reactive protein, HIV, postpartum, Zimbabwe Introduction Infection and trauma trigger an acute phase response (APR), which is a generalized, stereotypic host reaction, mediated by cascades of cytokines1 . The APR results in a marked change in the turnover of many proteins, and changes in their serum concentrations. Some of these proteins, such as α1antichymotrypsin (ACT) and C-reactive protein (CRP), are called acute phase proteins (APP’s). But serum concentrations of markers of micronutrient status, e.g. ferritin (iron) and retinol (vitamin A), are also affected by the APR2 . Attempts have been made to correct for these effects of the APR on markers of micronutrient status3-6 , but more data are needed on the magnitude and time course of the APP to be able to correct for its effect. Parturition also triggers an APR7 . The time course and magnitude of elevated serum acute phase reactants, such as ACT and CRP in the postpartum period are not well described. Besides, other factors contributing to or modifying the maternal parturition-induced acute phase response have not been identified. To describe the magnitude and time course of the postpartum APR, and to assess the role of obstetric procedures, pregnancy outcome, as well as HIV infection, as predictors of serum ACT and CRP, we performed a cross-sectional study among women in Zimbabwe. Subjects and Methods Women attending postpartum services at Chiredzi District Hospital, south-eastern Zimbabwe, were recruited. A questionnaire was administered and clinical examination and blood sampling done. The questionnaire was used to gather demographic data, and medical and obstetric history. Duration of gestation was calculated from the first day of the last menstruation and the date of birth. HIV tests were done using two different EIA based on different antigens (Genelavia Mixt, Sanofi, France; and Recombigen; Cambridge Biotech, Ireland). Samples found positive or indeterminate were later tested at the Department of Clinical Chemistry, Aalborg University Hospital, Denmark, using a modification of an in-house developed RT-PCR8 . For the purpose of studying serum ACT, HIV infected women were oversampled. From all those with a positive initial test, and on a random sample of two thirds of those with a negative initial HIV test, additional blood was collected for determination of acute phase reactants, and serum was separated and stored in liquid nitrogen at -196 oC until analysed. Serum ACT and CRP were measured by automated turbidimetry (Cobas Mira Plus; Roche, Switzerland). For serum ACT, rabbit anti-human ACT (DAKO, Glostrup, Denmark) was used to precipitate ACT and turbidity measured at 345 nm after 8.3 min incubation at 37oC. The results were given as g/L serum based on a standard curve from commercial calibrators (DAKO, Glostrup, Denmark). The test range for the assay was 0.05 to 1.20 g/L. Serum CRP was measured using human CRP antibodies, coated on latex particles, CRP latex (cat. No. A11A00175, ABX The acute phase response to parturition Diagnostics, France). Calibration was made from a series of human CRP calibrators with certified concentrations (A11A00177, ABX Diagnostics, France). Turbidity was measured at 340 nm after incubation for 6.7 min. at 37 °C. The test range of the assay was approximately 3– 80 mg/L. Permissions were obtained from the Medical Research Council of Zimbabwe and Danish Central Medical Ethics Committee. Women were pre-test counselled before giving written consent. Post-test and further counselling and support were provided by a nongovernmental organization, Family AIDS Caring Trust, Chiredzi. Antiretroviral treatment was not available at the time of the study. Assuming a mean (SD) of serum ACT of 0.50 (0.20) g/L among HIV uninfected individuals, we would be able to detect a 0.10 g/L difference with 85 HIV uninfected and 85 HIV infected women. The distributions of data were assessed using normal probability plots. Serum CRP values below the detection limit were randomly assigned values between 0.5 to 3 mg/L before log10 transformation. Two-way fractionalpolynomial prediction plots were made using Stata version 9 (StataCorp, College Station, Texas USA). The two-sample ttest and chi-square test were used to test for differences in means and proportions, and multiple linear regression analyses to identify predictors of serum ACT and CRP, while adjusting for time since delivery using dummy variables. Variables were included if p<0.10, and considered significant if <0.05. Results Two-hundred-and-sixteen women were recruited between 3-82 (median 21, interquartile range 11-45) days postpartum. The distribution of time postpartum was bimodal with peaks around 10 days and 6 weeks. Eighty-nine (41%) of the women had HIV-1 infection. Age, obstetric history and serum ACT and CRP are given in Table 1, separately for HIV uninfected and infected women. Data on serum ACT and CRP were available on 170 (79%) and 138 (64%), respectively, of the 216 women. As seen, serum ACT but not CRP was lower among HIV infected women, which was not explained by differences in time of examination or other factors. Serum ACT peaked around 9 days after delivery and declined with time postpartum, with a mean value reaching 0.35 g/L only towards the end of the 12 weeks postpartum (Figure 1). The role of age, parity, caesarean section, episiotomy, preterm delivery, low birth weight and HIV infection as potential predictors of serum ACT, were assessed in linear regression analysis, after adjustment for time postpartum. In the multivariable model (Table 2), HIV was associated with 0.11 g/L lower serum ACT. Multiparous women had 0.07 g/L lower serum ACT compared to primiparous, although only marginally significant (p=0.07, linear trend p=0.058). However, women undergoing caesarean section had a 0.11 g/L higher mean serum ACT, while delivering preterm babies was associated with a 0.07 g/L higher serum ACT. Since preterm delivery and low birth weight were highly correlated, only preterm delivery was included in the model, but without preterm delivery in the model, low birth weight was a positive predictor (0.07, 95% CI: 0.01; 0.14, p=0.03). Neither age nor episiotomy were predictors. Serum CRP peaked during the first week, slightly earlier than serum ACT, and declined faster, although geometric mean values did not go below 3 mg/L during the 12 weeks (data not shown). In multiple linear regression analysis with log10-serum CRP as dependent variable, after adjustment for time postpartum, age, caesarean section, and preterm delivery were positive predictors, and multiparity was a negative predictor (Table 3). Serum CRP increased 1.9 (10B =100.27 =1.9; 95% CI: 1.1; 3.0, p=0.01) times per ten year increase in age. Multiparous women had serum CRP that was only half (0.5; 95%CI: 0.3; 0.9, p=0.02, linear trend p=0.03) that of primiparous. Women delivering by caesarean section had 2.3 (95% CI: 1.04; 5.7, p=0.04) times higher serum CRP compared to giving birth by normal vaginal delivering. As for serum ACT, if entered one at a time, both delivering preterm (2.1, 95% CI: 1.3; 3.6) and low birth weight (2.2; 95% CI: 1.2; 3.9) babies were positive predictors of serum CRP. HIV was not a predictor of serum CRP in the final model (1.3; 95% CI: 0.9; 2.0, p=0.16). Discussion Not only infections, but also parturition precipitates a considerable acute phase response, with mean serum ACT concentrations a week postpartum at the same level as patients with pulmonary tuberculosis at the time of treatment (Friis, unpublished data). We have previously found slightly higher serum ACT among Zimbabwean primigravidae3 , and here we find that the acute phase response to parturition seem to be greater among primiparae compared to multiparae. This is in accordance with findings from a prospective study among Guatemalan women, where saliva cortisol was found to increase transiently a few hours after delivery, and more so in primiparae compared to multiparae9 . Although normal vaginal delivery precipitates an acute phase response, caesarean section is associated with a considerably greater response. While this may be explained by the procedure itself, the underlying complication making caesarean section necessary could contribute. A study among Finnish women undergoing uncomplicated caesarean section found elevated serum CRP peaking the second day postpartum, and that duration of operation was a predictor of serum CRP10 . In contrast to the effect of caesarean section, we found no evidence that episiotomy was triggering an acute phase response probably since the tissue damage involved is minor. Delivering a smaller baby most likely reduces the tissue damage and stress, and hence the acute phase response. The finding that preterm delivery was a predictor of serum ACT and CRP could reflect that the condition leading to preterm delivery was accompanied by a maternal acute phase response. In fact, the acute phase response could be part of the mechanism leading to preterm delivery. Similarly, data from Poland showed that women delivering infants small for gestational age had higher postpartum serum α1antitrypsin compared to women delivering infants appropriate for gestational age11 . We have previously found similar levels of serum ACT among HIV uninfected and infected pregnant Zimbabwean women (0.32 vs 0.32 g/L)(3), suggesting that asymptomatic HIV infection is not associated with an acute phase response. However, our data suggest that HIV infection may impair the acute phase response triggered by other factors. This is conceivable since the acute phase response is immune mediated, and other immuno-suppressive conditions such as malnutrition 12, 13 are also found to impair the acute phase response. Whether the lack of association between HIV and serum CRP is due to the fact that serum CRP is more fastreacting or synthesised by different mechanisms is not clear. It is important to be aware of the considerable and prolonged postpartum acute phase response, and there is a need for a better understanding of its determinants and possible effects. For example, it is likely to have implications for assessment of nutritional status of women in the post-partum period. Moreover, it may hamper the effectiveness of several widely used nutrition and health interventions. For example, iron supplements are often given to women in the postpartum period, but iron absorption is likely to be impaired due to the postpartum APR. The inflammatory cytokine IL-6 stimulates hepatocytes to release ACT14 , but also hepcidin, which blocks release of iron from enterocytes, macrophages and hepatocytes, which results in sequestration of iron in the stores and iron-limited erythropoiesis, and ultimately anaemia of chronic inflammation15 . Similarly, the limited effect of postpartum vitamin A supplementation, recommended by WHO in countries where vitamin A deficiency is widespread16 , could be due to the APR to parturition as recently suggested17 . If so, then it is likely that the intervention is more effective if given when the acute phase response is fading, eg after 6-8 weeks. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09022t1.jpg] [rh09022t2.jpg] [rh09022t3.jpg] [rh09022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}