 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
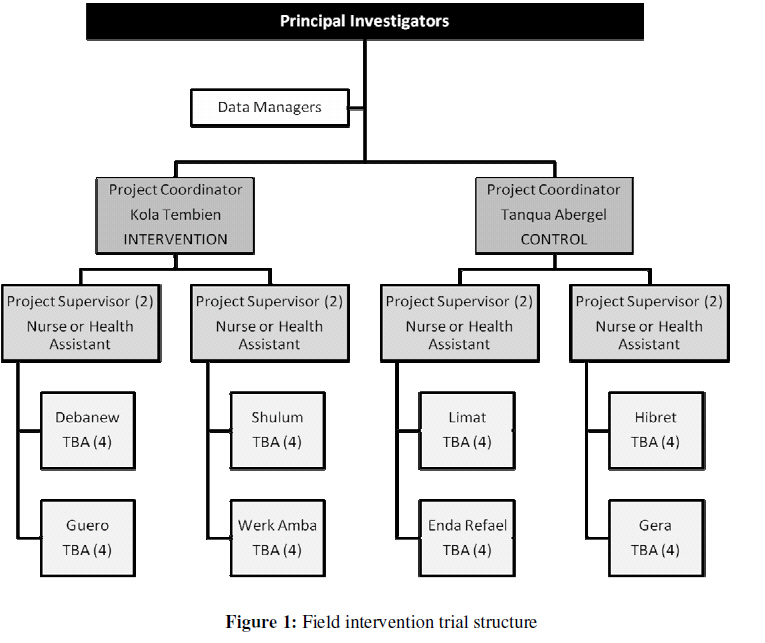
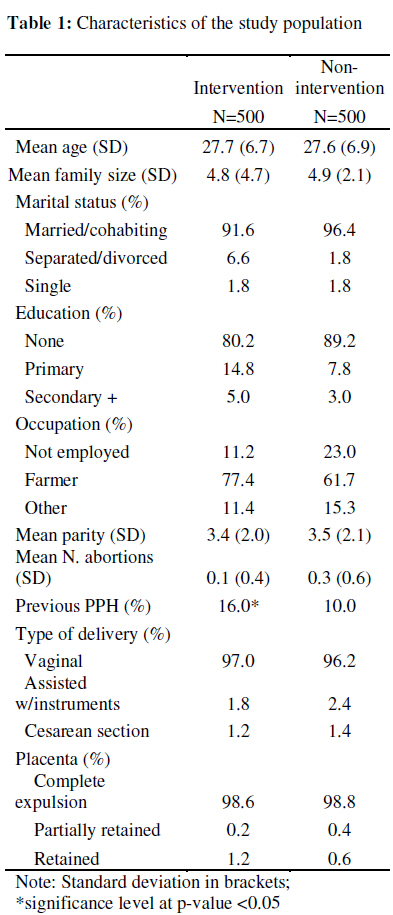
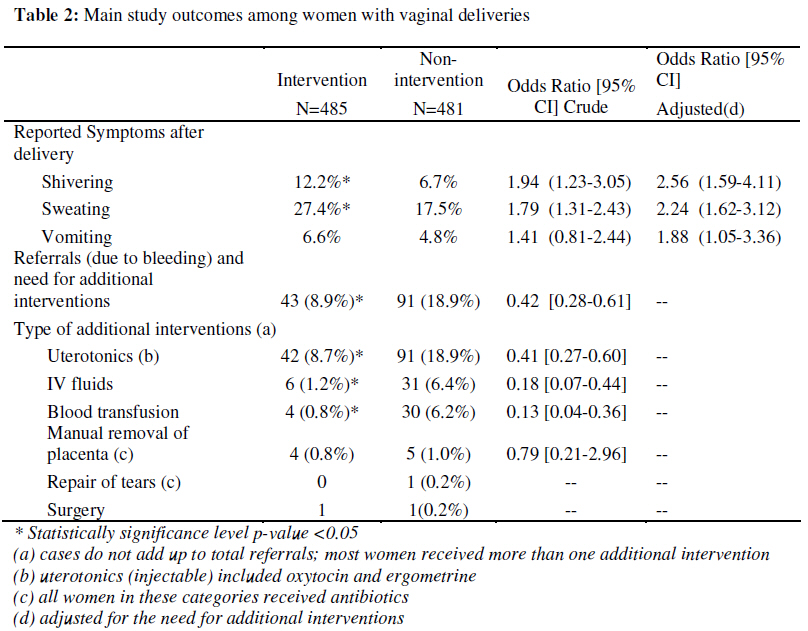
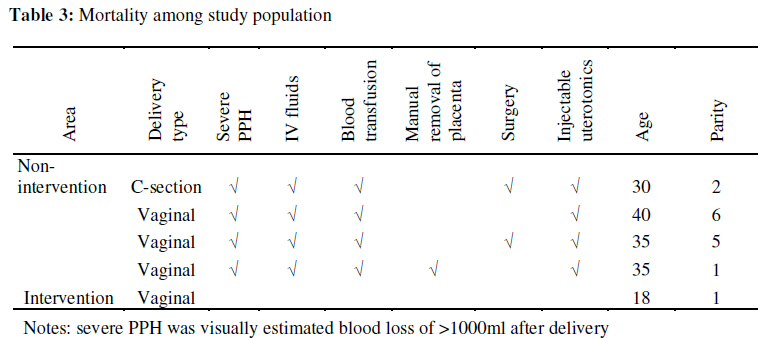
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 87-95 Original research article Prevention of Postpartum Hemorrhage: Options for Home Births in Rural Ethiopia La prévention de l’hémorragie du post-partum: options pour les naissances à domicile en Ethiopie ruraleN. Prata1*, A. Gessessew2, A. K. Abraha3, M. Holston4, M. Potts5 1Bixby Center for Population, Health and Sustainability, University of California, Berkeley, School of Public Health, 229 University Hall, Berkeley, CA 94720; 2Mekele University Hospital, College of Health Sciences; 3Tigray Health Bureau. Mekele, Tigray; 4Venture Strategies for Health and Development; 5Bixby Center for Population, Health and Sustainability, University of California, Berkeley, School of Public Health Code Number: rh09025 ABSTRACT This paper sought to determine the safety and feasibility of home-based prophylaxis of postpartum hemorrhage (PPH) with misoprostol, including assessment of the need for referrals and additional interventions. In rural Tigray, Ethiopia, traditional birth attendants (TBAs) in intervention areas were trained to administer 600mcg of oral misoprostol. In non-intervention areas women were referred to the nearest health facility. Of the 966 vaginal deliveries attended by TBAs, only 8.9% of those who took misoprostol prophylactically (n=485) needed additional intervention due to excessive bleeding compared to 18.9% of those who did not take misoprostol (n=481).The experience of symptoms among those who used misoprostol can be considered of minor relevance and self-contained. This study found that prophylactic use of misoprostol in home births is a safe and feasible intervention. Community health care workers trained in its use can correctly and effectively administer misoprostol and be a champion in reducing PPH morbidity and mortality (Afr J Reprod Health 2009; 13[2]:87-95). RĖSUMĖ Cette étude avait pour objectif de déterminer la sauveté et la faisabilité de la prophylaxie adaptée localement de l’hémorragie du post-partum (PHP) à l’aide de misoprostol, y compris l’évaluation de la nécessité des orientations vers les spécialistes et des interventions supplémentaires. A Tigray, en Ethiope, les sages-femmes traditionnelles (SFT) dans les régions de l’intervention ont été formées pour administrer 600 mcg de misoprostol par voie orale. Dans les régions où il n’y pas d’intervention, on a orienté les femmes vers un établissement de santé le plus proche. Sur les 996 accouchements par voie vaginale que les SFT ont fait accoucher, seul 8,9% de celles qui ont pris misoprostol prophylactiquement (n=485) avaient besoin d’une intervention supplémentaire à cause de l’hémorragie excessive par rapport à 18,9% de celles qui n’ont pas pris misoprostol (n=481). L’expérience de celles qui ont pris misoprostol ne peut pas être considérée come étant d’une pertinence mineure ou autonome. Cette étude a découvert que l’emploi prophylactique de misoprostol dans les accouchements à domicile est une intervention sans danger et faisable. Les membres du personnel soignant de la communauté qui ont été formés de la manière de l’employer, peuvent administrer misoprostol effectivement et de bonne manière et peuvent être des champions dans la réduction de la morbidité et la mortalité de la PHP (Afr J Reprod Health 2009; 13[2]:87-95). KEYWORDS: Misoprostol; postpartum hemorrhage; traditional birth attendants (TBAs) Introduction Despite having an effective means for both prevention and treatment, postpartum hemorrhage (PPH) continues to be the leading cause of maternal mortality worldwide.1 Although women experience PPH at similar rates across the globe, the burden of maternal death due to PPH weighs most heavily in developing countries, associated with a third of maternal deaths in Africa.2 Developing countries lack the necessary drugs and skilled attendance at delivery to prevent PPH and subsequent maternal deaths. Currently, oxytocin is the uterotonic of choice for the Active Management of Third Stage Labor (AMTSL), recommended by the World Health Organization (WHO) to prevent postpartum blood loss.3 Oxytocin requires both administration by injection and refrigeration, rendering it infeasible in resource-poor settings where the majority of women deliver at home without a skilled provider. Ethiopia is a case in point: country-wide, delivery in a health facility is the exception rather than the rule (6% of births).4 Almost all of these facility births occur in urban areas: children born in urban areas are 20 times more likely to be delivered in a health facility than those born in rural areas. 4 Ethiopia ranks fifth in the world in the number of maternal deaths, given its high maternal mortality rate (673 deaths per 100,000 live births)4 and large population. In settings such as this, strategies of reducing the risk of PPH at home births are urgently needed. Misoprostol is a proven uterotonic increasingly used in obstetrical and gynecological practice including the control of PPH.5-7 An inexpensive tablet, it is easy to store, stable in field conditions, and has an excellent safety profile with multiple routes of administration.8 FIGO/ICM jointly recommended that in home births without a skilled attendant, misoprostol may be the only available technology to control PPH9 and the WHO has recommended that in the absence of AMTSL, misoprostol should be offered by a health worker trained in its use for PPH prevention.10 Indeed, several other community-level studies have shown the program-effectiveness and safety of using misoprostol to control PPH at home births.11-14 The purpose of this paper is to present results of an intervention trial conducted in the Tigray region of Ethiopia, focusing on the safety of misoprostol for prophylaxis of PPH at home births attended by TBAs. In addition, we assessed the prevalence of referrals due to bleeding and additional interventions required. Methods A field intervention trial was carried out in rural villages of Tigray from July 2005 to January 2007. Figure 1 shows the trial structure. All TBAs participating in the study are respected members of their community and working as TBAs with the local health authorities for more than a decade, delivering between 3-5 babies a month. All were previously trained to conduct clean delivery and identify and refer complications, and in addition to report their activities to the local health facility. Prior to study implementation the research team conducted focus groups discussions (all TBAs in groups of 1012) and in-depth interviews with selected TBAs to assess knowledge, attitudes, and practices related to delivery, blood loss awareness and measurement, ability to follow study protocol, and patient referral requirements. TBAs were trained according to study protocol for intervention and nonintervention areas. Intervention TBAs administered 600 mcg of oral misoprostol (3 tablets, Sigma Pharmaceutical, Cairo, Egypt) immediately after delivery of the baby; in the case of twin pregnancy, after delivery of the second twin. Nonintervention TBAs continued their current practice of identifying danger signs and immediately referring the patient to a health facility. The level of supervision and data collected was identical in both intervention and nonintervention areas. In the study villages women do not use any form of blood loss measurement after delivery. Bleeding is expected and is associated with cleansing. Therefore, implementing a system to measure blood loss was not practical. TBAs in both areas were trained to monitor blood loss, pulse, respiration and signs of general weakness of the parturient. All TBAs also received extensive training in visual perception of approximate 500ml and 1000ml of blood loss. Even though inaccuracies exist with visual estimation, it is preferable to underestimate blood loss at home, transfer immediately, and let the skilled health provider evaluate and administer treatment accordingly if necessary, rather than waiting too long to seek assistance. TBAs were instructed to refer all women with partial or complete retention of the placenta (placenta not delivered within 20-30 min of birth), or women with any sign of weakness or deterioration of status after delivery regardless of the reason. Referral centers within village reach included basic and comprehensive emergency obstetric care. TBAs were instructed to accompany the parturient to the health facility. Transportation costs when needed were covered by the project. At the health facility, the provider completed the data collection tool initiated by the TBA by recording all interventions given to the woman, including her condition at discharge and condition of the neonate. A maternal mortality audit was conducted to account for all maternal deaths in the project villages. PIs conducted verbal autopsy in cases where the death occurred at home and cause of death was unclear. All forms were checked for accuracy and entered in an SPSS database. Analysis was performed with Stata/IC version 10 (Calverton, MD, USA). The study was approved by the University of California, Berkeley Committee for Protection of Human Subjects (CPHS#2005-6-9), and the Tigray Health Bureau. Results A total of 1000 women were recruited and enrolled in the study, equally divided between intervention and nonintervention areas. Table 1 shows the socio-demographic and obstetric history of the study participants by area of intervention. Women from both areas present similar socio-demographic characteristics. However, women in the intervention areas reported previous experience of PPH more frequently. A total of 34 women were withdrawn from the study because they did not have a vaginal delivery at home. The main outcomes of the study refer only to the 966 women (485 in intervention and 481 in nonintervention areas) who had a vaginal delivery at home assisted by a TBA (Table 2). Safety of the intervention was assessed by comparing the frequency of reported symptoms after delivery between the two study areas; the need for further treatment for these symptoms; and the report of serious adverse events due to failure to follow study protocol. Table 2 shows that the most commonly reported symptom after delivery was sweating, significantly higher in the intervention group (27.5% vs. 17.5%). Shivering was also significantly more reported in the intervention area (12.2% vs. 6.7%). Even after adjusting for receipt of additional treatment due to excessive bleeding, the odds ratios for shivering and sweating remained significantly higher in the intervention areas. Report of vomiting was not significantly different between the areas. However, when adjusted for those who had received interventions for excessive bleeding, women in non-intervention areas were significantly less likely to report vomiting (OR 1.88 95% CI 1.05-3.36). Less than 5% of women in both areas reported fever, a symptom commonly reported after intake of misoprostol. However, in this study fever was reported as perceived raised body temperature, not measured with a thermometer. No woman was referred to a health facility due to these symptoms in either area; symptoms were well managed at the household level without the need for further treatment. Women in intervention areas were significantly less likely to be referred for additional treatment related to excessive bleeding (8.9%) compared to women in non-intervention areas (18.9%), (OR 0.42 95% CI 0.28-0.61). Among all referrals due to bleeding, all but one woman (from the intervention area) received an injectable uterotonic drug (oxytocin or ergometrine) as additional intervention. Of those who received any additional intervention, 6.2% of women from nonintervention areas received blood transfusion, compared to less that 1% of women in the intervention area (OR 0.13 95% CI 0.04-0.36). The need for manual removal of placenta was not significantly different between the areas. Only one woman (non-intervention) needed repair of tears and another one needed surgery. During the study period a total of 5 maternal deaths occurred (Table 3). This was expected; given the maternal mortality ratio in Ethiopia, we were anticipating 7 maternal deaths. None of the deaths were due to misuse of misoprostol nor could in any way be linked to the drug. All of the deaths in the non-intervention area occurred at the health facility (3 of the deliveries started at home), so the cause of death was known. The only death that occurred in the intervention area was a patient that enrolled in the study, took misoprostol, did not have PPH, was not transferred after delivery, but was reported dead during puerperium. Verbal autopsy investigation revealed that the patient was HIV positive, deteriorated very rapidly after delivery, and died at home. It is important to note that the study protocol exclusion criteria included any woman with a chronic disease. However, existing stigma around HIV/AIDS prevents many patients for telling their providers their HIV status and this case was no exception. The TBA attending the delivery was not informed of the patient’s HIV status. Discussion This study demonstrated that household prophylaxis of PPH with 600 mcg of misoprostol is a safe intervention at the community level to prevent PPH at home births in rural areas where women have limited access to health care. The TBAs in Tigray demonstrated that they could safely administer misoprostol for PPH prevention, as evidenced by their ability to manage symptoms of the drug’s use at the home, the reduced number of referrals in the intervention area, and the absence of serious adverse events due to deviation from study protocol by TBAs. Evidence from this study can be used to inform policy decision-makers in Ethiopia and other areas with similarly high rates of home deliveries without skilled attendance on how best to protect women delivering at home. Women who took misoprostol were significantly more likely to experience shivering and sweating compared to nonusers. While these symptoms are commonly experienced among women who take misoprostol, 15 they are also common among all women who deliver, and are minor in comparison to the effects and possible consequences of excessive bleeding. The experience of symptoms after childbirth among those who used misoprostol can therefore be considered of minor relevance. Prophylactic use of misoprostol in the intervention areas reduced the rate of bleeding-related referrals by more than half and dramatically decreased the need for additional interventions. Reducing both referrals and the need for interventions not only lessens the burden of maternal death and morbidity due to PPH, but also relieves the overtaxed health care system. There was no standardized method of measuring postpartum blood loss in this study; it was proven to be infeasible. We cannot know for certain the true number of PPH cases in this study, except for those that needed and received additional interventions to treat excessive bleeding. Waiting for recognition of PPH in the absence of a culturally-appropriate, standardized method of measuring postpartum blood loss may delay seeking care and increase risk of death. In such circumstances, misoprostol as prophylaxis for PPH could be integral to decreasing PPH-related morbidity and mortality and reducing costs to the health care system. It is imperative that safe motherhood programs direct their efforts to tackle the main cause of maternal mortality – PPH – wherever the births occur. In doing so, programs should aim to increase protected births. If we assume that facility births are protected because they are assisted by skilled providers and PPH can be reduced by using AMTSL with oxytocin, it is now time to focus on protecting births where most maternal deaths occur in developing countries – in the home. Where women deliver far from a health facility, they must be empowered with an effective means of preventing the leading cause of maternal death. This study adds to the growing body of literature showing that at the lowest level of the health care system – community health care workers, such as TBAs, and even the mother herself – can and should use misoprostol in home births to prevent PPH. Only by deploying proven technologies such as misoprostol to protect the births at home can we hope to increase the coverage of protected births and decrease PPH morbidity and mortality. Other efforts to increase skilled assisted births should continue, but given the slow progress in developing countries, an interim measure such as this can have an immediate impact in helping poor women in rural areas for which skilled attendance is a distant dream. Acknowledgements The authors would like to thank Dr. Gebreab Barnabas, Head of the Tigray Health Bureau, for his support; Abraham Kahsay for his help with data management; the health care professionals at the Tanqua Aberguel and Kola Tembien Woredas; all traditional birth attendants that gave their time and invaluable insights into the knowledge, attitudes, and delivery practices of the communities they serve; and to all women that accepted to participate in the project, without them this study would not have been possible. We would also like to thank Venture Strategies for Health and Development who financially supported the study. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09025t3.jpg] [rh09025t2.jpg] [rh09025f1.jpg] [rh09025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}