 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
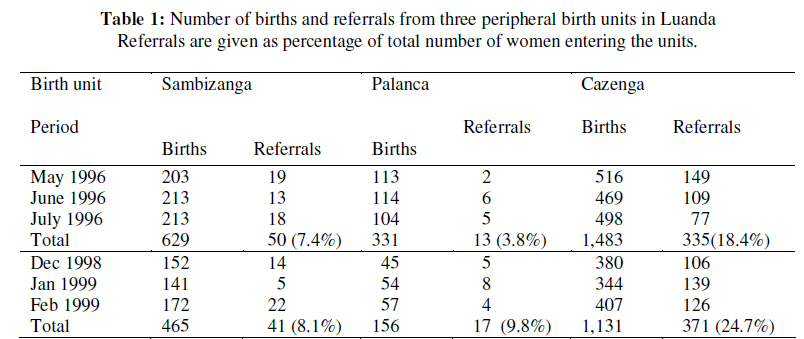
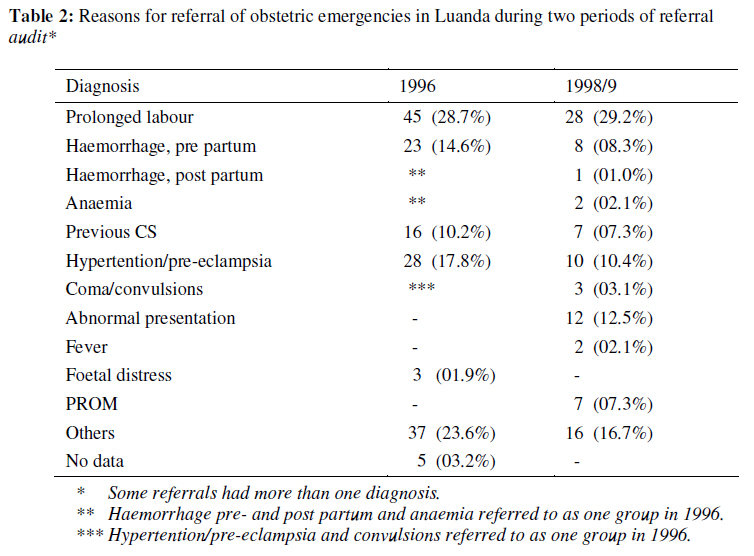
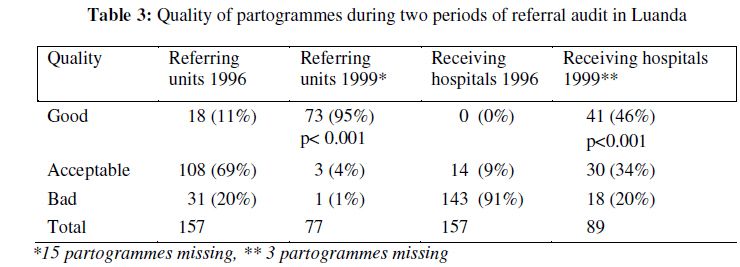
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 75-85 Original research article Audit of Referral of Obstetric Emergencies in Angola: A Tool for Assessing Quality of Care Vérification des orientations vers des services spécialises des cas obstétriques d’urgence en Angola – Un outil pour l’évaluation de la qualité des soins Strand RT1, de Campos PA2, Paulsson G3, de Oliveira J4 and Bergström S1 1Division of International Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, SE-171 76, Stockholm, Sweden; 2 Faculdade de medicina, Departamento de obstetrícia e ginecologia, Luanda, Angola; 3Kvinnokliniken, Södersjukhuset, Stockholm, Sweden; 4 Delegação Provincial de Saúde de Luanda, Angola. Code Number: rh09024 ABSTRACT By auditing various aspects of referrals of obstetric emergencies, we wanted to study the effectiveness over time of a recently established network of peripheral birth units and two central hospitals in Luanda. 157 women referred for obstetric emergencies were studied regarding clinical outcome and process indicators like waiting time, partogramme quality and Caesarean section rate (CSR). After a change in routines at hospital admission and further partogramme education 92 referred women were compared with the former. Maternal mortality decreased from 17.8% to nil in the second. Total mean waiting time was reduced from 13.7 hours to 1.2 hours. Partogramme quality was significantly improved. CSR increased from 13 to 30%. Prolonged labour was the most common diagnosis.This study demonstrates the importance of clinic-based audit to enhance quality of care regarding referrals of patients with obstetric emergencies (Afr J Reprod Health 2009; 13[2]:75-85). RĖSUMĖ En vérifiant les aspects divers des orientations vers les services spécialisés de cas obstétriques d’urgence, nous avons voulu étudier l’efficacité au cours d’une période d’un réseau récemment établi des unîtes de naissance peripherale et deux hôpitaux centraux à Luanda. 157 femmes qui ont été orientées vers les services spécialisés pour des cas obstétriques d’urgence ont été étudiées à l’égard des résultats cliniques et nous avons traité des indices comme la période d’attente, la qualité de la partogramme et le taux de l’opération césarience (TOC). Après une modification à l’égard des routines dans l’administration de l’hôpital et après davantage éducation du partogramme, 92 femmes qui ont été orientées vers les spécialistes ont été comparées a celles-la. La mortalité maternelle a baissé de 17.8% à zéro dans la seconde. Le temps moyen total d’attente a diminué de 13,7 heures a 1,2 hours. La qualité du partogramme s’est améliorée de manière significative. Le TOC a augmenté de 13% à 30%. Le travail prolongé a été le diagnostic commun. L’étude montre l’importance de la vérification basée sur la clinique pour mettre en valeur la qualité du soin concernant l’orientation des patientes qui ont des cas obstétriques d’urgence (Afr J Reprod Health 2009; 13[2]:75-85). KEYWORDS: Africa, audit, obstetric emergency, quality of care, referral, waiting time Introduction Angola is a country marked by social and political turmoil after more than thirty years of warfare. During this period a substantial migration into the national capital Luanda and its vicinities has taken place and added to the pressure on public obstetric services, already suffering from insufficient resources. With the aim of alleviating the heavy overload of patients at the two central maternities, a project was implemented in 1994 as part of the Swedish development co-operation with Angola through the Swedish International Development Cooperation Authority (Sida). This included reconstruction and equipment of nine peripheral birth units (salas de partos periféricas, SPP), run by midwives for normal deliveries without the possibility of administrating intravenous drugs, blood transfusion or manual exploration of the uterus. Via a system of radio communication and ambulances, rapid referral of patients in obstetric emergencies was made possible. A dramatic increase in institutional births has been registered since the completion of the project; from around 36,000 in 1994 to almost 59,000 in 1999. The major part of this change has taken place at the peripheral level; from 8,441 in 1994 to 30,516 in 1999 (Estatística anual de saúde maternal). In spite of this increased utilisation of the SPPs, the aim to reduce the load of deliveries in the two referral hospitals was not reached. The high number of births at these hospitals remained unchanged or even increased. The central hospital, Maternidade Lucrécia Paím (MLP), continued to register more than 18,000 births in both 1994 and in 1999, while the other maternity Maternidade Augosto N´Gangola (MAN) increased from more than 9,000 births in 1994 to over 12,000 in 1999. Most likely, these figures reflect the increasing influx of refugees to Luanda. The institutional maternal mortality ratio has been used as the only, though inappropriate, instrument to assess the quality of obstetric care in Luanda and has shown a decrease from 2,070 per 100,000 live births in 1994 to 772 in 1997, 807 in 1998 and 887 in 1999, parallel to a rekindling of the civil war. Institutional maternal mortality has continued to fluctuate since the time of the study (Estatística anual). There is, however, a growing awareness that maternal mortality ratio as an outcome indicator is too blunt an instrument for assessing quality of obstetric care, particularly in low-income countries1,2 . Maternal mortality in a setting like Luanda depends on much more than the medical service per se and outcome indicators rarely help in identifying which problems that most urgently need to be addressed. It has been shown that less than 50% of women in Luanda give birth in institutions (UNICEF, Angola: Studies on Extra-Institutional Deliveries in the Province of Luanda, 1997), which implies that the obstetrical outcome of every second pregnancy is likely not to be included in the official statistics. Attention has therefore gradually focused more on process indicators for the assessment of quality of health service and for analysis of the different links in the chain of obstetric care. It would be unwise to view process and outcome measurements as competing with each other; rather it is a matter of circumstances which indicator is regarded most useful3 . In a more focused perspective, like evaluating the quality of a referral system, process indicators are more relevant. Time is often of crucial importance in obstetric emergencies. The different factors that constitute impediments for rapid treatment have been schematically presented as “the three delays”4 . This stepwise model offers a pedagogic analysis of reasons for postponement of treatment in various contexts and is also applicable for referrals of obstetric emergencies from one level of care to another. The purpose of this study was to evaluate the efficacy of the newly established network of peripheral birth units and their relation to the hospitals. By auditing various aspects of emergency obstetric referrals at two different times and by letting the discussions and conclusions from the first study effect the second, we aimed at elucidating the potential impact of audit on quality of care, giving an example of a clinical “audit cycle”5,6 . Materials and Methods Three SPPs were selected for the study: Cazenga (C), Palanca (P) and Sambizanga (S). These were included of practical reasons as they are all situated relatively close to the hospitals at a distance of between two and six km. We postulated that this would result in high compliance to referral advice and a similar time for transport. The first part of the study took place between April 23 and July 24 in 1996 and included 157 women referred for obstetric emergencies. The chief midwife of each SPP had an established routine of monthly visits to the hospitals to which they had referred patients for collection of records. The frequency of these visits was increased to enable data collection on a weekly basis for the SPPs included in the study. Records were brought to the study group consisting of six midwives and one of the authors (PC) for analysis according to a study protocol. Diagnosis and treatment provided were registered. Besides outcome indicators of maternal and neonatal deaths, process indicators of waiting time, over all case fatality rate, Caesarean section rate and partogramme quality were studied. Transport and waiting time is central in referring obstetric emergencies and partogrammes had recently been introduced as an obstetric tool and were evaluated according to a list of criteria and subdivided into categories of good, acceptable or poor quality. A good quality partogramme should have relevant information on birth protocols and information on fetal heart rate, rupture of membranes, cervical dilatation at least every 4th hour, station of presenting part at least every 4th hour, blood pressure, time of birth, time of placental expulsion and Apgar score. With three or more of these items missing, the partogramme was considered of bad quality. In the following audit sessions, the organisational deficiencies of the referral system disclosed and the incompleteness of records and data were presented, analysed and discussed at two local seminars. A majority of doctors and midwives employed in institutional obstetric care in Luanda participated. Emphasis was put on further education in the use of partogrammes. Courses for midwives and doctors were implemented at both the hospitals and the SPPs. The WHO material on the partogramme7 was translated into Portuguese, distributed and explained during these lectures. The second part of the study comprised 92 referrals from the same SPPs between Dec 1, 1998 and Feb 28, 1999. During this part, the chief midwives of the two hospitals were also engaged in the study. The records of referred patients, which they had retrieved, were returned to the responsible midwives of the SPPs twice weekly. These records were then analysed every second week by the study group, using the same study protocol as in the previous collection of data. Ethical approval had been granted by the two local maternities and by Karolinska Institutet, Stockholm, Sweden. For statistical analysis EpiInfo 2000 software program has been used. Results The total number of births and referrals admitted to hospitals during the two study periods are presented in Table 1. The proportion of referrals differed widely between the SPPs; from 1.7% in Palanca in May 1996 to 28.7% in Cazenga in January, 1999. Basic obstetric data. Mean age was 24.1 years in both periods of the study. Young women, primiparous and grand multiparous women are among categories usually regarded at high risk of pregnancy complications. Women < 20 years of age constituted 36%, primiparous women 43% and grand multiparous women (≥ 4 previous births) 32% in the first period. The corresponding figures in second period were 29%, 40% and 22% respectively. These differences are not statistically significant. Diagnosis. In both periods the most common reason for referral was prolonged labour. The diagnostic alternatives in the first study protocol resulted in a large category called “other diagnosis”. In order to get a more differentiated picture, the list of alternatives was extended in the second period and some categories were subdivided into more specific diagnoses. Some women were also referred with more than one diagnosis (Table 2). The agreement on diagnosis at the SPPs and the hospitals was almost total in the second period of the study. In only two cases did they differ; one was diagnosed as foetal distress but turned out to be a normal birth, the other was a missed diagnosis of a twin pregnancy. In the first period records were too incomplete to make a meaningful comparison of diagnosis. Waiting time. The first period of the study demonstrated a mean waiting time of 13.7 hours from admission to hospital to first evaluation by a doctor. During the audit this question was much discussed and it was decided that referred patients should be seen with highest priority at the hospitals and not have to join the waiting line together with other patients. In the second period waiting time was studied more in detail. Mean transport time from the peripheral unit to the central hospital was 36 min (range 15-225 min). After arrival to the hospital, mean waiting time to see a midwife was 9 minutes and to the first evaluation by a doctor 71 minutes (range 0-510 min). This mean waiting time was 54 minutes at MAN (where 5 of the patients were met immediately at arrival by a doctor and 59% had to wait for less than 30 minutes) and 71 minutes at MLP (57% waited < 30 min). The mean total time from leaving the SPP to first assessment by a doctor was 104 minutes (range 15-570 min). With virtually the same transport time, mean total time was 92 minutes at MAN, compared to 108 minutes at MLP, but this difference is not statistically significant. Treatment The receiving hospitals had developed a more active stand regarding admission and treatment of referred patients after the audit. In the first period Caesarean section (CS) was performed in 13% of referred cases, uterotonic treatment was used in 15% and vacuum extraction in 2%. The corresponding figures for the second period were 30%, 24% and 4%, respectively. Only the difference in CS is statistically significant (p<0.005). The proportion of referred women who were left with neither medical evaluation nor treatment mentioned in the patients´ records decreased from 45% in the first period to 27% in the second (p=0.007). Partogrammes The quality of partogrammes differed to the advantage of the SPPs when compared to the overburdened delivery wards of the hospitals at both periods of the study. The poor partogramme quality of hospitals disclosed at the audit initiated further education in the proper use of partogrammes. This was reflected in the second period with a significant increase in quality over time at both levels (Table 3). Outcome In the first period there were 27 deaths among the traced 157 referrals, giving an over-all case fatality rate of 17.8%. In the second period no maternal death was registered. Foetal outcome was not addressed properly in the first period. In the second period, there were eleven stillbirths (12.0%). After the completion of the study, it was found in the books of the SPPs that during the first period 398 women were registered as “referrals”. The corresponding figure for the second period was 429. Thus, the 157 and 92 women who could be traced at the hospitals constituted only a minority of all women registered as referrals (39.4% and 21.4%, respectively). Only these could be included in the analysis above. Discussion In this study we have demonstrated a substantial improvement of quality of care over time regarding referrals of obstetric emergencies along with efforts to sensitise staff both in the referring and the admitting health units. By using the results of the first study for a clinical audit, sub-standard care with long waiting times, poor quality partogrammes and high mortality figures were revealed and provoked a challenge for improvement. Special areas of concern were identified and after a partogramme education programme, a second data collection took place. A dramatically reduced waiting time, an improved vigilance with use of partogrammes and a more proactive stand by the hospitals, all helped in reducing the maternal mortality to zero in the second study period. With the deplorable results in the first data collection, an improvement was to be expected by the mere focusing on the problems. Even if an improvement could be expected, this simple example of feedback nevertheless illustrates the importance of audit of process indicators in clinical practice. A large proportion of women, who were registered as “referred” in the books at the SPPs were not possible to trace at the hospitals. One explanation could be the unacceptably high referral rate at Cazenga. Many of the referred women from there were probably not really in an emergency situation and were not motivated to continue to the hospital. It could be argued that this loss to followup disqualifies the above findings since they are based on traced referrals only. This is however an inherent problem when studying referrals of obstetric complications in many African settings. Similar figures have been reported from e g Tanzania, Morocco and Ghana8, 9, 10 . (Recently even the well conducted Magpie on magnesium sulphate treatment reported over 30% loss to follow up11, 12 ). The technical aspects of referrals may be too narrow a focus since the number of non-traced persons gives rise to further questions. In resource-scarce settings like the current one, patients may feel forced to base their decisions not on what is medically sound, but on what is economically possible and culturally appropriate13 . Although many women in Luanda deliver without assistance, it should be recognised that the public medical services work in competition with alternative health systems. Our observations indicate that many of the referred women had preferred home birth with the help of a friend or a traditional birth attendant to a delivery in an overcrowded maternity ward. It has been shown that expert-defined risk has little influence on women’s decision to seek care. Apart from financial pressures, many women were found to fear discrimination and disrespect8 . Unfortunately these factors have a bearing also in Luanda where negative perceptions of the hospitals may make women hesitate to seek care and the demand for informal user-fees seems to breed a fatalistic attitude among birthing women: “From where will we take that kind of money? You stay home and hope for the best”14 . Prolonged labour was the single most common reason for referral in both periods. The two collections of data did not occur at the same time of the year. We therefore expected to find differences in reasons for referring. In the second study protocol we listed fifteen diagnostic alternatives but still did not register common severe diagnoses like malaria and jaundice. Referrals of obstetric emergencies have been the focus of several African studies during the past decade and obstructed/ prolonged labour is repeatedly one of the main indications15, 16 . In the study from Burkina Faso15 maternal mortality increased proportionally with the distance to the hospital, which illustrates one of the “delays” in obstetric care4 . The emphasis put on partogramme education and the decision to give highest priority at the hospitals to referred women were crucial for the final results. There is no doubt that the partogramme has meant dramatic improvement in the perception of the birthing process in countries where no such notion was present before17 . In the time study, we have been mainly concerned with the duration of transport and the “admission to treatment interval”. Few such studies have been published previously but a reduction of the same magnitude as in this paper has been demonstrated for women with obstetric complications from some other African settings. In a general hospital in Nigeria, a mean interval of 11 hours decreased to 1.5 hours after intervention18 . At a teaching hospital, the same team could demonstrate a reduction in both waiting time (from 3.7 hours to 1.6) and overall case fatality rate (by 21%)19 . “Decision to delivery interval” has recently been reported in a paper from Abidjan among cases of life-threatening obstetric emergencies (with a median time of 4.8 h and 2.8 h respectively from the two hospitals studied)20 . Routine records in low-income countries are often too poor in information to allow for analysis of time of decision-making and have not been included in this paper. We have, however, in a previous paper on uterine ruptures in Luanda addressed the “decision to delivery interval” (Strand RT, Tumba P, Niekowal N, Bergström S. Audit of cases with uterine rupture: a process indicator of obstetric care, 2009. Unpublished). Although there are reasons to assume that regular audits have to be repeated in order to ensure the improvement that has been achieved, in practical life this is often difficult. In their paper regarding audit of “near misses” from 12 hospitals in four African countries, Filippi et al reported failure of sustaining the audit practice in a majority of hospitals after the end of their project and identified several important factors for a successful implementation of audit21 . Approaches on how to carry out the revolving cycle of re-evaluation vary from informal discussions of selected cases to structured reviews of large number of cases using statistical analysis. The criterion-based clinical audit is an example of the latter, quantitative, method monitoring the extent to which different complications are treated according to a set of explicit criteria22 . This would yield a case fatality rate for each complication instead of the overall case fatality rate, which we have used here. In conclusion, audit of referrals of obstetric emergencies addresses a process indicator of great importance. Delays between care provided at a peripheral unit and admission at the receiving hospital can be identified and the reasons elucidated and acted upon. This study has shown a dramatic shortening of waiting time, an increase in CS rate, high agreement in diagnosis between peripheral and central units as well as an increased quality of partogrammes. In spite of the statistical limitations of this study, we cautiously interpret the findings as signs of an improved quality of care regarding the referral of obstetric emergencies in Luanda during the periods studied. Future studies also need to include factors affecting patients´ reluctance of being referred. Acknowledgements We would like to thank all midwives involved in collecting the patients´ records that form the basis for this paper. We appreciate the participation of midwives and doctors in the discussions during the audit sessions and their flexibility and willingness to improve what is documented in this study. Special thanks to Dr Peter Beck-Larsen, who was a driving force in the first part of the study. We would also like to address the Department for Research Cooperation, SAREC, Swedish International Development Cooperation Agency (Sida), Stockholm, Sweden with gratitude for economical support. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09024t2.jpg] [rh09024t1.jpg] [rh09024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}