 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
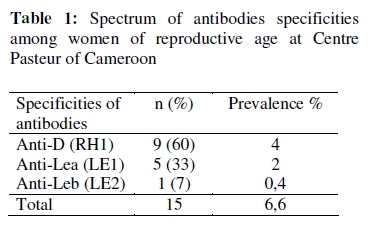
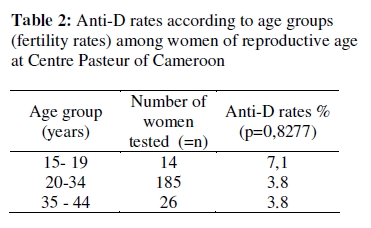
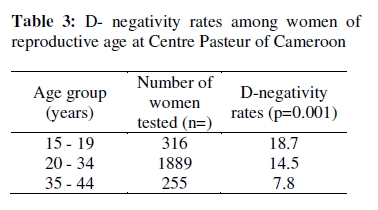
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 47-52 ORIGINAL RESEARCH ARTICLE High Prevalence of Anti-D Antibodies Among Women of Childbearing Age at Centre Pasteur of Cameroon Haute prévalence des anti-corps Anti-D chez les femmes en âge d’avoir des enfants au Centre Pasteur du Cameroun. Belinga Suzanne1, Ngo Sack Françoise2, Bilong Catherine1, Manga Jeanne1 Mengue Marie-Ange1 and Tchendjou Patrice3 1Laboratory of Hematology, Centre Pasteur, Yaounde, Cameroon; For Correspondence: BELINGA Suzanne, Centre Pasteur of Cameroon, B. P. 1274 Yaoundé Cameroun. Tel: +237-2203-6622; Fax: +237-2223-1564. Email: belinga@pasteur-yaounde.org ABSTRACT We conducted a cross sectional retrospective study to determine anti-D and D-negative phenotype rates among Cameroonian women of reproductive age (15 – 44 years), in order to evaluate the importance of D alloimmunization. Analysis of the haematology laboratory records from January 2006 to December 2007 harvested 225 results for red blood cell alloantibody screening and 2460 D phenotypes. Anti-D rate was found to be high at 4% and not linked to women’s parity. Three hundred and fifty two (14.3%) women were found to be D-negative. Anti-D rates significantly decreased with age from 18.8% among teenagers (15-19) to 7.8% among older women (35-44) (p = 0.001). The number of women submitted to both irregular antibody screening and type D phenotype determination was not strong enough (50) to analyse the link between anti-D rate and antigen D distribution in our study (Afr J Reprod Health 2009; 13[3]:47-52). RĖSUMĖ Nous avons mené une étude retrospective et transversale pour déterminer les anti-D et les taux de phénotype D-négatif chez les femmes en âge d’avoir de reproduction (15 -44 ans) à l’aide des laboratories du Centre Pasteur du Cameroun afin d’évaluer l’importance de l’alloimmunisation-D. L’analyse des documents du laboratoire d’hématologie de janvier 2006 au décembre 2007 ont produit 255 résultats pour le dépistage de l’alloanticorps du globule rouge et 2460 phénotypes-D. Quatre vingt-six pourcent (40/50) des femmes ont subi les deux dépistages de l’anticorps irrégulier et le phénotype-D était D-négatif. Le taux de l’anti-D s’est montré élevé à 4% et resté le même à tous les âges, ce qui indique qu’il n’y avait pas assez de mesures de prévention par rapport à l’alloimmunisation-D. Le test chez 352 femmes (14,3%) était D-négatif. Le test de la Dnégativité ont diminué de façon significative avec l’âge. Allant de 18,8% chez les adolescents (15-19) jusqu’à 7,8% chez les femmes plus âgées (33-44) (p= 0,001) (Afr J Reprod Health 2009; 13[3]:47-52). KEYWORDS: Alloantibodies, Anti-D, Childbearing age, Women, Cameroon. Introduction The presence of red cell alloantibodies during pregnancy can result in severe obstetrical complications ranging from new-born child’s haemolytic disease to fetal death by anaemia.1 Antibodies of the Rh and Kell systems are most frequently reported to be associated with obstetrical complications.2 Anti-D specificity is the most frequent antibody identified among women of reproductive age, accounting for almost one-fourth of all antibodies responsible for obstetrical complications.3 Anti-D antibodies appear after blood transfusions or from previous pregnancies with a fetus carrying the D antigen while the mother is D-negative.1 The risk of maternal D alloimmunization is influenced by the frequency of D alleles in a given population 1,4 . American Indians and Asians are almost all D-positive; consequently, D alloimmunization is not a main concern among these populations1,5 . While D alloimmunization is a typical problem for White women among which D-negativity frequency is the highest between 15-18%.6,7,8 Widespread adoption of guidelines for the prevention of D-alloimmunization and safe blood transfusion practices have reduced the incidence of D alloimmunization in western countries. 4,6,9 D-alloimmunization is also related to higher order birth and abortion rates 1,4 . D-negativity rates vary from 3 to 8% among the Black populations and therefore D alloimmunization still deserve some special attention in Africa. 1,7,8,10 As data on D alloimmunization among Cameroonian women of reproductive age are scarce, we conducted a cross sectional retrospective study to determine anti-D and Dnegativity rates among Cameroonian women of reproductive age tested at Centre Pasteur of Cameroon. Materials and Methods Design A cross-sectional retrospective study was conducted from January 2006 to December 2007 in Centre Pasteur of Cameroon, the national reference laboratory in Yaounde. Data The haematology laboratory records were reviewed. All women aged 15 to 44 years, found to have an antibody screening or a type D determination, were retrieved. Techniques Red cell antibody screening was performed with an indirect gel technique using a three cell screening panel at 37°C in LISS-Coombs and enzymatic medium. When irregular antibody was suspected, the blood sample was further tested with a full red cell panel to determine the antibody specificity. The screening, identification cell panels and gel micro tubes were from DiaMed (Morat, Switzerland). Red cell antibody screening and identification were performed on clotted blood, at the latest 72 hours after collection. D phenotype was determined on EDTA blood samples, using both direct gel technique (DiaMed, Morat, Switzerland) and slide with Transclone sera (BioRad Marnes-La Coquette, France). Statistical analysis Data analysis were performed with Epi info 3.4.1 (July 2007; Center for Disease Control, Atlanta, USA) software. For statistical analysis, women of childbearing age were divided into 3 groups, with ages according to the fertility rate as defined by the Cameroon Demographic and Health study III (CDHS-III) in 200411 . Age groups were characterised as follow: group 1: women aged 15-19 years representing teenage fertility (141/1000); group 2: women aged 20-34 years with the highest fertility rate (226/1000) and group 3: women aged 35-44 with the lowest fertility rate (98/1000). Results Anti-D rates A total of 286 red cells antibody screenings were performed from January 2006 to December 2007. Age and sex were available for 256 (90%) files, among which 228 belonged to women aged 15 to 44 years. Only 225 (88%) women were included in the analysis after exclusion of 3 repeated tests. The median age of the study population was 28 years, with ages ranging from 17 to 42 years. Fifteen women were found to have irregular antibodies giving a prevalence of 6.7% (CI 95%: 3.8 – 10.8) in the study population. Their specificities were further characterized as follows; 9 anti-D, 5 anti-Lea, and 1 anti-Leb (Table 1). The unique specificity of clinically significant antibody found was anti-D. Therefore, the prevalence of anti-D among women of reproductive age was found to be high at 4% (CI 95%: 1.9 – 7.5). Anti-D rates by age groups were not significantly different (p=0.73) as shown in Table 2. D -Phenotype determination During the study period, 5319 Dphenotype determinations were carried out. Age and sex were available in 4591 (86%) files among which 2460 (46%) belonged to women of childbearing age. The median age was 25 years and ranged from 15 up to 44 years. Three hundred and fifty two, that is 14.3% (CI 95%: 12.9-15.7) were found to be D-negative. This D-negativity rate is very high for a Black population. When distributed by age groups, D-negativity rates significantly decreased (p= 0.0001) with age as shown in Table 3. Only 50 women have had both irregular antibody screening and D phenotype determination in our laboratory during the study period. D-negativity rate was 86% (n=43) among them. Discussion During this 2 years period when data was analysed, 88 % of requests for screening irregular antibodies in our laboratory were made by women of reproductive age (15 –44 years). As our laboratory doesn’t have a blood bank activity, we could therefore assume that irregular red blood cell screens were ordered for obstetrical follow up. Anti –D is the unique clinically significant alloantibody found in this study. This is not surprising considering that very low prevalence (0,1/1000) of other clinically significant antibodies have been found among 3000 Zimbabwean women attending an antenatal clinic in 199610 . However, it could be assumed that, since anti-D is the most frequent alloantibody responsible for obstetrical complications, antibody screen is mainly prescribed to D-negative women. This hypothesis is confirmed with the high prevalence of D-negative (86%) among the 50 women having had both D-phenotype determination and irregular antibody screening during the study period. The prevalence of anti-D in the study population was high: 4% (CI 95%: 1.9 – 7.5). This could be explained by the representation of women submitted to the test. Antenatal antibody screening is generally recommended at least once for all pregnant women, and should be repeated for D-negative pregnant women 12 . This does not seem to be the case in our study considering the low number of tests (225) requested during the study period with only 3 tests repeated. It is more surprising because this particular test is not available in many laboratories in the country. Therefore we suggested that irregular antibody screen is requested mainly to Dnegative women to find out the reason of obstetrical complications. Hence the high rate of anti-D in our study. Since parity increases with age 13 among Cameroonian women, anti-D rate should be expected to rise with age. Surprisingly, anti-D rate was not significantly different among the age groups in our study (p=0.82).4,13 Anti-D frequency was rather found to be high among adolescent women of reproductive age, illustrating that D-alloimmunization occur early in life. These observations raise issue of Dalloimmunization route among Cameroonian women, and shows that early pregnancies are probably not the only way of D alloimmunizations. Therefore it could be worthwhile to explore other routes such as unsafe blood transfusions as regards women’s D alloimmunization. Women of reproductive age account for 54% of all requests received for D phenotype determinations. The frequency of D-negativity observed among women in our study is one of the highest described for African or Black people 1,7,8,10. To find out the reason of this difference, we looked at D-negativity rates by age groups related to fertility. Dnegativity rate was found to significantly decrease with age from 18,8% for adolescent women to 7,8% for the older women of the study group (p=0,001). Dnegativity rate among women of 35 to 44 years is similar to the one described for Black people 1,7,8,10 (7.8%), while Dnegativity rate of adolescent women (1519 years) is similar to the one found 6,7,8 among Whites. One of the reasons we could suggest for this difference is that D-negative phenotype are confirmed in our laboratory in order to exclude weak D mainly for first pregnancies. Further studies are suggested to determine if this difference is observed in the general population. Only 50 women had both irregular antibody screening and D-phenotype determination during the study period. This small overlap did not allow analysing the link between anti-D rate and D allele distribution in this study. To conclude, it was found that Anti-D is the unique significant alloantibody identified among Cameroonian women of reproductive age at a rate of 4%. This high rate not related to high number of pregnancies raises the concern of Dalloimmunization route among Cameroonian women. D-negativity rate is also found to be very high at 14.3% and decreases with age; an observation which needs to be explored by further studies. References
The following images related to this document are available:Photo images[rh09034t1.jpg] [rh09034t2.jpg] [rh09034t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}