 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
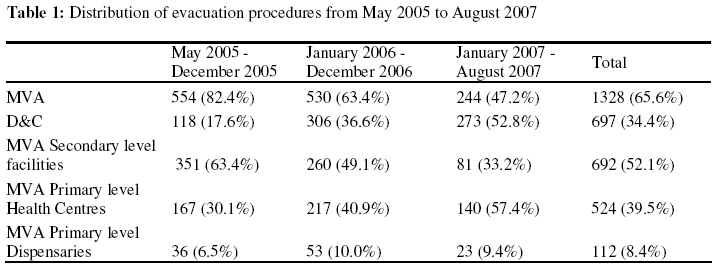
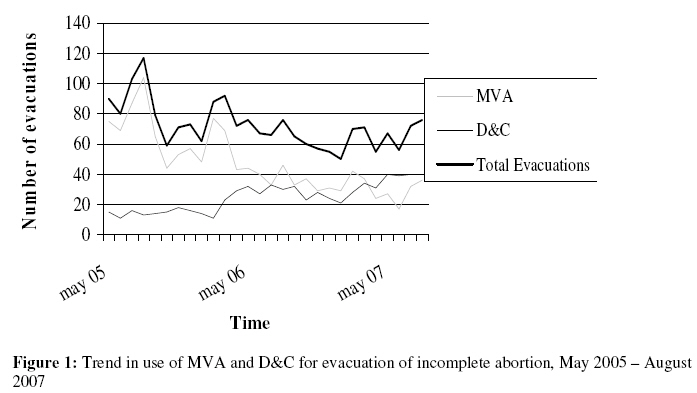
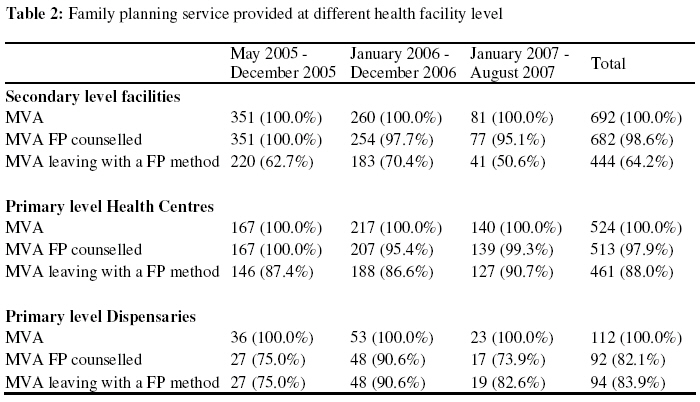
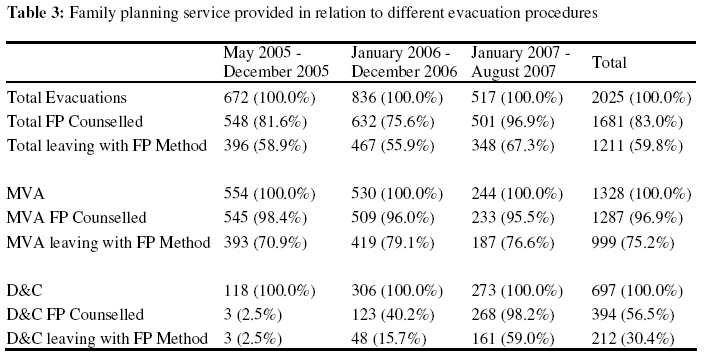
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 129-138 Original research article Expanding Comprehensive Postabortion Care to Primary Health Facilities in Geita District, Tanzania L’expansion due soin du post avortement compréhensif vers les établissements de la santé primaire dans le district de Geita, TanzanieKaroline Kragelund Nielsen1, Grace Lusiola2, Joseph Kanama2, Juliana Bantambya2, Nassor Kikumbih2, Vibeke Rasch1 1 University of Copenhagen, Denmark Code Number: rh09029 ABSTRACT A postabortion care program was implemented in 11 primary and secondary health facilities in rural Tanzania in order to decentralize comprehensive postabortion care to community level by upgrading midlevel providers to perform manual vacuum aspiration (MVA). Information about evacuation procedure and family planning (FP) service provided was obtained from the health facilities. In all, 2025 evacuations had been performed with MVA and D&C accounting for 65.6% and 34.4%, respectively. Among the women admitted with abortion complications, 59.8% left with a FP method. The proportion of women offered FP service differed by evacuation procedure, hence the proportion was higher among women evacuated by MVA. Upgrading midlevel providers to perform MVA is an efficient means to address the problem of unsafe abortion in rural areas. However, the sustainability of MVA service provision remains a challenge. Moreover, FP services should be offered to all postabortion clients regardless of evacuation procedure (Afr J Reprod Health 2009; 13[2]:129-138). RĖSUMĖ Un programme du soin du post-avortement a été mis en œuvre dans des établissements de la santé primaire et secondaire dans la Tanzanie rurale afin de décentraliser le soin du post-avortement compréhensif jusqu’au niveau de la communauté par l’augmentation de la performance des dispensateurs moyens pour qu’ils puisement faire l’avortement par aspiration manuelle (AAM). Le renseignement sur la procédure de l’évacuation et sur le service la planification familiale (PF) disponible était obtenu à partir des établissements de santé. En tout, 2025 évacuations ont été faits à travers AAM et le curetage de l’utérus étant responsable pour 65,6% et 34,4% respectivement. Parmi les femmes qui ont été admises avec des complications de l’avortement, 59,8% sont parties avec une méthode de la PF. La proportion des femmes qui ont profité des services de la PF était différente par la procédure de l’évacuation ; ainsi, la proportion était plus élevé chez les femmes qui ont subi l’évacuation par l’AAM. L’amélioration de la performance des dispensateurs moyens pour accomplir l’AAM est une manière efficace de s’occuper du problème de l’avortement dangereux dans les régions rurales. Toutefois, la capacité pour soutenir la dispensation des services de l’AAM reste un défi. De plus, les services de la PF doivent être offerts à toutes les clients du post-avortement sans considérer la procédure d’évacuation (Afr J Reprod Health 2009; 13[2] :129-138). KEYWORDS: Postabortion care; unsafe abortion; family planning; Tanzania; MVA; D&C Introduction Abortion-related complications are a major contributor to maternal mortality and morbidity, especially in Sub-Saharan Africa1 . In addition, incomplete abortion contributes significantly to the number of admissions in the gynaecological wards in many hospitals2 . In spite of a number of studies emphasizing the need for implementing comprehensive postabortion care and the world leaders agreement at the International Conference on Population and Development (ICPD) held in Cairo in 1994 to address the issues of abortions, only a restricted number of postabortion care programs have been implemented 3-6 . Most of these have been in urban settings and implemented at a regional level7 . However, it has been documented that there is a need for postabortion care at district and community level8 . Postabortion care programs aim at improving the management of abortion complications. This often includes replacing dilatation and curettage (D&C) with manual vacuum aspiration (MVA), and linking women to family planning (FP) counselling and services 9,10. Use of MVA for management of first trimester incomplete abortion has been found to be quicker to perform and less painful compared to D&C11 . Furthermore use of MVA over D&C reduces hospital costs 12 . In addition, it allows for services to be provided safely on an outpatient basis in decentralized locations by midlevel providers since it does not require electricity and is performed under local anaesthesia 5,13,14 . This is of great importance since a major barrier to providing postabortion care to women with incomplete abortions is lack of access to health facilities providing the service. Therefore it is evident that postabortion care is also implemented at the primary level 5,15,16. However, there is a tendency to equalize postabortion care with MVA. This is problematic since no matter how the postabortion care program is organized there will always be women who will need D&C e.g. women with incomplete second trimester abortion. Further lack of constant supplies of MVA kits as well as lack of chlorine solutions to clean the kits may also hamper the availability of MVA and consequently the providers may have to utilize D&C for evacuation instead of MVA. Thus postabortion care programs should be grasped as including both MVA and D&C as well as FP. As a result of a slow movement of comprehensive postabortion care from centralised public sector system to a decentralised district based approach, the majority of primarily rural women remain without adequate access to postabortion care. To address this problem, EngenderHealth initiated a comprehensive postabortion care (cPAC) program in 2005 which was implemented at primary and secondary level health facilities in Geita District, Tanzania. The Geita District is a remote rural area situated in the Mwanza Region near Lake Victoria. Before the program was implemented, postabortion care was only available at the District Hospital in Geita Town and the procedure offered was D&C. Training of service providers In April 2005 a cPAC training course was conducted for service providers working at health centres and dispensaries in the Geita District. The training involved service providers from 11 health facilities. Two of the facilities had doctors employed (in the following referred to as secondary level facilities), whereas health care services in the remaining 9 facilities, 6 health centres and 3 dispensaries, were provided by midlevel service providers (in the following referred to as primary level facilities). The aim of the training was to enable midlevel service providers working at secondary and primary health facilities to provide postabortion care, including counselling, emergency treatment of abortion complications and FP service. The training included theory in class and practical sessions at a district hospital. The training was competency based using a humanistic approach by practicing on female reproductive pelvic models before moving on to attend clients. Each participant developed a cPAC action plan specific to his/her facility that should serve as a guide for the implementation and form a basis for follow up and evaluation. Follow up visits were carried out in September 2005. These revealed that two of the dispensaries were not actively providing the cPAC service. At one of the dispensaries, the service provider trained in cPAC had left the facility shortly after the training sessions, thus, no MVAs was ever performed at the facility. At another of the three dispensaries the service provider did perform MVAs; however, in the first year after the training, none of the clients received FP counselling. The remaining 9 facilities were all actively providing the cPAC services included in the training. The two secondary level facilities are the only facilities that provide D&C. In case a woman attends one of the primary level facilities with incomplete abortion after the first trimester, the facility will refer her to one of the secondary level facilities for evacuation. In addition, women with severe complications are also referred to a secondary level facility. Methods Data collection The data were collected in October 2007 and covered a 28 months period (May 2005 -August 2007). All the 11 facilities, which had service providers participating in the training in May 2005, were visited and data of women admitted with incomplete abortion were collected. Data were obtained from the cPAC registration books at the sites. Moreover, at one of the secondary level facilities data on D&C clients were also collected from the registration books from the operating theatre. In total 2031 women with incomplete abortion were registered in the books. Information on evacuation procedure (MVA or D&C), FP service provided as well as reasons for referral was gathered. Results Use of MVA and D&C procedures From May 2005 to August 2007 a total of 2025 evacuations of incomplete abortion were performed in the Geita District (Table 1). Two-third of the evacuations were performed using MVA, whereas D&C accounted for the remaining onethird. Of the 1328 MVA procedures, almost half (47.9 %) were performed at primary level facilities, either in health centers or in dispensaries. The average number of MVAs performed, however, decreased over time. At the secondary level facilities, the average number of MVAs performed per month in 2005 was 43.9 (351 MVA/8 months) compared to 21.7 (260 MVA/12 months) in 2006 and 10.1 (81 MVA/8 months) in 2007. A similar trend of decreasing MVA procedures was observed at the primary level facilities although the alteration over time is smaller. Hence in 2005, 25.4 MVAs (203 MVA/8 months) were performed in average every month, the corresponding figures for 2006 and 2007 were 22.5 (270 MVAs/12 months) and 20.4 (163 MVAs/8 months). The trend of decreasing number of MVA procedures performed over time is also illustrated in figure 1, where it is shown that the number of MVAs reached the highest level in the first months after its introduction with a peak in August 2005 where 104 evacuations were performed. Thereafter the use of MVA gradually declined, reaching the lowest number of MVAs carried out in June 2007 with only 17 MVAs. The number of D&Cs performed compensated for the decrease in MVA procedures. Hence the number of D&Cs began to increase in 2006 and from April 2007 the number of D&C actually exceeded the number of MVAs. FP counselling and methods at different health facility level Regarding FP counselling, the proportion getting counselling at the dispensaries is lacking behind that of the health centres and secondary level facilities (Table 2). However, even though the secondary proportion is especially low in 2007 level facilities have the highest where only half of the MVA clients left proportion of MVA clients counselled, with a method although 95.5% received the facilities have the lowest proportion counselling. In comparison, at the health leaving with a FP method. The centres, where the proportion getting counselling is very close to that at the secondary level facilities, the proportion leaving with a method is much higher (90.7% in 2007) than at the secondary level facilities. Further, even at the dispensaries the proportion leaving with at method is quite similar to the fraction receiving counselling. Hence, the dispensaries also have a higher proportion of MVA clients leaving with a FP method compared to the secondary level facilities. FP counselling and methods among MVA and D&C clients Of the 2025 women admitted with incomplete abortion, 1681 (83.0%) received FP counselling and 1211 (59.8%) left the facility with a method (Table 3). However, the proportions differed from year to year with the proportion receiving counselling being highest in 2007 (96.9%) and lowest in 2006 (75.6%). Furthermore, there was a difference in the proportion leaving with a FP method with 67.3% in 2007 and 55.9% in 2006 being maximum and minimum. Looking exclusively at the MVA clients, the same tendency is not present. Altogether, almost all the women (96.9%), who had an MVA performed, received FP counselling and approximately 75% left with a method. The overall numbers for the D&C clients receiving FP counselling and service are somewhat lower, with 56.5% receiving counselling and less than one third leaving with a method. However, the proportion of D&C clients who received FP counselling increased quite significantly from 2.5% in 2005 to 98.2% in 2007, whereas the proportion leaving with a FP method rose from 2.5% in 2005 to 59.0% in 2007. Discussion A successful scale up of cPAC with increasing numbers of MVAs conducted at primary health facility level was observed. At secondary health facilities, however, the number of MVAs decreased and the number of D&Cs increased over time. Further problematic differences in FP service provision were observed between women treated with MVA and D&C, respectively. Close to half of all MVA procedures were performed at primary level facilities, either in health centres or in dispensaries. These findings add to the existing evidence that postabortion care can successfully be implemented at lower level health facilities 8,17,18 . It is increasingly being acknowledged that scaling up postabortion care to cover lower level health facilities should be a priority when aiming at addressing the problem of unsafe abortion17-19 . However in many low-income settings, postabortion care is still difficult to access in rural areas and women often have to travel a considerable distance to reach services. Such travelling requires time and money and may prevent women from accessing services. It is hoped that the results from the present study may inspire policy makers to scale up postabortion care to primary health care level, thereby making the service more available for rural women. The observed decline in the number of MVA procedures performed at secondary health level facilities may partly reflect the successful scale up of MVA service to cover primary level health centres. Another factor which likely also have contributed to the observed fall in MVA procedures over time is the increasing number of first trimester incomplete abortions being evacuated using D&C instead of MVA. This notion is supported by the fact that the number of MVAs primarily decreased at secondary level facilities. In contrast to this a study describing a program to scale up postabortion care in Guatemala found that during a period of 18 months the proportion of incomplete abortions evacuated with MVA inclined continuously20 . The explanation for this discrepancy might be the shorter program period and a more frequent use of follow up visits to the facilities in the Guatemalan study. Thus, it might be that without regular follow up visits the facilities will return to the procedure they are familiar with, namely D&C. Another explanation could be shortage of trained staff. Only 15 service providers were trained in the use of MVA making the system vulnerable to departure and transfer of staff. This was found to be the case at one of the dispensaries resulting in no evacuations performed at the facility. At the secondary level facilities, a similar situation might result in a switch from MVA to D&C, while the number of evacuations remains constant. FP counselling was offered to and accepted by 83.0% of the women with incomplete abortion. The proportion is similar to that found by other studies 20,21 . However, the proportion of women receiving counselling was substantially higher among the MVA clients compared to the D&C clients. This was mainly due to the majority of D&C clients not receiving counselling in the first 15 months. Yet, FP counselling is an essential element of postabortion care since it adds a preventive aspect to the service. Therefore, it is vital that not just MVA clients but also D&C clients receive FP counselling and service. Further, since first trimester incomplete abortions are best undertaken by MVA3 , D&C should whenever possible be reserved for second trimester abortions. However, since spontaneous abortions are uncommon after first trimester it could follow that, if used as recommended, the likelihood of the incomplete abortion stemming from an induced abortion was higher among D&C clients. Consequently the need for FP counselling would be more profound among D&C clients, making it ever more important to reach this group with counselling. Hence, in any case it is extremely problematic when D&C clients are not offered FP counselling to the same extend as MVA clients. The proportion leaving with a FP method was 59.8%. For the D&C clients the proportion leaving with a method increased over time. However, in the three years combined only 30.4% of D&C clients left with a FP method. In contrast 75.2% of MVA clients left the facility with a method. The proportion of MVA clients accepting a FP method corresponds to that found in another study among rural women in Tanzania and from other studies on postabortion care interventions20-22 . However, the proportion of MVA clients leaving with a method differs substantially between the different types of facilities, with 64.2% at the secondary level facilities and 88.0% at the health centres being minimum and maximum. With the secondary level facilities being the only one performing D&C, this could point to a general low rate of clients leaving with a method at this type of facility which might be explained by a higher level of work pressure. Even so the proportion of D&C clients leaving with a method is still significantly lower within the facilities. Moreover, this would not explain the discrepancy in the proportion getting FP counselling. There is a tendency to equalize cPAC with MVA, therefore in the beginning of the intervention period only MVA clients were provided with FP service. This problem was identified by the program managers in 2006 and it was stressed for the health staff that both D&C and MVA clients should be counselled and offered FP service. Hence, when implementing cPAC programs it is of paramount importance that the unmet need of FP is addressed among both MVA and D&C clients especially since there will be a need of D&C in case the women have past 12 gestational week, if MVA kits and chlorine solution is lacking or if staff trained to perform MVA is unavailable. Conclusion This study supports the line of papers that have shown the positive effect of postabortion care. It is possible to reach a high proportion of women with incomplete abortion receiving FP counselling and accepting a FP method. However, this study also shows that it is crucial to emphasize that postabortion care should not only include women undergoing MVA. The services must also be available and offered to D&C clients. Moreover, this study indicates, that when introducing a new method such as MVA it is important to conduct regular follow up visits and to ensure that a sufficient number of service providers are trained in the procedure. By taking these lessons learned from the Geita District into consideration, the implementation of future postabortion care programs could not only achieve high quality in emergency care of incomplete abortion but also avoid repeated abortions by high proportions of women counselled on FP and leaving the facilities with a method. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09029t1.jpg] [rh09029f1.jpg] [rh09029t2.jpg] [rh09029t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}