 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
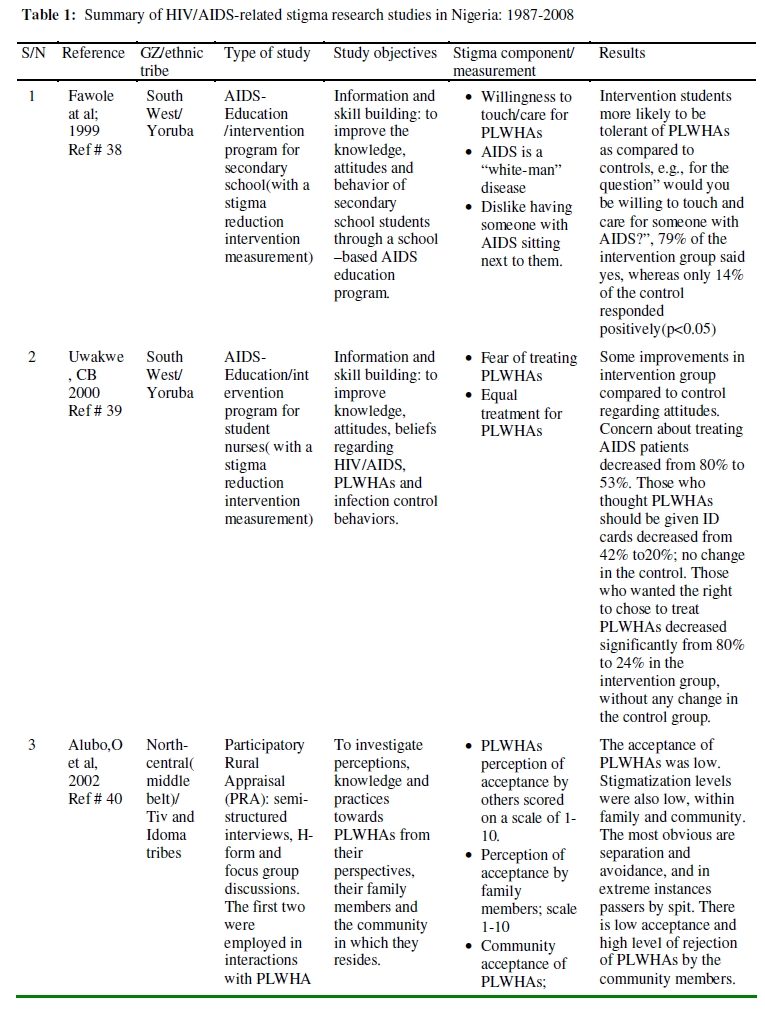
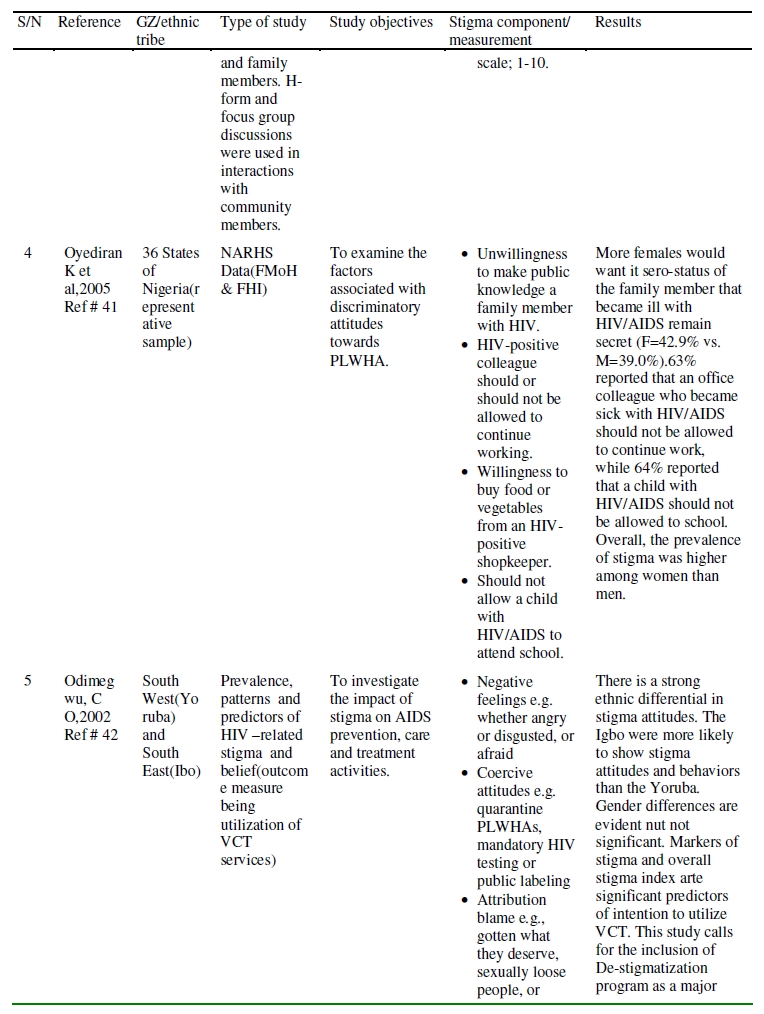
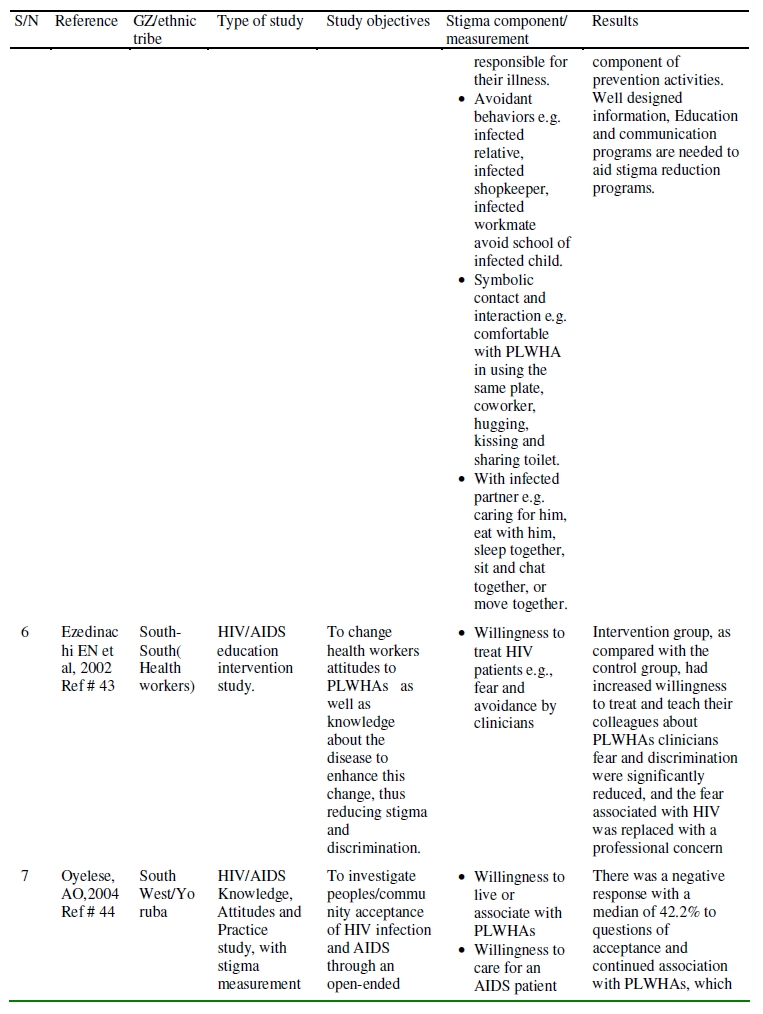
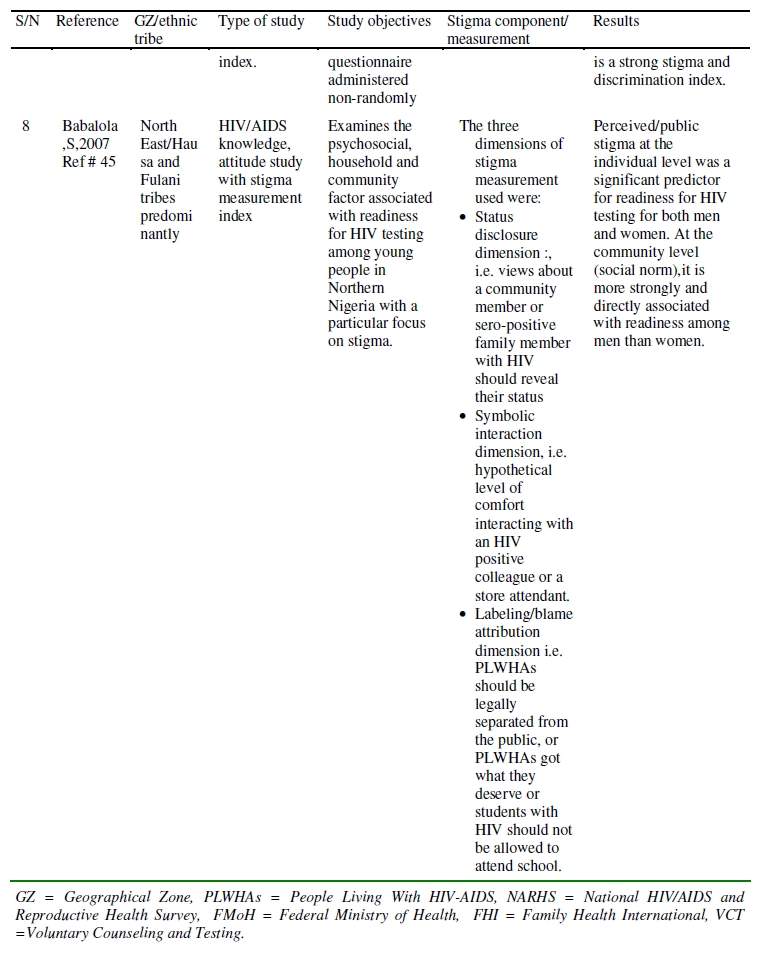
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 21-35 ORIGINAL RESEARCH ARTICLE HIV/AIDS -Related Stigma and Discrimination in Nigeria: Review of Research Studies and future directions for Prevention Strategies Stigmatisation liée au VIH/SIDA et la discrimination au Nigéria: Compte-rendu des études de recherche et la direction future pour les stratégies de la prevention. *Emmanuel Monjok, Andrea Smesny and E. James Essien *Institute of Community Health, University of Houston, Texas Medical Center, 1441 Moursund Street, Houston TX, 77030, USA. For correspondence: Emmanuel Monjok MD, MPH. Email: emonjok@uh.edu ABSTRACT Human Immunodeficiency Virus (HIV) infection and AIDS remain a major public health crisis in Nigeria which harbors more people living with HIV than any other country in the world, except South Africa and India. A significant challenge to the success of achieving universal access to HIV prevention, treatment, care and support by 2010 is HIV-AIDS stigma and discrimination. Eight studies looking at some degree of measurement of stigma and discrimination in Nigeria were reviewed in an attempt to investigate the cultural context of stigma, health seeking behavior and the role both perceived and community stigma play in HIV prevention. Results suggest that reducing stigma does increase the individual as well as community acceptance of people living with HIV-AIDS (PLWHAs), but long term studies are needed. Some suggestions are recommended for future research on culture specific stigma studies in Nigeria (Afr J Reprod Health 2009; 13[3]:21-35). RĖSUMĖ L’infection du virus de l’immunodéficience humaine (VIH) et le SIDA reste une crise majeure de la santé publique au Nigéria, un pays qui abrite un plus grand nombre des gens séropositifs que les autres pays du monde, à part l’Afrique du Sud et l’Inde. La stigmatisation et la discrimination causeés par le VIH/SIDA constituent un défi important aux efforts pour l’accès universel à la prévention, au traitement, au soin et au soutien jusqu’en l’année 2010. Nous avons fait un compte-rendu de huit études qui examinaient à quelque niveau de mesures de la stigmatisation au Nigéria afin d’évaluer le contexte culturel de la stigmatisation, le comportement qui favorise la santé et le rôle que jouent à la fois la sstigmatisation perçu et la stigmatisation de la communauté dans la prévention du VIH. Les résultats ont montré que la réduction de la stigmatisation augmente, en effet, l’acceptation de l’individu ainsi que l’acceptation par la communauté des gens séropositfs: mais il faut des études à long terme. Nous avons fait quelques recommendations pour les recherches futures à l’égard des études de la stigmatisation propre à la culture au Nigéria (Afr J Reprod Health 2009; 13[3]:21-35). KEYWORDS: HIV/AIDS, Stigma, discrimination, Nigeria Introduction Human Immunodeficiency Virus (HIV) infection and AIDS in Nigeria remain a major public health crisis. Nigeria is Africa’s most populous nation and is home to more people living with HIV than any other country in the world, except South Africa and India. 1 The prevalence rate has increased progressively since the first reported case of HIV in Nigeria. 2 HIV prevalence among adults aged 15-49 years, increased from 1.8% in 1991 to 5.8% in 2000, 3 and in 2005, declined to 3.9 %. 2, 4 Although the prevalence rate is lower than it is in South Africa, it is estimated that about 2.9million people are living with the virus in Nigeria.2 In 2005, the international community embraced the goal of universal access to HIV prevention, treatment, care and support by 2010.5, 6 To achieve this goal, national HIV/AIDS programs need to strengthen their health systems and block all barriers to treatment and prevention programs. Nigeria has taken various strategies to limit the spread of this disease. Due to global initiatives like the US Presidential Emergency Plan For Aids Relief (PEPFAR) program, there has been substantial increase in the number of people living with HIV/AIDS (PLWHAs) who are on Antiretroviral Therapy (ART),as a result of having taken an HIV test.7 In addition, there are many more antenatal women with HIV positivity who have received ART to prevent mother to child transmission of HIV.8 The challenges many of these global and national programs face in a multi-diverse socio-cultural society like Nigeria are the problems of stigma and discrimination(S&D). The issues of S&D described by Jonathan Man 9 as the third phase of the HIV pandemic poses a serious threat to prevention and treatment. Therefore, for Nigeria to achieve her national policy on HIV/AIDS, aimed at controlling the spread of the infection and its impact, the issue of S&D needs to be addressed. Significant research and knowledge on HIV related S&D in many ethnic and cultural settings that constitute Nigeria, are important tool in understanding this “hidden factors” that are impediments to effective prevention and treatment. Incorporating these findings into national prevention strategies will go a long way in reducing the transmission of the virus in the population. Stigma and Discrimination Stigma is often associated with discrimination and human right and has been defined in various ways.. Erving Goffman 10 defined stigma as an undesirable or discrediting attribute that an individual possesses, thus reducing that individual’s status in the eyes of society. Stigma can stem from a particular characteristic, such as a physical deformity, or from negative attitudes towards a group, such as homosexuals or prostitutes. Under Goffman’s definition, society labels an individual or group as different or deviant. Jones et al 11 defines stigma as an attribute that links a person to undesirable characteristics. Crocker et al 12 indicated that stigmatized individuals are believed to possess some attributes or characteristics that convey a social identity that is devalued in a particular social context. Others have defined stigma as societal processes that are linked to societal power structures. 13 Stigmatization can lead to prejudicial thoughts, behaviors, and actions on the part of governments, communities, employers, health care providers, coworkers, friends, and families.14-16 Discrimination is an aspect of stigma defined as a form of exclusion, or restriction of expression, marginalization, or prevention from access to something or services.17, 18 Discrimination is normally expressed by force, from avoidance to life threats, lynching and death.17, 19 Stigma has been classified by several authors. Some divide stigma into felt, or perceived stigma and enacted stigma.20, 21 AIDS stigma by association with someone who is HIV positive is classified as secondary stigma or “courtesy stigma” which can affect family and friends of PLWHAs, as well as health care workers.22, 23 Other classifications identify S& D as operating at three levels; personal, community and institutional.17 S&D are major obstacles to effective HIV/AIDS prevention and care, globally. S&D in the context of HIV/AID is unique when compared to other infectious and communicable diseases. It tends to create a “hidden epidemic” of the disease based on socially-shared ignorance, fear, misinformation, and denial.17, 24, 25 This is particularly more intense in sub-Saharan Africa, including Nigeria, where a combination of weak health systems is entangled with poor legal and ethical framework.26 Significant and relevant research studies are needed to thoroughly understand the consequences of S&D at the three levels and its effect on HIV prevention, treatment and care as it is directly related in the different socio-cultural settings in Nigeria. Individual level S&D S&D lead to identity crises, isolation, loneliness, low self-esteem and lack of interest in containing HIV-AIDS. 25. It also leads to lack of motivation to practice prevention.27 Fear of S&D limits the efficacy of HIV-testing programs because it prevents individuals from taking an HIV test14, 17, 22 and leads to reduced care seeking behavior.23 Community level S&D At the community level, fear of S&D can cause pregnant women to avoid voluntary counseling and testing, which is the first step in reducing mother-to-child transmission.28-30 It may force mothers to expose babies to HIV infection because using alternative feeding methods, other than breast feeding, especially in the rural communities, would arouse suspicion of their HIV status.31 Family members who are identified as taking care of HIV infected member of their family, also suffer from S&D.32 Open support for HIV/AIDS activities by community and civil organizations may be adversely reduced as a consequence of S&D.33 Institutional level S&D HIV infected individuals may face termination of appointment, hostility, denial of gainful employment, forced resignation or retirement.17 S&D experienced within the health sector represents one of the most inimical forms of institutional stigma. Discriminative acts among healthcare workers include, delivery of poor quality treatment and counseling services, early discharge from hospital, segregation of hospital wards, isolation, the marking or labeling of patients beds, files and ward, selective application of “universal” precautions and lack of confidentiality.34, 35 Other factors There are also other factors that influence S&D like gender, age and background factors,17 social class,17 geographical regions 36 and religion.37 Understanding and removing the barriers of S & D is a critical public health issue for HIV/AIDS prevention strategies in Nigeria. Current initiatives and prevention and treatment programs will be more effective if culturally appropriate and culture specific research on S&D is documented and understood. This paper aims to review published research studies in Nigeria that addressed HIV/AIDS –related S&D, with the intention of providing an analysis of these research output and identify critical areas so as to encourage and drive more culture specific and in-depth research on S&D in the various multiethnic societies in Nigeria. The range of studies to be identified would include cultural epidemiological studies, measurement of health related stigma, stigma reduction interventions and evaluation of HIV-related S&D. A thorough understanding of these stigma dynamics would help strengthen the contents, as well as shape prevention intervention programs in Africa’s most populous nation. Methods Electronic search of published literature was conducted with the key word: HIV, AIDS, and HIV/AIDS, stigma, which were combined at various times with the terms: Nigeria and sub-Saharan Africa. The search was restricted to English language articles only. We searched all original articles that were published from 1987 to 2008 on HIV/AIDS stigma on MEDLINE, psycINFO, Science citation index, social science citation index, EMBASE, CINAHL, AIDSLINE, and POPLINE. Additional searches were done via journal search i.e. journals specifically tailored towards all aspects of HIV/AIDS research. Reports from international NGO as well as university research fellowship documents were also consulted. Internet Google scholar search was also done. The main criteria for inclusion in this review is that the paper significantly focused on (1) Cultural epidemiology of stigma. (2) Measurement of stigma, particularly health-related stigma (3) Stigma reduction interventions. (4) Evaluation and assessment of stigma and discrimination. Using these criteria, we identified 8 studies that met these criteria. We excluded the majority of articles that were studies directed at knowledge, attitude and practices (KAP studies) towards PLWHAs that had no input on stigma measurement, literature review articles on S&D in sub-Saharan Africa, including Nigeria and anecdotal articles on stigma from PLWHAs. Results A comprehensive search of published information on HIV stigma in Nigeria using the various electronic search engines outlined in the methodology, shows that very little has been done on stigma in the various multi-cultural and diverse communities in Nigeria. Table 1 (a, b, c, d) shows a summary of the eight identified research studies in Nigeria that have some degree of stigma measurement. The table includes the geographical zone and the ethnic tribe where the study was conducted. There are many articles and studies not related to stigma but where a comment on the impact of HIV/AIDS stigma was mentioned. These studies were not included since most were anecdotal notes on the effect of stigma Attitudes towards PLWHA Negative attitudes of PLWHAs among the population are some of the most common manifestations of AIDS stigma, which potentially lead to discrimination. As a result, the intervention research is aimed at increasing tolerance and acceptability by decreasing these negative attitudes and promoting positive change in behavior towards PLWHAs. The eight studies 38-45 all have some index of trying to change the negative attitudes in the general population, towards PLWHAs. These include students, 38, 39 health workers 43 and the general community.40-42, 44, 45 Willingness to treat PLWHAs among health care workers There is increasing concern about health care workers reluctance to care for and treat PLWHAs. There is no particular health worker exempted from this reluntance. Nurses in Nigeria have an important role to play in the prevention of this epidemic because they are most of the time the “gatekeepers” in the various communities in Nigeria, especially in the rural areas, where very few doctors are likely to be practicing. There is one study, 43 both information and skill building intervention studies, aimed at improving the knowledge of the disease among health care workers, as an important aspect in changing behaviors towards PLWHAs. Perceived stigma of PLWHAs PLWHAs do need some coping mechanism to be able to live normal lives within their family and communities. Only one study 40 attempted to assess the perceived stigma of HIV-positive individuals within the family and community. Discussion This mini review has a few relevant observations. First, there is still great fear of HIV/AIDS due to poor understanding of the disease process in the Nigerian population, even among the healthcare providers. Second, there is no identifiable research study on the cultural epidemiology of HIV/AIDS stigma in the various ethnic populations. Third, much anecdotal evidence of the impact of stigma on care is documented but, very little rigorous research has been conducted. Fourth, very limited intervention studies on stigma reduction have been done and the few were of short duration to warrant any significant long term impact. Fifth, more epidemiological studies are needed to understand the relationship of stigma on prevention initiatives in Nigeria. HIV/AIDS related stigma and the resulting discriminatory attitudes creates an environment that fuels the epidemic. This is often times as a result of inadequate knowledge about the disease in the general population, even among health care professionals. Several studies 46-48 among nurses, physicians and laboratory scientist in Nigeria show that these groups of care givers still lack knowledge about the disease, thus enhancing their negative attitudes and often times refusal to treat and care for PLWHAs. AIDS-education/intervention studies aimed at students and health care givers, as in Fawole at al 38 and Ezedinachi et al 43 respectively, were designed to increase the knowledge base of the participants. Although the time frame was short after the intervention, 97% of the students in the intervention group were willing to touch and care for PLWHAs compared to 14% of the control group 38 indicating that a long term, continuous and population based AIDS education program can significantly increase knowledge and thus reduce stigma and discrimination. The fear of stigma has been identified as an important factor for pregnant mothers not to seek voluntary counseling and testing.28-30 The more antenatal patients know their HIV status the better for the prevention of mother to child transmission programs (PMTCT). There is now substantial evidence to the fact the PMTCT is feasible, but it is still imperative the mothers to know their own HIV status. The role of perceived stigma, both at an individual and community level did result in reducing the willingness and readiness to participate in HIV testing.45 The implication for PMTCT is grave since this program has been successful in many countries where routine HIV testing is done and where the factor of fear and stigma has been significantly reduced. It is therefore absolutely important that stigma reduction programs should be vigorously pursued in the various multiethnic communities in Nigeria, if PMTCT is to be sustained. The various ethnic tribes in Nigeria are diverse. The study by Babalola 45 was done among the Hausa/Fulani tribe, which is the dominant tribe in Northern Nigeria. Similar studies need to be conducted in the other major tribes in the West, East, and South –south of Nigeria, because of the interplay of culture and religion on the acceptability and willingness to have an HIV test. As outlined in the study by Odimeqwe 42, the cultural diversity between the Yoruba in the West and the Ibo in the East is responsible for the manifestations of HIV/AIDS stigma. The Ibo in the Eastern part of Nigeria are more eager to avoid PLWHAs than the Yoruba in the Western part of Nigeria. They also harbor negative feelings towards infected individuals. The Yoruba are more eager to support mandatory testing and attribute blame to infected individuals than the Igbo. It is possible that the different levels of socio-economic development could account for these ethnic differences. The Western states are more advanced in terms of education and the level of Non-Governmental Organizational (NGO) AIDS educational activities are higher and more concentrated here than in any part of Nigeria. This again enhances the fact that knowledge of the disease process is a significant tool in stigma reduction and prevention/ intervention strategies. The effect of stigma on public health intervention is well documented. For many interventions to achieve universal coverage, stigma reduction should be a major player in the design and implementation of HIV/AIDS prevention programs. With the introduction of new antiretroviral drugs, better delivery services as well as prevention of pediatric AIDS, a significant proportion of research on community as well as individual stigma epidemiology is needed, since the possibility of an HIV vaccine is still in the distant future. Suggestions to address the stigma issue in AIDS prevention include, but are not limited to: (1) The news media, home videos, radio jingles etc should be used to produce de-stigmatization programs in schools, hospitals, religious centers. (2) The introduction of AIDS education can be integrated into the curriculum of teaching in the country from primary to university. (3) Empowerment of the stigmatized group like the PLWHAs and the commercial sex workers as well as their involvement in the design and implementation of prevention programs in the country. (4) Health education campaigns should integrate a change from fear to caring for PLWHAs as this is particularly important for the health care personnel.(5) More prevention activities should be situated in rural and remote areas than in urban locations, as it is currently in Nigeria. Since 65% of the population resides in the rural area, it is most appropriate to concentrate these programs where the majority of the population resides. This translates to more emphasis on primary care. (6) More research is needed to study the role of culture, religion and social structures and their relationship to stigmatizing attitudes in the various ethnic communities that make up the over 140 million people in Nigeria. (7) Destigmatization should be a major component of the Abstinence, Be faithful and Condom (ABC) approach in prevention strategies. There are few limitations to this paper. It is possible that our mini-review is biased since we were not able to guarantee the inclusion of all published papers in this topic. In addition, more indepth cultural studies that are of longer duration need to be reviewed in the future, before a concise interpretation of the role of stigma in HIV disease transmission reduction can be made in Nigeria. And finally, our paper might be biased since we were unable to examine studies published in languages other than English, however, this is unlikely, since Nigeria is an English speaking country. In summary, we have shown that there is paucity of relevant research on stigma and discrimination related to the HIV-AIDS epidemic in Nigeria, although there is much anecdotal evidence documenting the role of stigma on individual and community participation in health related activities. Stigma remains a barrier to all the essential components that make up a good prevention program, and much detailed research on stigma reduction is needed to improve the components of a good prevention program. These components can include HIV testing, utilization of a crucial prevention strategy in pediatric AIDS known as PMTCT, antiretroviral therapy initiatives, and community awareness programs. The results of such stigma studies will increase our knowledge and cognizance of HIV risk factors and should lead to an increase in both the global and national communities potential to strengthen HIV-AIDS intervention and prevention program in Nigeria as well as other global populations affected by this public health crisis. The end results should contribute to a declining prevalence of HIV infectivity in sub-Saharan Africa and the rest of the world. Acknowledgement The preparation of this manuscript was facilitated by National Institute of Mental Health grant number RO1 MH073361-02. We acknowledge the excellent administrative assistance of Ms Ruthie Pittman of the Institute of community health, College of Pharmacy in preparing this manuscript. References
The following images related to this document are available:Photo images[rh09032t1c.jpg] [rh09032t1d.jpg] [rh09032t1a.jpg] [rh09032t1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}