 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
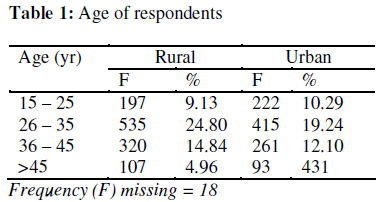
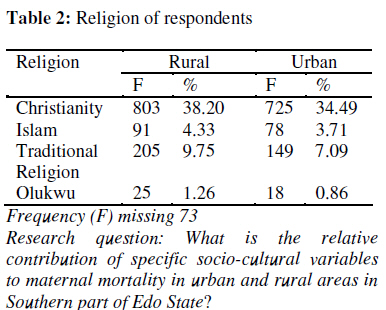
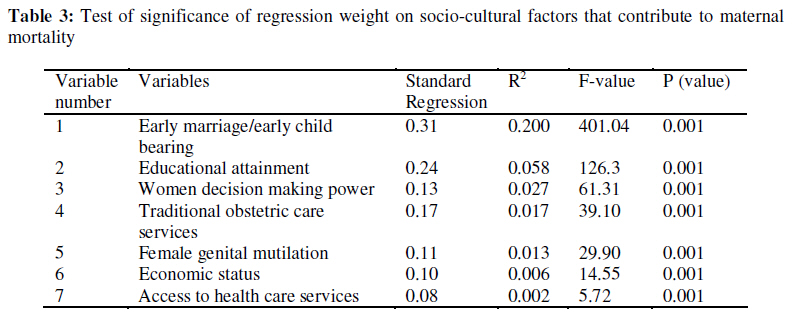
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 109-115 Original research article Relative Contributions of Socio-Cultural Variables to the Prediction of Maternal Mortality in Edo South Senatorial District, Nigeria Contributions relatives des variables socio-culturels à la prédiction de la mortalité maternelle dans le district sénatorial du sud de l’état d’Edo, NigériaChinwe Lucy Marchie, Francisca Chika Anyanwu2 1 School of Nursing, University of Benin Teaching Hospital, Benin City, Edo State; 2 Department of Human Kinetics and Health Education, University of Ibadan, Ibadan. Code Number: rh09027 ABSTRACT The study examined the extent of contributions of socio-cultural factors to maternal mortality (through survey method). Two thousand one hundred and fifty seven (2,157) females of reproductive age were selected using multi-stage sampling technique. The instrument was a self developed structured and validated questionnaire with a reliability of 0.82. Focus Group Discussion (FGD) and In-depth interview guide were used to complement the instrument. Inferential statistics of multiple regression was employed to test the hypothesis at 0.05 level of significance. The result showed that the most relevant variables across the two locations (rural and urban) was early marriage/early child bearing (R2 = 0.200; F = 401.40; P = 0.001) followed by educational attainment. Others in descending order were: women decision making power; traditional obstetric care services; female genital mutilation ; economic status and access to health care service. This indicates the importance of formulating policies that would focus on attaining high level of literacy among girls (Afr J Reprod Health 2009; 13[2]:109-115). RĖSUMĖ L’étude a examiné l’importance des contributions des facteurs socio-culturels à la mortalité maternelle (à travers la méthode de l’enquête). Deux mille cent cinquante sept (2,157) femmes en âge d’avoir des enfants ont été sélectionnées à l’aide de la technique d’échantillage à stade multiple. L’instrument était une structure auto-développée et un questionnaire valide ayant une confiance de 0,82. L’instrument a été complété à l’aide des Discussions à Groupe Cible (DGC) et un guide des interviews en profondeur. Des statistiques déductives de la régression multiple ont été utilisées pour vérifier l’hypothèse à un niveau de signification de 0,05. Le résultat a montré les variables les plus pertinents a travers les deux milieux (rural et urbain) étaient le mariage précoce/l’accouchement précoce (R2 = 0,200 ; F= 401,40 ; P = 0,001) et ensuite l’acquis éducatif. Les autres d’un ordre descendant étaient : le pouvoir de la femme de prendre des décisions ; les services de soins obstétriques traditionnels ; la mutilation génitale féminine ; la situation économique et l’accès au service des soins médicaux. Ceci montre l’importance de la formulation des politiques qui mettront l’attention sur l’acquisition d’un haut niveau d’alphabétisation chez les filles (Afr J Reprod Health 2009; 13[2]:109-115). KEYWORDS: Socio-cultural, Edo South Senatorial District, maternal mortality, Edo State, Nigeria Introduction The incidence of maternal mortality has increased in many parts of the world including sub Saharan African region for a variety of socio-cultural reasons. Maternal mortality is defined as death of a woman while pregnant or within forty two days (or six weeks) of termination of that pregnancy regardless of the site, duration or outcome of the pregnancy or its management, but not from accidental causes. From the estimate, each year 585,000 women die from causes related to pregnancy and childbirth2 . Maternal mortality estimate for Nigeria, Africa’s most populous country, is among the highest in the world and it is put at between 800 and 1,500 deaths per 100,000 live births3 It was as a result of this rate that safe motherhood initiative (SMI) was officially launched at an international conference held in Nairobi, Kenya in 1987 and in Nigeria 1990. this was part of global goal to reduce maternal death by 50 percent by the year 2000. Since then awareness of the problem has been raised among policy makers, health professionals and the general public. The major reported causes of maternal deaths in developing world are severe bleeding, infections, obstructed or prolonged labour, unsafe abortion and hypertensive disorders of pregnancy especially eclampsia. Beside the health services, there are socio-cultural factors that contribute to maternal mortality and some of them, according to WHO are harmful traditional practices like female genital mutilation which could lead to prolonged and obstructed labour, due to adhesions. About four percent of maternal deaths have been attributed to such practices. Other socio-cultural problems include food restriction and taboo. In some cultures, pregnant women are not allowed to eat eggs so as to prevent their babies from being thieves when they grow up4 . They also identified another essential food nutrient like milk which pregnant women were not allowed to drink. This is to prevent the baby from being weakling or develop stealing tendency later in life. This study is based on the research questions, “What is the relative contribution of specific socio-cultural variables to maternal mortality in Edo South Senatorial District?” Methods The descriptive survey method was used for this study. The population was made up of all females of reproductive age who were married, all health workers and all relatives of women who died in pregnancy, labour and peuperium. There were seven Local Government Areas in Edo South Senatorial District, three were identified by the Independent National Electoral Commission to be predominantly urban and four predominantly rural5 . Using the simple random sampling technique, two Local Government Areas were chosen from the urban areas that formed the first cluster and two from the rural areas that formed the second cluster. The participants for the study were drawn from 44wards in the four Local Government areas selected and they were, Oredo(7wards), Ikpoba-Okha (6wards) and Ovia-North(6wards). Sixty percent of the wards were selected using proportional random sampling technique. In each participating ward, married women of reproductive age (1549years) were drawn as respondents using convenience sampling technique. A total number of two thousand one hundred and fifty seven urban and rural married women of reproductive age 1549years selected from the four Local Government Areas formed the sample for the study. There were tow interviews: health workers interview and interview for relatives of those who died in pregnancy, labour and peuperium. In all, 59 respondents participated in the study. Health workers interviews were conducted in the hospital/health centers/traditional birth attendant’s clinic, in the wards already selected for study and convenience sampling technique were also employed. Focus Group Discussion (FGD) was also conducted in the four Local Government areas used for the study namely Oredo, Ikpoba-Okha, Orhiomwon and Ovia-North. Community leaders were visited and briefed on the study and permission was sought to involve some community members in group discussions. Volunteers were invited to participate in the discussion. Forty eight participants were involved in the four FGD-two from urban and two from rural areas. The time, date and venue for discussions were specified to those who volunteered. Discussion group sessions were conducted with the investigator playing the role of the moderator. There was also a note taker and guard to prevent distraction during the course of the discussions. In al four sessions were held. In this study, we utilized a questionnaire (which was the main instrument), FGD and In-depth interview of health workers and relatives of the subjects. To ascertain reliability, the corrected version of the questionnaire was pre-tested by administering it to 200 adults of reproductive age from urban and rural areas of one Local Government Area outside the sampled ones. The data collected were correlated to estimate the reliability of the instrument using Cronbach’s coefficient (R), which produced an estimate of 0.82. Data Collection The researchers and ten research assistants administered the questionnaire on the respondents. The questions were also discussed and read out to the illiterate women in pidgin English/native language and their responses recorded on their behalf. The questionnaire were collected immediately after administration. Data Analysis Focus Group Discussion was transcribed and analyzed qualitatively. In-depth interviews were sorted and coded for computer analysis. The data collected were analyzed using Statistical Analytical System (SAS) mode. Descriptive statistics of frequencies were used to describe the demographic data. The inferential statistics of multiple regression was used to test the hypothesis at 0.05 level of significance. Results Table 1 presents the distribution of respondents based on their age category. From the table, the highest frequency was obtained from age range of 26-35years which had 534(24.8%) for rural area and 415(19.24%) for urban area. This was followed by the age range 35-45years, which had 320(14.8%) for rural and 261(12.1%) for urban. The age range 1525 was the third and made up of 197(9.13%) for rural and 222(10.29%) for urban, while age 45years and above was made up of only 107(4.96%) for rural and 93(4.31%) for urban. It can be concluded from the result that majority of the women in child bearing age were between the age range 26-35 years. Table 2 shows the religious inclination of respondents, most of who are Christians for both urban and rural areas. There is no significant difference between rural and urban with regards to religious inclinations. The result from Table 3 shows for each independent variable, the standardized regression weight (B), the F value and level at which the F value is significant at 0.05 level. As for the extent to which independent variables contributed to maternal mortality, the relevant variables across the two locations were early marriage/early child bearing; educational attainment, women decision making power, traditional obstetric care service, female genital mutilation, economic status and access to health care service. There was no attempt to compare responses among different groups of respondents. Data obtained were aggregates from respondents. Focus group discussions (FDG) were conducted at the beginning of the study, it gave the researchers comprehensive insight into the problem and the result was also used in fine-tuning the questionnaire which was the major instrument. The following, however is the trust of the interaction; views were consistent concerning the poor treatment of women in the society as obvious contributor to mothers death. The women also talked about having children early and for different men and not allowing them to take decision especially on where to go for treatment in emergency as a contributory factor to women dieing in pregnancy. Discussion The death of a woman in child birth is a tragedy and an unnecessary and wasteful event that carries a huge burden of grief and pain6 . They also stated that half a million women die each year due to pregnancy related complications and that 95% of them came from developing world. This study showed the extent to which each of the seven independent variables contributed to prediction of maternal mortality. The value of standard regression weights associated with the variables across the two locations (Urban and Rural) was early marriage/early bearing (R2 = 0.200; F = 401.04; P = 0.001), followed by educational attainment (R2= 0.058; F = 126.32; P = 0.001). The ranking in descending order were; women decision making power (R2 = 0.017; F = 39.10; P = 001); female genital mutilation (FGM) (R2 = 0.013; F = 29.90; P = 0.001), economic status (R2 = 0.006; F = 14.55; P = 0.001), and lastly access to health care services (R2 = 0.002; F = 5.72; P = 0.001). The results, showed clearly that all independent variables had positive contribution to the dependent variable of maternal mortality in Edo South Senatorial District at 0.05 alpha level. Death of a woman during pregnancy, labour and peuperium has been described as a major public health problem in developing countries7 . Studies carried out to find out possible causes of maternal mortality had different findings. A study of socio-cultural correlates of maternal mortality was considered to proffer solution to the problem. The result from the feeling of the women was that early marriage/early child bearing was the most important variable in the prediction of maternal mortality in Edo South Senatorial District. The results were largely supported by findings in Focus Group Discussion among women of reproductive age and in-depth interview on health workers and relatives of women who died in pregnancy, labour and peurperium. They emphatically identified early marriage/early child bearing as potent contributor of maternal mortality. There is a cultural belief in Benin that when a woman has a baby for a wealthy man, the baby will be at an advantage position in that particular family, where the inheritance of the father will be shared according to the number of children the man has. For this reason, according to Focus Group Discussion on women, a woman may have children for different men in order to acquire more inheritance when the man dies. Mothers therefore do not frown at their daughter who have children for married and nonmarried men because of the ‘gain’ they envisaged. This type of practice encourages early child bearing, which sometimes result in early marriage because in some cases the man may marry the girl eventually. This cultural phenomenon encourages “born for” syndrome, where a woman has children for different men. This finding therefore confirms the assertion that early marriage/early child bearing was the best contributor in the prediction of maternal mortality in Edo South Senatorial District. The result concretely reinforces findings of Inter-African Committee8 who observed that early marriage and child bearing were among the commonest practices found especially in the Northern part of Nigeria. The report additionally stated that early child baring could lead to cephalo-pelvic disproportion and subsequently prolonged and obstructed labour. The resultant effect of incontinence of urine and faeces due to continuous pressure on the vagina and bladder, which may make a woman to be withdrawn from the society. The woman may also suffer severe depression and infection and may eventually die. Also, in a study on maternal mortality among women in Heart province of Afghanistan, it was observed that the average age at which women get married was 15years, which contributed to high maternal death in the country9 . However, a contrary opinion was reported, and the argument was that maternal mortality among mothers of 35years and above was nearly three times higher than that of teenage mothers. This study was on the demographic, socio-economic and medical factors affecting maternal mortality in New Delhi, India10 . However most studies have shown that early marriage/early child bearing is a potent factor of maternal mortality and that young mothers have more risk of dying during childbirth11 . Another disadvantage of early child bearing includes girls losing out on schooling with few employment options. This result therefore affirms, the assertion of early child bearing as an effective predictor of maternal mortality. Conclusion Good reproductive health is a right of all women. In order to reduce reproductive health problems, quality services like good antenatal care should be made available, accessible and affordable in both urban and rural areas. It is therefore recommended that women should be encouraged and sensitized to be personally involved with their health and should be empowered to take prompt/early decision to seek medical care in emergency. Government should consciously put in place policies aimed at achieving basic level of literacy especially among girls and women in general. This could be achieved by building more functional schools and preferential scholarships for girls education. When young girls are effectively engaged in schools, early marriage/early child bearing, which is the potent contributor to maternal morality would be ultimately be less attractive. Acknowledgement We wish to express our gratitude to Prof. J. Akerele and Dr. U.A. Osunde for the editorial guidance. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09027t2.jpg] [rh09027t1.jpg] [rh09027t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}