 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
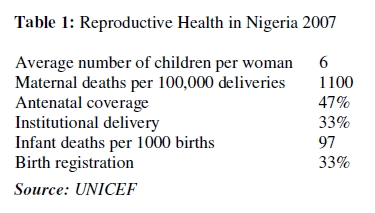
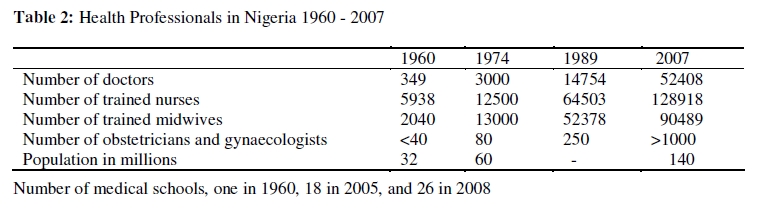
African Journal of Reproductive Health, Vol. 13, No. 3, Sept, 2009, pp. 9-20 Commentary The Struggle to Reduce High Maternal Mortality in Nigeria La lutte pour réduire la mortalité maternelle élevée au Nigéria Kelsey A Harrison*¶ *Adapted from a keynote paper entitled “Transforming health systems to improve lives of women and newborn babies in Nigeria” presented at the Nigerian National Health Conference at Uyo, Akwa Ibom State Nigeria on 8 June 2009. ¶Emeritus Professor of Obstetrics and Gynaecology and former Vice-Chancellor, University of Port Harcourt, Nigeria. For correspondence: Email: kaharrison19@hotmail.com Tel: +358 9 2753135 Code Number: rh09031 ABSTRACT According to UNICEF estimates for Nigeria, maternal mortality ratio is 1100 per 100,000 live births, antenatal care coverage 47 percent, institutional delivery rate 33 percent, and each woman bears six children on the average. Reducing the high maternal mortality ratio, which is the prime concern, has hitherto concentrated on transforming the health system through bringing resources and expertise to bear on the high maternal mortality per se including some of its surrounding elements. It has failed. High maternal mortality must be tackled at a much more fundamental level. In the complexities and uniqueness of Nigeria’s current situation, it is suggested that the fundamental remedy is to stamp out the chaos in the country by getting the politics and governance structures right. Accurate population census is paramount. Compulsory registration of births and deaths, fixing the broken-down educational system and bringing back the public service ethos the country once had, are core issues (Afr J Reprod Health 2009; 13[3]:9-20). RĖSUMĖ D’après les chiffres de la UNICEF pour le Nigéria, le rapport de la mortalité maternelle est de 1100 contre 100.000 naissances vivantes, 47% pour la couverture des soins prénatals, 33% pour le taux d’accouchement institutionnel et chaque femme donne naissance à six enfants en moyenne. Réduire la mortalité maternelle élevée qui constituait l’affaire de la plus grande importance, avait jusqu’ici mis l’accent sur la transformation du système sanitaire à travers les ressources et l’expertise consacrées à la mortalité maternelle élevée en soi, y compris certains éléments autour. Il faut aborder le problème de la mortalité maternelle élevée à un niveau beaucoup plus fundamental. Etant donné les complexiés et le caractère unique de la situation actuelle du Nigéria, nous suggérons que la solution fondamentale sera d’éliminer le chaos par la mise en place d’une bonne politique et d’une bonne gouvernance. Un recensement exact de la population est d’une importance primordiale. Les questions principales comprennent l’inscription obligatoire des naissances, la réhabilitation du système d’éducation qui est en panne et la restoration de la philosophie des services publics qui existait autrefois dans le pays (Afr J Reprod Health 2009; 13[3]:9-20). KEYWORDS: Antinatal care, Birth, Death, Maternal mortality, Nigeria Introduction One of the greatest failings in Nigeria and one that is partly responsible for much of the confused state of affairs, be it in health care or whatever, is not knowing enough about the past and an unwillingness to learn from it. Therefore, in this presentation, this is being corrected, in the belief that most things become clearer when viewed from a historical perspective. The focus here is primarily on the dangers of childbirth and not on issues about HIV/AIDS, abortion and family planning as important as they are. A Summary of the Present Position of Maternal and Perinatal Health in Nigeria Nigeria has one of the worst records of maternal and child deaths in the world, and they are worsening with time in some areas. The reproductive health statistics shown on Table 1 are all derived by estimates, therefore, they are by no means accurate but they are the best that are available and they are dreadful. The explanations for them are straight forward. Failure to satisfy the basic needs of the poorest people who make up the vast majority in the country is at the heart of this problem. I am of the view that if we look after the poorest and the least powerful, the rest will look after themselves. Permit me to digress somewhat. I have seen with my own eyes and I know what it takes to look after women and their newborn babies in a conflict zone. This was during our civil war of 1967-19701 . The conditions were awful. To this day I still have nightmares about some. I shudder to think what must be going on in our current conflict zone in the Niger Delta. Impressive Historical Landmarks: The Outstanding Gains in Community Obstetrics If one looks at the pathetic state of reproductive health in this country, one might conclude that the present is bad, the immediate future is bleak, and the distant future is too terrible to contemplate. That would be unfair. The achievements of the past give cause for hope for the future. The total coverage of these achievements is impossible. So only those considered to be landmark efforts in community maternity care in my lifetime will be presented. Those of us who are old enough to remember know that as early as the 1940s, elements of system of modern community obstetrics were practised to very good effect in some places in this country. They predated even the Alma Mata Declaration of Primary Health Care in 1978. Their recall is important. 1940s and 1950s In the 1940s, alarmed by the unsatisfactory obstetric outcome in the Diocese of the Niger, the people, their Native Administration, the Lagos-based colonial government, and the Church Missionary Society went into action 2 . The aim was “to raise the standard of midwifery work in this country and to try to bring it nearer to that of similar work in England and other countries”. To that end, the effort was directed to improve the way people lived and the way their health needs were being met. The strategy combined community health education on a massive scale, the setting up of trained midwives-mannedmaternity homes, the rigorous supervision of these homes, and the institution of measures to boost staff moral and efficiency, including scaling up of their salary and forbidding private practice. Fees were charged but they were affordable. It was noteworthy that traditional birth attendants (TBAs) were not part of the team effort, instead the training of midwives was stepped up, and the brightest and best of them were sent to England for advanced midwifery education. By 1949, in the 31 maternity homes that handled 6500 deliveries yearly, the maternal mortality ratio became 46 per 100,000 births. Katsina province was next. Beginning in 1945 and for over 35 years, the province ran a reliable system of compulsorily obtaining and keeping records of all births and deaths in the entire province of over 1 million people (see later for further details). The excellence of the quality of this source of data is attested to by the publication of good papers based on them 3. The concept of a base hospital that served all the maternal and child health clinics and many privately owned maternity centres in the Ilesha area with population of 100,000 was practised by the Methodist Church of Nigeria 4. Published records of its work described the linkages between the base hospital and its satellite establishments at urban and village levels, down to the facilities provided, staffing levels and deployment, buildings, records, and the organisation of the whole set up. Close to perfection, it offered a good opportunity for replication in the rest of the country but we failed to take notice. Acceleration of manpower development Then came independence in 1960. Even before, there were bold and wide-ranging attempts at improving social welfare. Health infrastructure and manpower provision and training advanced, and the momentum continues (Table 2). In 1960 there were 349 doctors, 5938 trained nurses, 2040 trained midwives, and fewer than 40 obstetricians and gynaecologists that served Nigeria’s estimated population of 32 million. By 2007, the rise in number was 150 fold for doctors, 20 fold for nurses, 40 fold for midwives, 25 fold for obstetricians and gynaecologists, and 5 fold for the population of the country. My personal view is that the establishment of the School of Nursing and Midwifery in University College Hospital Ibadan in 1952-3 is the most important development because of the sheer professionalism of its products and its implications for women’s education and empowerment. In research, the gains in knowledge of severe anaemia in pregnancy and sickle cell disease in pregnancy were monumental achievements of global significance Zaria Maternity Survey This work carried out in the department of obstetrics and gynaecology at Ahmadu Bello University Zaria, and led by me, is reported in detail elsewhere 5, and pundits reckon that the lessons it teaches are absolutely fundamental and that the report is as relevant today as it was when it was first published over 20 years ago 6. Data collection of 22774 consecutive hospital births, took place in a period of 3½ years from January 1976 to July 1979. The data were analysed in defining the role of both obstetric and nonobstetric factors in maternal mortality and morbidity with particular emphasis on the influence of illiteracy and educational levels. Overall, the results offered an insight into the key factors for maternal survival during pregnancy and childbirth. They are three:
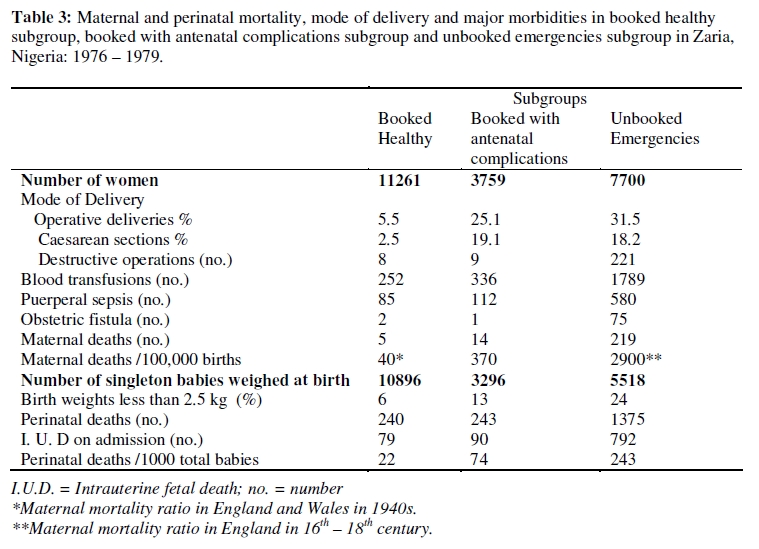
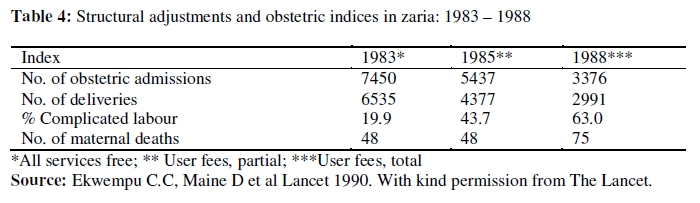
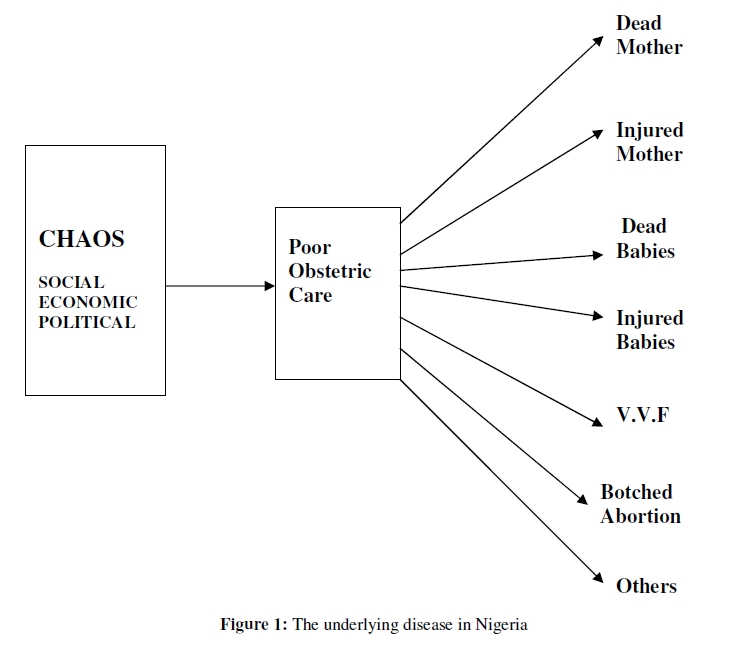
While socio-economic, cultural, political, religious, and health care systems prevent these conditions from being met, maternal mortality will remain high. The report documented the favourable influence of both formal education and antenatal care on the results of childbearing. In women who had never had any formal education nor received antenatal care, that is 33 % of the survey population, maternal mortality ratio was 2900 per 100,000 total births, perinatal mortality was 258 per 1000 total births, and 26 % of the babies weighed less than 2.50 kg at birth. With education and antenatal care combined, as was the case in only 10 % of the survey population, the maternal mortality ratio was 250 per 100,000 births, perinatal mortality rate was 30 per 1000 total births, and only 8 % of the babies were of low birth weight. Most maternal deaths occurred in unbooked emergencies, amongst whom the maternal mortality ratio was similar to that of much of Europe in the 16 – 18th centuries. By contrast, booked healthy women had very low maternal mortality ratio – 40 per 100,000 -similar to those in some modern-day European countries (Table 3). Among infants of good birth weight, perinatal mortality rates were also closely related to the uptake of antenatal care. Early teenage pregnancy and high parity groups are often considered highrisk, but detailed analysis reveals that this is generally only true under conditions of poverty and neglect. In good circumstances, their risks in pregnancy are not much increased. However, in addition to the usual risks of primigravid pregnancy, young teenagers who are poorly nourished may have pelves not yet fully grown, leading to a high incidence of operative delivery, obstructed labour and obstetric fistula (VVF). In Zaria, malarial chemoprophylaxis and iron and folic acid supplements given to adolescents during pregnancy resulted in a growth spurt both in height and pelvic capacity, with subsequent lowering of the incidence of difficult labour. The increased risk of maternal death in women of high parity is closely associated with a low level of economic and educational deprivation. Maternal mortality in this group also runs parallel to infant mortality. Maternal deaths are rare among women of high parity if all their children have survived, whereas women who have lost several children are at higher risk of maternal death7. These facts have important implications for family planning programmes, which in poor circumstances are insufficient alone to improve the maternal mortality rate. Bacterial infections, eclampsia, anaemia, haemorrhage and obstructed labour were the principal obstetric causes of death. There was marked increase in maternal mortality risk in women with haematocrit levels of less than 14 % and in women with haematocrit levels exceeding 45 %, affirming the need for installation in the labour ward, a microhaematocrit centrifuge so that emergency admissions can then be screened on the spot for anaemia or volume depletion and disasters avoided. There were other revelations and observations. Long delays in the treatment of ill pregnant women are the result of a variety of influences. These include poor health services organisation, transport difficulties, social disorganisation due to wars and civil strife, and harmful traditional customs, as well as simple reluctance on the part of women to make use of the available health care system. These delays mean that treatment may be more difficult and timeconsuming so that hospitals are overwhelmed by unbooked emergencies presenting late. They compete with the management of healthy booked women, who may therefore receive less than their due. High illiteracy rates impede the development of a country and affect progress even for the educated. Literacy is essential for knowledge, understanding and for participation in a country’s development. Indeed, despite scarce resources, China, Costa Rica, Cuba, Sri Lanka, and Kerala State in South India have succeeded in reducing maternal mortality. A common factor in all these countries is the high level of education in their populations. Education is at the very heart of the development process. Expounding on this thinking was with these words: “If you think education is expensive, try illiteracy”. The words of Galbraith were equally telling. He wrote: “There is, in our time, no well-educated, literate population that is poor; there is no illiterate population that is other than poor”. Next, we made the point that in Third World settings, there is no simple solution to the problem of emergency transportation: each area must make locally appropriate provision. Waiting homes or hostels adjacent to maternity units are valuable in rural areas served by poor transport. Another conclusion drawn was that nutritional supplementation might achieve improved results in early teenage pregnancy by improving pelvic growth and thus reducing the incidence of cephalopelvic disproportion and operative delivery. Lastly, the report asserted that further research is needed along the lines of that carried out in Zaria to define high risk factors locally, and that the results must be clearly transmitted to front-line health workers. Along side the Zaria Maternity Survey, the study of the sociology of VVF 8,9, was encouraged. This and other activities in the Zaria community led to 10 the eradication of VVF in the area in the late 1970s, and to the formation of the Nigerian National Task Force on VVF in 1990 11 . Although VVF has since resurged in the Zaria area, enough was done in placing the surgical treatment of VVF in our national agenda 11, 12 , and in bringing about the on-going worldwide assault on VVF 13, 14, 15. Important Historical Landmarks: The Mistakes So far, I have dwelt largely on successes but there have been terrible mistakes as well. Those highlighted here are particularly spectacular because the damage caused continues. The first set of mistakes concerned the Katsina effort. The records collected and kept were very reliable, full community participation was obtained, the Emir led it, and civil service personnel gave their unstinted support. Properly replicated elsewhere in the country it could have laid the foundations for civil registration and the collection of health-related information in rural areas. It afforded an opportunity of nurturing countrywide, the culture of generating reliable health and socioeconomic statistics and indeed population statistics but we blew it. Instead, the use of sporadic estimate of population data came into vogue. Pity, because if you want to change anything, you get your public facts first and in doing so, you should not distort reality in order to make the task easy. The best thing is to start from the reality, which for safe motherhood, means actual counts of births and deaths on a continuous basis and in a structured manner, not ad-hoc estimates of population data. The use of estimates is a poor substitute for compulsory civil registration. Not surprisingly, progress has stalled after initial flourish. There is another dimension to the issue of counting correctly, and it applies here too. Ideally, a society has to make it a habit to weigh, measure, and record outcomes correctly. Failure to do so results in widespread belief in superstition, magic, and miracles, one of whose consequences is the growing popularity of all sorts of prayer houses and Pentecostal churches in this country. The greatest mistake, in my view, was the adoption in the early 1980s of neoliberal economic policies forced on us by the World Bank and International Monetary Fund. Branded as Structural Adjustment Programmes (SAP) they were meant to cure our economic ills. Weakening of governance structures, reduction of state machinery, drastic reduction in the size of the public sector, worker retrenchment, increasing private sector involvement, savage devaluation of the naira, increasing privatisation, and the charging of user fees for cost recovery in health care were all part of SAP. The consequences were damaging. The results on maternal and child health and education in most places in Sub Saharan Africa were catastrophic 16,17, and recovery is still nowhere in sight. In terms of maternal mortality and morbidity, Zaria’s experience shown in Table 4, was typical. SAP in one fell swoop wiped out much of the good work done by generations of dedicated men and women, both nationals and nonnationals. Hence adoption of the principles of SAP or anything remotely like them will mean reinforcing failure, which is never a good thing to do. Thoughts on Transforming Maternal Health Care in Nigeria Currently, a large proportion of our population recognises the need for modern maternal health care. But because public system of doing this is riddled with vices, people have no confidence in it, and one consequence is that those of pregnant women who can afford to do so, seek care and support in two or more places at the same time -the public system, private clinics and hospitals, prayer houses and TBAs. Some go to the extent of doing without any assistance at all. Among the affluent minority, some go abroad just to have their babies normally. Frankly this is a national disgrace. It is not acceptable. We need to perform better so that our women have confidence in the system of modern maternity care, and patronise the public hospitals and those of the private establishments that are properly regulated. Be reminded that TBAs are a product of their time, but that, surely, that time has passed. As for primary health care (PHC) my thinking is that it is trying to seek grassroots solutions to Maternal and Child Health problems. If this is the case, then I suggest that one action it can take is to encourage us to mount as a matter of urgency, surveys of the type carried out in Zaria, but community-based instead of being hospital centred, and in different areas in the country. The less disjointed they are, the better. Based on the results obtained, prioritisation of needs, their implementation and evaluation should logically follow, guided by well established principles made widely available especially from WHO sources. It will mean among other things that the various sectors of our government need to work closely together to improve health standards. Perhaps, this is already the case but I am not sure that it is, particularly at the grassroots or Local Government level. Next to be considered are some practical problems, and most are about money. Obviously, the system of funding health care in this country is important. In my view there is need to review it urgently. Like most developing countries, and unlike most developed countries and those of developing countries with low maternal mortality ratios, we are yet to put in place the one type of health systems financing known to be least expensive and most equitable: it is tax based, and public funded, with universal access free at the point of care 18 . Presently, it is rarely recommended and practised in developing countries including Nigeria, as it should. For most Nigerian families, the out of pocket payments they have to make in order to cover user fees charged, are unaffordable. In any case, the concept of charging user fees is now reckoned to be bad for health care systems 19 . The Nigerian National Health Insurance Scheme is meant to offset some of the hardships caused by charging user fees, but it remains ineffective. There is the Abuja Declaration, which in 2002 recommended that government should spend 15% of its total revenue on health. To the best of my knowledge, we are not doing so yet. If so, why? In any case, what stops us from raising revenue through taxation? As an interim measure, a case could be made for charging fees for normal deliveries but not for operative deliveries especially caesarean sections. I turn briefly to the issue of Non Governmental Organisations (NGOs). There are over 800 registered NGOs in Nigeria, of which around 100 operate in the fields of gender and women’s development, and about 50 deal with children’s issues. Their large presence would seem to indicate that action is being taken increasingly to make things better for our women and children. However, it is the coherence of their action and their level of commitment that are open to question. I believe it is up to our government to effect donor coordination so that their activities bring about short and long term gains for our people. We should state our priorities for them to follow not the other way round. Furthermore, care must be taken to ensure that they do not become part of the problem we are trying to solve. There are all sorts of policies and strategies being proposed to turn things round for the benefit of women and children in our country. Perhaps the most topical of these policies and strategies are those that are enshrined in the United Nation Millennium Development Goals (MDG), which member states and some international organisations agreed to achieve by the year 2015. There are 8 goals, 16 targets and 48 indicators. Poverty reduction is Goal number 1, reducing under-fives mortality by twothirds is Goal number 4, and cutting maternal death rates by three quarters is Goal number 5. The best thing that can be said about them is that they give cause for hope of better things to come. Mention must also be made of the role of traditional medicine. Here, the argument in favour is thin because the truth is that there is no system of traditional medicine known to give full protection to women during pregnancy and childbirth. So, where does the future lie? Here is another thought. Those of us who are retired after a lifetime spent in battling against enormous odds to reduce maternal mortality, we now have plenty of time for sober reflection. We have come to realise that in focussing on damaged mothers and their babies, and how PHC can make things better for them, we are looking at the wrong end of the problem. The Underlying Disease Dead and damaged mothers and infants make up a cluster of conditions resulting from one thing, very poor obstetric care. But then, very poor obstetric care is one result of the chaotic socio-economic and political systems, which is the major underlying disease (Figure 1). It is the disease that must be treated. To transform a society such as present day Nigeria, where scarcely anything works properly into a society where most things work to the general benefit of society, only bold measures will have the desired impact. Clearly, the solution is political largely. I expressed this view most forcefully in a paper I delivered on Africa Day, 23 March 2007, at the Royal College of Obstetricians and Gynaecologists in London. The title of the paper was “Thoughts on making safe motherhood work better”. Shiffman and Okonofua, in an important paper 20 agree, but their suggested approach differs from mine. In my view 21, 22, getting the population census right is the core issue. Next is the provision of quality basic formal education because of the social, economic, political and health benefits it confers. The current system has broken down. We must fix education, invest in it, resource it properly, look at the countries that do it best, seek their assistance and copy. There is no shame in copying what is good, as there is in copying what is bad. Another measure must be the counting and proper recording of all births, deaths and cause of death. Advocacy for this has a long history 23 and more recently The Lancet has made the case for it, even stronger 24-30. I am aware that the National Population Commission, an agency of the Federal Government, has this responsibility. To be honest, it needs to do its work better. And at the same time, Nigeria’s health professional bodies especially the Nigerian Medical Association and Society of Gynaecology and Obstetrics of Nigeria could give the lead. In conclusion, societal dislocation and weak governance structures cause the all-pervading chaos in our society, one effect being that the way our health system presently operates cannot guarantee improved maternal and perinatal survival. However, blaming the bureaucracy, seeking private-public partnerships, wholesale privatisation, increasing NGO involvement, working towards the fulfilment of the Millennium Development Goals, all look good on paper, but in the complexities and uniqueness of Nigeria’s current situation, they are peripheral issues. There will be little or no hope unless we get the politics and governance structures right, and bring back the public service ethos we once had. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09031t2.jpg] [rh09031t4.jpg] [rh09031f1.jpg] [rh09031t3.jpg] [rh09031t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}