 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
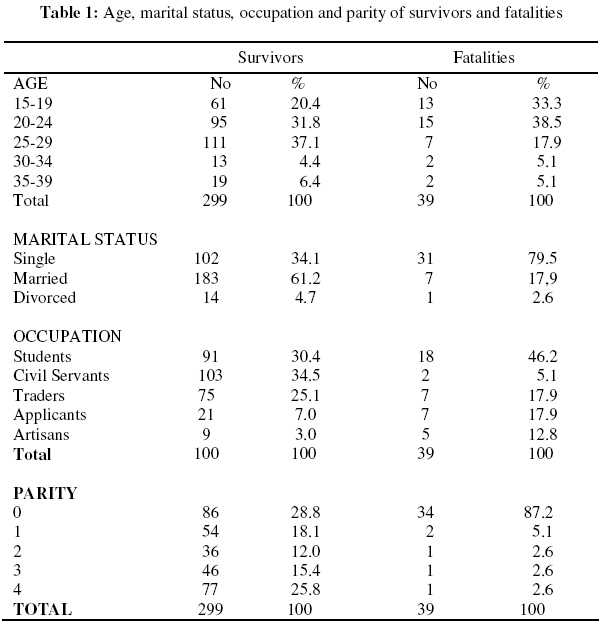
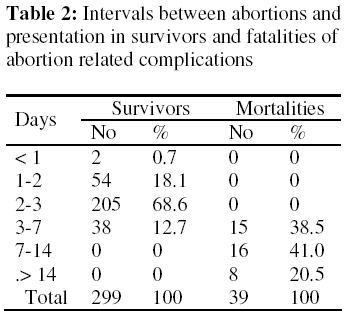
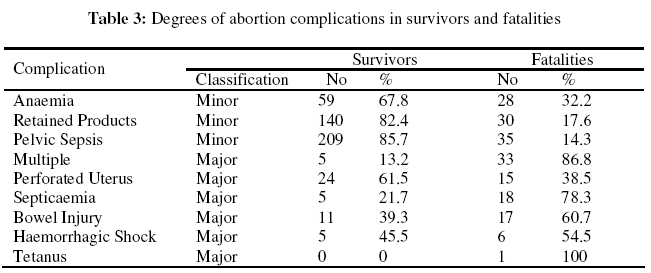
African Journal of Reproductive Health, Vol. 13, No. 2, June, 2009, pp. 139-146 Original research article Correlates of Abortion Related Maternal Mortality at the Lagos State University Teaching Hospital, Ikeja Corrélats de la mortalité maternelle liée à l’avortement à Lagos State University Teaching Hospital, Ikeja.Adetokunbo Olusegun Fabamwo, Oluwarotimi Ireti Akinola, Akpan Essien Akpan1 1Department of Obstetrics and Gynaecology, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria. Code Number: rh09030 ABSTRACT This study was carried out to highlight the probable correlates of mortality among patients managed for abortion related complications at the Lagos State University Teaching Hospital, Ikeja. All patients managed for abortion related complications between 1st January 2000 and 31st December 2003 were studied. Certain relevant socio demographic and clinical factors were compared among the survivors and fatalities. There were a total of 338 patients with abortion related complications. 299 survived while 39 died. Being single, nulliparous, of low educational status, presenting late and having major complications were significantly associated with mortality in this series. Encouragement of safe sex practices, increasing adolescents’ access to contraception, additional training of physicians and other appropriate heath workers in abortion care as well as the liberalisation of the restrictive abortion laws in Nigeria will go a long way in reducing abortion related mortality (Afr J Reprod Health 2009; 13[2]:139-146). RĖSUMĖ L’étude a été menée pour attirer l’attention sur les corrélats possibles de la mortalité chez les patientes qui reçoivent les traitements pour des complications liées à l’avortement à l’University of Lagos Teaching Hospital, Ikeja. Nous avons étudié les cas de toutes les patients qui recevaient des traitements pour des complications liées à l’avortement entre le 1e janvier 2000 et le 31 décembre 2003. Nous avons comparé certains facteurs démographiques et cliniques pertinents chez les survivants et les décès. En tout, il y avait 338 patientes qui avaient des complications liées à l’avortement. 299 ont surveçu alors que 39 étaient mortes, Dans ces séries, le fait d’être célibataire, nullipare, peu instruite, d’avoir présenté tard à l’hôpital et d’avoir des complications sérieuses ont été liés de manière significative à la mortalité. L’encouragement des pratiques sexuelles non dangereuses, la libéralisation de l’accès à la contraception par les adolescents, la formation davantage des médecins et d’autres dispensateurs de service de la santé par rapport des soins de l’avortement aussi bien que la libéralisation des lois restrictives contre l’avortement au Nigéria, aideraient d’une large mesure à réduire la mortalité lié à l’avortement (Afr J Reprod Health 2009; 13[2]:139-146). KEYWORDS: Abortion, fatality, Ikeja Introduction An abortion is when pregnancy is lost before the age of viability1 . It is known that about 15 – 17% of all pregnancies are complicated by spontaneous abortion, mainly in the first trimester2 . Induced abortion is an age old method of fertility control that had existed and had been practiced by different groups of people all over the world3 . Several reasons exist, medical, social or a combination of reasons and several methods or means can be employed to induce an abortion1,2 . Induced abortion frequently provokes sensitive reactions. Social, medical, political, religious, legal concerns exist and therefore many countries have formulated laws and policies that regulate its practice4 . A procedure for terminating an unwanted pregnancy by someone lacking the necessary skills or in an environment lacking minimal medical standards or both is referred to as unsafe abortion5 . In 2003, 48% of all abortions worldwide were unsafe and more than 97% of all unsafe abortions were in developing countries6 . In Africa, about 19 million cases of unsafe abortion occur annually3 . A large percentage of these unsafe abortions are performed by people least skilled to provide them4 . Over five million or approximately 1 in 4 women having an unsafe abortion is likely to face severe complications,which can cause death, and will seek hospital care, putting heavy demand on scarce resources7 . Every year about 20,000 Nigerian women die from complications of unsafe abortion. Few women have access to safe abortion in Nigeria because termination of pregnancy is illegal. It is only allowed to save the life of the woman and to preserve her physical and mental health. In addition two physicians are required to certify that the pregnancy poses a serious health to the life of the woman8 . This results in underground and clandestine performance of the procedure making it potentially unsafe and dangerous. This prospective study primarily sought to identify the correlates of mortality in cases of abortion related complications managed at the Lagos State University Teaching Hospital, Ikeja over a four year period. It also assessed how recent hospital-based abortionrelated mortality experiences in Nigeria compared to those from earlier studies. Methods Following the Ethical Committee approval, all admitted cases of induced abortion confirmed by the patients or accompanying relations and carried out in other facilities and with specific complications who were managed between 1st of January 2000 and 31st December 2003 at the Department of Obstetrics and Gynaecology of the Lagos State University Teaching Hospital, Ikeja, Lagos were recruited into the study. Cases of spontaneous abortions were excluded. Based on the outcomes of the standard management protocols applied, the study subjects were the patients who eventually died while under our care while the survivors served as controls. After obtaining informed consent from all patients, information on the age, marital status, occupation, parity, interval between procurement of abortion and arrival in hospital, complications, treatment modalities and outcome was obtained and entered into specially designed forms. The term “illiterate’ was used to describe subjects who had no formal education at all. Applicants are secondary school leavers with no definite work engagement. Civil servants are public service workers who must have attained a minimum of secondary level education. These parameters were compared in the survivors and the fatalities and subjected to statistical analysis using the Pearson’s chi-square test. This was in order to identify probable correlates of mortality in this series. Results There were 10,412 total births during the study period. There were a total of 338 cases of abortion in the four year period. Thirty nine of them died while 299 survived. There were 158 maternal deaths during the study period. Abortion related deaths accounted for 24.7% of all maternal deaths, the case fatality rate was 11.5% and the abortion mortality rate was 375 per 100,000. All abortion related deaths followed induced abortion. The age distributions of the survivors and fatalities are shown in Table 1.The majority of patients in both groups (89.3% of survivors and 89.7% of fatalities) fall within the 15 to 29 age range. Age distribution however did not have any statistically significant association with abortion mortality or survival (p = 0.143). Table 1 also shows the marital status of the two groups studied. Most of the survivors (61.2%) were married, while most of the fatalities (79.5%) were single. There was a statistically significant association between being married and surviving an abortion (p< 0.001). The occupations of the study groups are shown in Table 1. Most of the survivors (64.9%) were students of secondary and tertiary institutions as well as civil servants. Statistically, with a p < 0.001; the outcome of an abortion related complication appears to be associated with the occupation of the patient. The parity status of the subjects is shown in Table 1. Most of the fatalities (87.2%) were nulliparas. There was a significant association (p < 0.001) between parity and outcome of abortion related complications. Table 2 shows the interval between the abortion and presentation at the facility.61.5% of the fatalities presented in the hospital after 7 days while 87.4% of the survivors presented before 3 days. There was a significant association between the abortion-presentation interval and the outcome. In Table 3, the frequencies of specific abortion related complications are shown. The survivors had mainly minor complications like anaemia, retained products and pelvic infections while the fatalities had mainly multiple as well as major complications like haemorrhagic shock, septicaemia, perforated uterus and bowel injuries. There is a significant Discussion Unsafe abortion remains a silent scourge especially in the developing countries. The treatment of large numbers of women with complications of unsafe abortion is a major problem in the health care systems in Sub-Saharan Africa. Abortion complications are an important contributor to hospital-based maternal mortality and morbidity Reliable statistics on the incidence of abortion and associated morbidity and mortality are difficult to obtain as variations exist in the way abortion statistics are defined or calculated. The contribution of 24.7% of all maternal deaths in this series is high compared to 9.6% from a 17 –year review in North Central Nigeria10 and 12.5% from a series in Benin11 but almost similar to 21.1% from a series in Nnewi, Nigeria12 . The series from Sagamu reported 18.6% maternal deaths among cases of induced abortion in a ten year period13 . In Kenyan public hospitals, out of 20,893 women presenting in one year with abortion-related complications, 182 died, giving a case fatality rate of 0.87%14 . In this series, a case fatality rate of 11.5% was rather high. The summation of the findings from this study suggest clearly that a lot more of the maternal deaths in our facility were contributed by unsafe abortions and a relatively higher number of cases were likely to die from abortion complications. In our opinion, the cosmopolitan nature of the location of our facility as well as its tertiary nature may account for the relatively higher proportion of severe cases managed. In seeking to suggest possible correlates of mortality in abortion cases, the age distribution did not appear to matter. Most of both the survivors and the fatalities in this study belonged to the adolescent age bracket. A review found that two thirds of unsafe abortions occurred among women aged between 15 and 30 years15 . The proportion of women aged 15 to 19 years in Africa who have had an unsafe abortion is higher than in any other region4 . Almost 60% of unsafe abortions in Africa are among women aged less than 25 years4 . In Nigeria, a series showed that 60% of abortion seekers were between the ages of 15 and 24 years of which adolescents constituted 23.7%16 . Other studies from Nigeria documented similar findings12,17 . In the adolescent and early adult age brackets, the factors contributing to the relatively higher incidence of abortions include being in school, the unmarried status, contraceptive ignorance as well as lack of access to and high cost of contraceptive services18 . It is also posited that teenagers were more likely than women in the older age groups to obtain their abortion in the second trimester of pregnancy thus generating a theoretical possibility of increased complications and perhaps mortality12 The results from this series would seem to suggest that being married was associated with reduced chances of mortality from abortion complications. This is consistent with the findings from other studies12,17 . However in a 12 year review from Ile Ife, Nigeria, it was reported that married women constituted 59.3% of all cases of abortion complications and the point was made that illegal abortion affects all women regardless of their marital status19 It is however believed that the economic empowerment and spousal support likely to be assured within a marital setup will inevitably reduce the possibility of exposure to unsafe abortion. Most of the survivors in this study were students of higher institutions and civil servants, indicating a fairly reasonable level of education. Some other studies had documented the student population as the predominant group of abortion-seekers16 and the greatest sufferers of mortality17 . A low level of education was reported in 92.6% of cases of abortion related deaths in the Ile Ife series19 . In most parts of Sub-Saharan Africa, illiteracy, ignorance and poverty are a veritable recipe for resort to clandestine abortion with consequent morbidity and mortality. This study highlighted nulliparity as a possible correlate for mortality with 87.2% of fatalities being nulliparas. This finding was similar to 93.5% earlier documented12 and would appear to be consistent with our earlier finding that 89.3% of the fatalities were in the age range of 15 to 29 years. Nulliparity and young age may be associated with with the stigmatisation linked with unplanned and unwanted pregnancies thus leading to undue concealment of the fact.This promotes delay in finally making a decision to terminate. This may be complicated by lack of knowledge of available safe options for abortion. However more importantly, even when there is adequate knowledge of where to obtain safe abortions, lack of financial resources may make the resort to substandard facilities inevitable. Survival or death following a complicated abortion is clearly demonstrated to be partly a factor of early or late presentation. In this study, most of the survivors presented before 3 days while most of the fatalities presented after 7 days. This was similar to the findings in another study13 . Haemorrhage and sepsis, which are the leading causes of death in complicated abortions, will expectedly be more fatal in patients presenting late. Indeed, the common theme in fatal septic abortion is delay: delay in recognition, delay in getting to care, then delay in initiating care upon arrival9 . The severity of specific complications in this study significantly predicted mortality or survival. Other studies reported mortality in abortion cases when severe complications like haemorrhage and sepsis were present12,13,17 . Uterine perforation and bowel injuries were additional complications in patients studied in this series. It would appear therefore that apart from the inherent risks of haemorrhage and sepsis in complicated abortions, their performance by mainly unskilled personnel increases the possibility of additional visceral injuries. The nulliparous, single, illiterate patient with severe complications and presenting late for care is highlighted in this study as being particularly at risk of mortality. The case is thus reinforced for the encouragement of safe sex practices especially among adolescents as well as increasing their access to contraception. Physicians in the private sector and other relevant health workers need to refresh their knowledge of post abortion care and be constantly reminded about the need to refer complicated abortion cases to facilities where they can be managed in a standard fashion. The restrictive abortion laws in Nigeria also need to be liberalised. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09030t1.jpg] [rh09030t3.jpg] [rh09030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}