 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 53-69 ORIGINAL RESEARCH ARTICLE Modeling Contextual Determinants of HIV/AIDS Prevalence in South Africa to Inform Policy Modélant les déterminants contextuels de la prévalence du VIH/SIDA en Afrique du Sud pour informer la politique Oumar Bouare* For correspondence: *AEM,2, rue de la Convention, 75015 Paris, France. Email: Obouare@hotmail.com ABSTRACT There is a voluminous literature on HIV/AIDS and South Africa. However, no study focuses on the modeling of contextual factors concerning HIV/AIDS prevalence in South Africa. In this paper, two models of contextual behavioral risk factors of HIV/AIDS prevalence were developed so that policy makers can be alerted to the key variables in order to help curb the spread of the disease. It was found that fearlessness/low-perception, poverty and hopelessness risks are determinants of an active risk factor. While the latter and passive risk factor (i.e. gender dependency) are the determinants of HIV/AIDS prevalence. As a result, it was argued to go beyond the KABP determinant studies to focus on contextual behavioral risk factors and pointed out that further research is needed on the limit of contextuality of risk factors. In conclusion, policies were suggested to help curb the spread of HIV/AIDS (Afr J Reprod Health 2009; 13[3]:53-69). RĖSUMĖ Il existe un gros volume de documentation sur le VIH/SIDA et l’Afrique du Sud. Toutefois, il n’y a pas d’étude consacrée à la modélisation des facteurs contextuels concernant la prévalence du VIH/SIDA en Afrique du Sud. Dans cet article, nous avons élaboré deux modèles des facteurs de risque contextuel du comportement de la prévalence du VIH/SIDA afin d’avertir les décisionnaires sur les variables clé pour aider à réduire la propagation de la maladie. On a trouvé que l’intrépidité/la faible perception, la pauvreté et des risques de désespoir sont les déterminants d’un facteur de risque actif. Alors que le second et le facteur de risque (c’est-a-dire la dépendance du genre) sont les déterminants de la prévalence du VIH/SIDA. En conséquence, nous avons proposé qu’il faut dépasser les études des déterminants selon KABP pour mettre l’accent sur les facteurs de risque contextuel du comportement; nous avons indiqué qu’il faut des recherches supplémentaires sur la limite de la contextualité de facteurs de risque. En conclusion, nous avons suggéré des politiques qui permettront d’aider à la réduction de la propagation du VIH/SIDA (Afr J Reprod Health 2009; 13[3]:53-69). KEYWORDS: HIV/AIDS; determinants; contextual behavioral risk factors; contextual non-behavioral risk factors Introduction AIDS has become the single largest cause of disease/death in Africa, exceeding malaria.1 According to the UNAIDS Global Report 2000, 19.9% adults in South Africa are infected with HIV/AIDS, while ONUSIDA reported in 2008 that 18.1% of them are infected.2,3 There is a voluminous literature on HIV/AIDS and South Africa. However, no study focuses on the modeling of contextual behavioral risk factors concerning HIV/AIDS prevalence in South Africa. In this paper, two models of contextual behavioral risk factors of HIV/AIDS prevalence were developed so that policy makers can be alerted to the key variables in order to help curb the spread of the disease. An overview of behavioral determinants of HIV/AIDS and preventive strategies will shed some light on the issue. As stated in UNAIDS Global Report 2000 and ONUSIDA 2008 Report, HIV infection in South Africa is largely heterosexually transmitted.2,3 As a result, prevention strategies concerning the transmission through sexual intercourse focus primarily on personal/individual behavior.4 The rationale has been that in the absence of a cure for AIDS the spread of the epidemic could be controlled if individuals were able to adopt preventive strategies such as using condoms and limit their number of sexual partners. The widely used strategic frameworks for the development of HIV/AIDS preventive strategies have historically been cognitive behavioral models and include the health belief model of Rosenstock, the model of reasoned action of Fishbein and Ajzen, the model of planned behavior of Ajzen, and the social cognitive model of Bandura.5-9 These theoretical models also guided most of the determinant studies which formed a basis for most interventions with a dominant focus on individual aspects of a particular behavior, i.e. knowledge (K), attitudes (A), beliefs (B) and practices (P), in other words behavioral intentions and behavior, better known as KABP-studies. Cognitive theories of behavior risk assume that individuals will calculate and assess their risk in performing a particular behavior. Thus, induced actions to reduce the risk are seen as reasoned or rational behavior. In contrast, the engagement in risky behavior is seen as irrational behavior. Efforts to change behavior are therefore directed at changing the cognition of a particular behavior, namely the beliefs, knowledge, attitudes, perceptions and practices with regard to the behavior in question. These theories view risk perception and behavior change as an individual rational decision-making process based on the perceived costs and benefits of risk-related action. Individuals are seen as transformers of information with their different cognitive schemas acting as filters through which information is interpreted and acted upon. Despite high knowledge scores on HIV/AIDS in general and with regard to transmission modes, it seems that risky sexual practices in South Africa have not been significantly reduced.10-13 It should be noticed, however, that in a more recent study some changes in sexual behavior in South Africa with 11% of the population which are HIV positive was reported by Shisana and Simbayi.14 This is also echoed by Williams et al. and Pettifor et al. who reported limited changes in sexual behavior in South Africa.15,16 The question then is to look for other determinants of HIV/AIDS prevalence, namely the determinants among contextual factors. In the first part of the paper, we present the materials and methods. In the second part, we report the results. This is followed by the discussion in the third part. In the fourth part, the conclusion and policy implications are presented. Materials and Methods This section consists of two parts: materials and methods. Its objective is in twofold. First, it is to examine whether the fearlessness/low-perception, poverty and hopelessness risks are determinants of the active risk factor; and second, whether the passive risk factor, i.e. gender dependency and the active risk factor are broad risk factors or determinants of HIV/AIDS prevalence in South Africa. The population of study is the South African population which is divided among 9 provinces or sample size of the observations. The study of course should be seen in the context of the follow-up of Apartheid era. Era in which there was racial discrimination against black, colored and Indian people in terms of employment, education, residential location and wealth acquisition, and gender discrimination against black, white, colored and Indian women in terms of employment and wealth acquisition. Materials The materials we examine are composed of 5 South African contextual factors which induced risky sexual behaviors in each of South Africa’s 9 provinces and its HIV/AIDS prevalence in each province. In this section, we present the rationale for the 5 contextual factors, their descriptions and how the data were collected. Rationale The inability of preventive strategies to significantly change the behavior of people who have regular and non-regular sexual partners or only non-regular sexual partners and do not use condoms during sexual intercourse in South Africa, i.e. people whose sexual behavior exhibits “HIV/AIDS active risk factors” or simply the “active risk factor”, could be related to the fearlessness/low perception, poverty and hopelessness risks. For example, people do not always make cognitive risk assessments when they are fearless nor when they make decisions about sexual behavior. Similarly, people might not value their own life as the highest when other circumstances or belief such as a code of honor motivates their behavior. This could happen, for instance, when a person does not want to use condoms during risky sexual behavior. A person’s risky sexual behavior should therefore be viewed in a similar way as fearlessness to engage in a high risk behavior knowing that its outcome could be death. However, this risky sexual behavior could also be due to a low perception of a high risk behavior.16 This risky behavior might be derived from a multitude of beliefs and contextual factors, which cannot necessarily be understood in terms of a risk assessment. The fact that behavior is not only located within the individual will, but also develops out of choices among available options, is often neglected. These choices are determined by the demographic, social, political, economic, and physical environments.17 Thus, consideration should be given to these dimensions of the HIV epidemic that provide the contexts for HIV risk and preventive behaviors in general and to the fearlessness/low-perception risk in particular.18,12 Despite the growing concern for the role of contextual and cultural issues in HIV/AIDS, these issues have not been adequately researched.19 Although Hargreaves et al. reported on socioeconomic issues,20 further HIV/AIDS research in the relationship between the individual and society, which have been identified as under-researched areas by UNAIDS,19 is still needed. As a result, another contextual mediator of the HIV/AIDS pandemic, namely poverty, needs some consideration. The role of poverty in the spread of HIV/AIDS in Southern Africa is well documented.22-24,20 The economic deprivation of many Africans in South Africa has been seen as leading to social ills such as violent crimes, prostitution and rape, the latter two facilitating the spread of HIV.23 A possible solution to the poverty-HIV/AIDS hypothesis was provided by Kawachi et al.,25 who isolated social capital as a more likely causal factor in health inequalities.i However, although the explanation provided by social capital is conceptually appealing as far as health inequalities are concerned, poverty remains a tangible manifestation of low or no social capital as well as the reflection of the inadequacy of social systems. Thus poverty should remain an important factor that needs to be taken into account in a strategy to reduce the spread of HIV/AIDS. Social indicators are also relevant when assessing social change processes, for example those related to people's perceptions of well-being. Measurements of feelings of hopelessness could offer insight into the impact of environmental or contextual factors on the individual and the milieu from which HIV/AIDS related-behaviors derive. Feelings of hopelessness are not only a reflection of people's psychological state, but also reflect their social systems, i.e. the socio-economic, political and cultural contexts in which individuals operate. In the current social structures with their multitude of stressors, many people might find it difficult to give meaning to their lives and therefore struggle to see a purpose.28 Unless they feel that they have a reason to live and work for, it cannot be expected that they will care for themselves and others. As a result, a culture of hopelessness contextualizes the practice of risk-taking behavior. Therefore, it can be argued that people who feel hopeless and have no purpose in their life or future expectations are less likely to protect themselves from getting HIV/AIDS than people who are hopeful and have a purpose and future expectations. The role of hopelessness as a reflection of disintegrated social systems and its association with HIV/AIDS have received very little attention. Meyer-Weitz and Steyn and Abdool Karim reported that feelings of hopelessness as well as the absence of a future purpose contribute to risky sexual behaviors among the youth, which in turn contribute to the HIV/AIDS epidemic.29,30 In addition, people who feel fatalistic about contracting AIDS have been found to be less likely to change their behaviors to prevent HIV/AIDS infection.28 Therefore, some consideration needs to be given to hopelessness when one intends to reduce the HIV/AIDS active risk factor. The HIV/AIDS active risk factor, with fearlessness/low-perception, poverty and hopelessness risks as determinants, needs to be contrasted with the passive risk factor, i.e. gender power relations or the dependence of women on men in the spread of HIV/AIDS. Although the socio-cultural aspects of gender power relationships and their association with women's vulnerability for HIV/AIDS have been studied, little attention in terms of quantitative study was paid to women's economic dependence on men as a determinant for HIV/AIDS. The majority of South African women are either not employed or are employed in low-paid jobs and thus often have to rely on men as the primary breadwinners.31,22 Because of this situation, women engage in casual sex when their partners are away for a while or in sex work for economic support and to ward off starvation for them and their children. 30,32-35,23 Their economic dependence is further exacerbated by migratory patterns. 36 Rural women are often abandoned by their male partners when the latter move to work in an urban area. Their partners often take other wives and have children with them in their new environment. This prevents the men from going back to their first wives or to send money to them as they might previously have done.33,37, 39 The economic hardship that many women face, especially those with children, could drive them to have casual sex or to become sex workers and thus increase their risk of HIV/AIDS infection. In addition, migratory labor could contribute to an unequal male:female ratio especially in rural areas, which could render women more vulnerable for HIV risk because of greater possibilities of exploitation due to competition among women to have available men. This unequal male:female ratio also features in South African demographic in which there are by and large more women than men in each racial group.40,41 In this context, dependent women, who would like to keep their partners, would be less likely to insist on condom use even when they are aware that their partners have other women.12,42 It was reported that sex workers in general experience a powerlessness when they insist that their customers use condoms.43 Clients are often also willing to pay more for unprotected sex.44,23 The unequal gender-power relations of male dominance and sexual prowess are further reinforced by the economic and emotional dependency of especially women with children.12,45-47 The economic dependency of women on men not only increases their own HIV risk but subsequently may also fuel the epidemic. However, there is an absence of information about the role of women's economic dependency on men and its association with HIV risk and HIV prevalence. Therefore, women’s dependency on men needs to be taken into account when one wants to reduce the spread of HIV/AIDS. It emerges from the literature review that little empirical attempt has been made to go beyond the KABP determinant studies, and to empirically investigate nationally the role of other socalled contextual or environmental factors such as fearlessness/lowperception risk, poverty risk and hopelessness risk on the HIV/AIDS active risk factor, which is often seen as fueling the HIV/AIDS pandemic. Neither has an attempt been made to directly link the HIV/AIDS active risk factor and the dependence of women on men to HIV/AIDS prevalence in South Africa. Therefore, our study seeks to address these issues and suggest some policies in order to help curb the spread of the disease. However, it should be pointed out that our study is not concerned with contextual non-behavioral risk factors, such as prevalence of sexually transmitted infections other than HIV/AIDS, state of the immune system, health status, general population prevalence, population viral load, and nosocomial infection, which influence HIV prevalence. Description The “fearlessness risk” is characterized by the risk some people take by engaging in sexual intercourse with non-regular multiple partners without using condoms. As stated before, we labeled it “fearlessness risk” because it is similar to the risk a fearless person takes while knowing that its outcome could be death. However, some people who have a low perception of high risk sexual behavior could engage in sexual intercourse with non-regular multiple partners without using condoms. This was reported by Pettifor et al. in the South African youth survey. 16 Therefore, this risky sexual behavior may be called fearlessness/lowperception risk. “Poverty risk” is the risk poor people take in engaging in unprotected sexual intercourse due to the lack of financial resources. This occurs in the context of their life circumstances, which include the lack of money to buy condoms or the lack of information concerning the existence of social services in which they can obtain condoms free of charge or offering their bodies for financial reward in order to make ends meet. The “hopelessness risk” is the risk some people take in valuing more an immediate sexual reward than their future expectations of improvement or achievement in South Africa. This valuation of immediate sexual reward may occur in a context in which they lack a purpose in life. The “active risk factor” is the risk taken by people who have regular and non-regular sexual partners or only nonregular sexual partners and do not use condoms during sexual intercourse. While the “passive risk factor”, i.e. gender dependency or, more precisely, the risk taken by women because of their dependency on men due to their greater number and smaller income. Data The collection of data started in South Africa in 2003. From the nationwide survey that was conducted by the Human Sciences Research Council (HSRC),48 we collected data on ARF (the active risk factor), NH (the number of hopeless people) and NFLPR (the number of people taking the fearlessness/lowperception risk) in the nine provinces, namely KwaZulu-Natal, Mpumalanga, Gauteng, Free State, Western Cape, Eastern Cape, Northern Cape, North West and Limpopo (the new name of the Northern Province).ii The data required to compute the HAP (HIV/AIDS prevalence)iii was collected from the Department of Health and Department of Social Development publications,11,49 and those needed to compute the GDR (the gender dependency ratio) and RPI (the relative poverty income) were collected from Statistics South Africa publications.40,41 ARF was measured by the number of people in each province who had regular and non-regular sexual partners or only non-regular sexual partners and who did not use condoms when they engaged in sexual intercourse. NFLPR was measured by the number of people in each province who had non-regular multiple partners and do not use condoms in sexual intercourse. RPI was measured by the ratio of the income of a province to the income of the poor in that province. Relative poverty is of particular interest because poverty is dependent on the environment in which one lives. In addition, we have chosen province as a category instead of the nation in order to remain consistent with the other variables. NH was measured by the number of people in each province who did not have great future expectations or no future expectations for themselves in South Africa. The data were collected from a four-point scale questionnaire item on hopelessness in South Africa in the HSRC national survey.48 The number of respondents in each province who stated that they did not have great future expectations or no future expectations for themselves in South Africa were put into the category number of hopeless people of the province. HAP was measured by the number of people who were infected with HIV/AIDS in each province. GDR was measured by the sum of the ratios of the number of women to the number of men in each racial group plus the sum of the ratios of their incomes. As a composite variable, GDR captures the proportion of women to men, that of their incomes and the segmentation by racial group in the country. GDR and ARF were also computed for each province. Methods This section consists of two parts. In the first part, we specify the two regression equations. In the second part, the empirical study, we present five hypotheses which will be tested with the Ordinary Least Square (OLS) technique.v Models The specification of the first model is as follows: ARFi = p + q.NFLPRi + r.RPIi + s.NHi , i = 1,2,…,9 (1), where 9 = n is the number of provinces; ARF (the active risk factor) is the dependent variable; NFLPR (the number of people taking the fearlessness/lowperception risk) is the first independent variable; RPI (the relative poverty income) is the second independent variable; and NH (the number of hopeless people) is the third independent variable; p is the constant; and q, r and s are the coefficients of NFLPR, RPI and NH that will be estimated. The specification of the second model is as follows: HAPi = a + b.GDRi + c.ARFi ,i=1,2,…., 9 (2), where 9 = n is the number of provinces; HAP (HIV/AIDS prevalence) is the dependent variable; GDR (the gender dependency ratio) is the first independent variable; ARF, the second independent variable, is the same as before; a is the constant; and b and c are the coefficients of GDR and ARF that will be estimated. The estimates of the coefficients of the two models will tell us whether our selected variables or contextual factors are relevant, i.e. whether the fearlessness/low-perception, poverty and hopelessness risks are determinants of the active risk factor, and whether passive risk factor (gender dependency) and the active risk factor are determinants of HIV/AIDS prevalence in South Africa. Empirical study The study was conducted in South Africa. In this section, we state five hypotheses and report the results. The five hypotheses which will be tested are as follows:
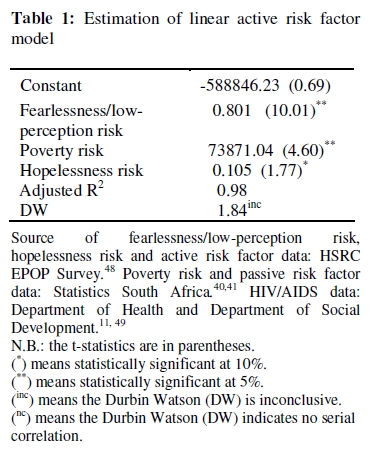
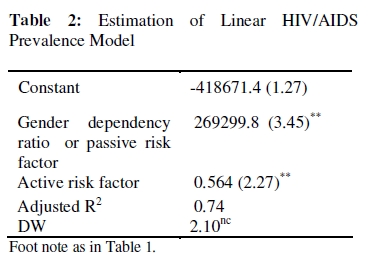
Results Estimates of the coefficients of the independent variables of the two models are in Table 1 and Table 2 respectively. The fearlessness/low-perception, poverty, and hopelessness risks explain 98% of the active risk factor, i.e. the adjusted R2 = 0.98. All the coefficients of the independent variables have the expected positive sign. The coefficients of fearlessness/low-perception risk and poverty risk are statistically significant at 5% level of significance. While the coefficient of hopelessness risk is statistically significant at 10% level of significance. The Durbin Watson, DW = 1.84, is inconclusive at 1% as well as at 5% level of significance. This makes fearlessness/low-perception, poverty and hopelessness risks the main determinants of the active risk factor. The gender dependency ratio (i.e. the passive risk factor), and the active risk factor explain 74% of HIV/AIDS prevalence in South Africa, i.e. the adjusted R2 = 0.74. All the coefficients of the independent variables have the expected positive sign. The coefficient of the passive risk factor and active risk factor are both statistically significant at 5% level of significance. The Durbin Watson, DW = 2.10, indicates that there is no serial correlation. This makes the active and passive risk factors the main determinants of HIV/AIDS prevalence. In other words, our selected contextual factors are relevant. Discussion The discussion revolves around four issues. First, the empirical investigation of the so-called contextual or environmental factors of equation (1) in Table 1 have a positive impact on the active risk factor. In relation to the first hypothesis, it is clear that if the fearlessness/lowperception risk increases, i.e. the number of people who have non-regular multiple partners and do not use condoms in sexual intercourse increases, the risky sexual behavior increases. In other words, the active risk factor will increase. Concerning the second hypothesis, this result may be due to the fact that poor people by and large engage in risky sexual behavior because of the lack of financial means to make ends meet or because they lack the knowledge to protect themselves against HIV/AIDS. This is supported by the literature.21-24,48 With regard to the third hypothesis, this result may be due to the fact that hopeless people by and large engage in risky sexual behavior because they do not care for themselves or others. This is also supported by the literature.28-30 Similarly, the gender dependency ratio and HIV/AIDS active risk factor of equation (2) in Table 2 have a positive impact on HIV/AIDS prevalence in South Africa. Concerning the fourth hypothesis, it is clear that if women outnumber men and depend more on them for financial support or engage in sex work because they are destitute, they may turn a blind eye on their partners’ risky sexual behavior in order to keep them. This is also supported by the literature. 37-39, 12, 33, 43-46, 35 With regard to the fifth hypothesis, again it is clear that an increase in the number of people who have regular and non-regular sexual partners or only nonregular sexual partners and who do not use condoms when they engage in sexual intercourse results in the spread of HIV/AIDS, i.e. in the increase in its prevalence. Second, the technique used in this study can be applied to that of other sexually transmitted diseases. Third, it should be pointed out that there may be a colinearity of independent variables in Table 1. This may be due to an interaction between poverty and hopelessness risk factors because some poor people who are hopeless about their future in South Africa may engage in risky sexual behavior. However, since the Durbin Watson is inconclusive, the interaction between these variables does not reach a level that undermines the study. In addition, there are difficulties that point to areas of future investigation due to the lack of available data on contextual non-behavioral risk factors and the limit of contextuality when one goes beyond the KABP determinant studies. Concerning the absence of contextual non-behavioral risk factors as determinants of the active risk factor in our study, a distinction should be made between active risk factors and contingent risk factors of HIV/AIDS. We call contingent or incidental risk factors the contextual non-behavioral risk factors, such as prevalence of sexually transmitted infections other than HIV/AIDS, state of the immune system, health status, general population prevalence, population viral load, and nosocomial infection, which influence HIV prevalence but have no behavioral risk inducing HIV/AIDS-infection. Whereas active risk factors are contextual behavioral risk factors. Consequently, although these contingent risk factors are determinants of HIV/AIDS prevalence, they are not contextual behavioral risk factors as far as HIV/AIDS-infection is concerned. Moreover, the fact that fearlessness/ low-perception risk, poverty risk and hopelessness risk explain 98% of the dependent variable (active risk factor) even though contextual non-behavioral risk factors cited above are not part of equation (1), simply indicates that the regression equation is a behavioral equation. As a result, they should not be part of equation (1). However, given that the independent variables of equation (2) in Table 2 explain 74% of HIV/AIDS prevalence, one could of course add to them another independent variable which regroups contextual non-behavioral risk factors in order to account for some of the remaining 26% of the explanation of HIV/AIDS prevalence. We did not do so because we simply did not have data for these risk factors. Going beyond the KABP determinant studies, which rest on cost-benefit risk assessments, to focus on behavioral risks induced by contextual factors such as fearlessness/low-perception, poverty, hopelessness and women dependency on men, which cannot necessarily be understood in terms of risk assessment alone, also calls for a discussion on the limit of the contextuality of these factors. Although risky behaviors are inherent to individuals’ decisions in both KABP determinant studies and contextual behavioral risk factors, in the latter, risky behavior is induced or mediated by the context in which individuals live. The lack of knowledge, for instance, resulting from poverty can prevent an individual from seeing the consequences of a decision. That is, the individual may not be aware of the risk associated with a behavior. Thus, poverty may induce or mediate a risky sexual behavior. In contrast, a fearless individual may be fully aware of the consequences or risk associated with a given decision, but could have a clouded mind due to a code of honor during the decision-making process in such a way that no difference would be made between rational and irrational decisions. This is so because the reference upon which the individual makes a decision is affected by fearlessness. As a result, an individual’s fearlessness decision that may be irrational for a fearful or normal individual could be perceived by the individual as a rational decision. Thus, fearlessness may induce or mediate a risky sexual behavior. Similarly, an individual, who has a low-perception of a high risk he or she is taking, may make a decision which seems rational to him or her. In this case, the low perception may induce or mediate a risky sexual behavior. Furthermore, the lack of will of hopeless individuals or dependent women on men for financial support could lead them to engage in irrational decisions which are risky, even though they are fully aware of the riskiness and irrationality of their decisions. Thus, hopelessness and women dependency on men may induce or mediate a risky sexual behavior. It follows that contextuality induces poverty, fearlessness/low-perception and hopelessness risks as well as passive risk or gender dependency, which trigger risky sexual behavior for some individuals while they do not for others; and this is so even though there are other non-risky options for individuals who engage in risky sexual behaviors. Thus, it seems that contextual behavioral risk factors, such as poverty, fearlessness/ low-perception, hopeless-ness and gender dependency, operate as mediators which divide individuals into two groups. The risk group for which the mediators trigger a risky sexual behavior and the non-risk group for which they do not. Given that poverty, fearlessness/lowperception, hopelessness and passive risks, i.e. the contextual behavioral risk factors, divide individuals into two groups, it could be investigated whether there is a threshold of a set of stimulating conditions for the risk group above which the individuals who belong to this group engage in risky sexual behaviors. This threshold could be the limit of contextuality of these contextual behavioral risk factors. But this is beyond the scope of our study. Fourth, the significant finding of the study is the relevance of the estimate of the gender dependency variable in the model in Table 2. To our knowledge, in the literature, this is the first time that a gender dependency variable is introduced in modeling. Conclusion and policy implications This paper identified some contextual behavioral risk factors as determinants of HIV/AIDS prevalence in South Africa as well as those which are determinants of the active risk factor by testing two regression equations. We found that poverty, hopelessness, and the fearlessness/low-perception risks are related to the active risk factor. We also found that the active risk factor and the passive risk factor (i.e. gender dependency ratio) explain HIV/AIDS prevalence in South Africa. Thus, to reduce HIV/AIDS prevalence the policy should consist of reducing the active and passive risk factors. That is, the policy should address the followings:
The first four policies may help reduce the active risk factor, while the passive risk factor may be reduced by the last policy, resulting in a decrease in HIV/AIDS prevalence in South Africa. It should be pointed out that poverty and economic empowerment of women programs, i.e. recommendations 1 and 5, are already part of national health-sector strategies. However, these strategies are not necessarily based on public work policies which may have a lasting impact on the communities. Thus, this paper provides policy tools that will enable policy makers to help curb the spread of the disease. Acknowledgement This author benefited from the communication with Anna Meyer-Weitz when we were colleagues at the Human Sciences Research Council (HSRC), which is the South African think tank in Pretoria. End Notes i Social capital is measured by levels of trust of fellow citizens and their extent of membership in various voluntary groups and associations. It is argued that income inequality exerts its effect only through the social capital variable. Income inequality is thus a reflection of low social capital and it is the latter that causes the increases in mortality. Furthermore, Lomas argued that a solution to inequalities in health is to be found in the improvement of the integrity of social systems in which we live.26 The adequacy of South Africa's current social systems to foster health and well-being and to reduce the spread of HIV/AIDS in particular is thus questioned. The South African disintegrated social and support systems are evident in the increasing levels of poverty, unemployment, crime, violence, prostitution and racial tension.23 Colvin stated that the poor public health system and poor education in the prevailing socio-economic context contribute to the spread of HIV/AIDS.24 Therefore, it can be argued that social change, defined as the alteration in social phenomena at different levels of human life from the individual to a community level, needs attention as a HIV/AIDS prevention strategy even if the interface between HIV/AIDS infection and social capital is a complex area that defies easy generalization.27 ii The HSRC has for several years been conducting regular national surveys on public opinion on a range of topics, including economic and political issues. The study population in the surveys consists of South African residents aged 18 years or older, in all nine provinces. For the 2002 survey a sample of 2704 respondents was selected throughout South Africa in clusters of eight households situated in 338 primary sampling units and enumerated areas as determined from the 1996 census. In order to ensure adequate representation in the sample from each province and from each of the four dominant racial groups (Black, White, Colored, Indian), the sample was explicitly stratified by province and urban/rural locations. This added up to 18 strata. Disproportional samples were drawn from less populated provinces such as the Northern Cape, Free State, Mpumalanga and North West. Households were drawn from the sampled clusters with equal probability. One respondent was randomly drawn from the eligible members of the household (by applying a grid). In this way a sample of households was selected and one respondent aged 18 years or older was selected from each household. The realized sample was n = 2530, which is slightly less than the intended sample of 2704. In terms of province and population (racial) group, the spread was sufficiently wide to facilitate statistical generalizations about opinions prevailing within each province and among persons of each of the four main population groups. Each case was then weighted so that the resultant weighted dataset would approximate the distribution of the population of South Africa in terms of population group, province, gender and educational qualification. The survey instrument comprised a structured, intervieweradministrated questionnaire containing questions compiled by different researchers on a variety of themes. The questionnaire was divided into different topics and the interviews with respondents lasted 60 to 90 minutes. Different items from the Beck’s scale of hopelessness were adapted and included five items used previously as a scale by Beaumont (Department of Psychology, The Open Polytechnic of New Zealand, June 2001). The participants were asked to describe themselves on a four-point scale, ranging from ‘very well’ to ’not at all’, in terms of feelings of unhappiness, likeness to cry, and sense of hopelessness. Specific questions were also posed relating to HIV/AIDS risk behavior, namely the number of regular and non-regular sexual partners, only non-regular sexual partners, non-regular multiple partners and do not use condom. The response options were Yes = 1 and No = 0. We multiplied the percentage of respondents who said “Yes” for the categories hopelessness risk , fearless/low-perception risk and active risk factor in each province by the number of inhabitants of the corresponding province to determine the data for the variables NH (number of hopeless people), NFLPR (number of people taking the fearless/low-perception risk) and ARF (number of people engaging in active risk factor) for the 9 provinces. iii We multiplied the percentage of HIV/AIDS prevalence in each province obtained from the Department of Health publications by the number of inhabitants of each province obtained from the Department of Social Development in order to have the data of the variable HAP (the number of people infected with HIV/AIDS). iv The number of men and women of each racial group as well as their respective incomes in each province obtained from Statistics South Africa enable to determine the data of the variable GDR (gender dependency ratio) for each province, which is the sum of the ratios of the number of women to the men in each racial group plus the sum of the ratios of their incomes. From the publications of Statistics South Africa we also obtained the income of each province and that of the poor in each province. This enables us to compute the data of the variable RPI (relative poverty income) for each province, which is the ratio of the income of a province to the income of the poor in that province. Given that GDR and RPI are ratios whose magnitudes are far smaller than the magnitudes of the other variables, in order that the left hand-side and right handside of the two linear regression equations balance out, one should expect that the coefficients of GDR and RPI in Table 2 and Table 1 be far greater than the coefficients of the other independent variables. v The OLS technique should not be confused with the Logistic regression technique. In contrast with the Logistic regression technique, in the OLS technique no characteristics of the sample size or variables are required before running the regression. Only the number of observations (n) for each variable, which should be equal for all of them, and the number of units or the amount of value taken by the variables are needed. Moreover, the number of units or the amount of value taken by the variables for different observations are not the same, and the data on the variables need not be from the dataset of the same sampling. Additionally, to have the best fitted regression equation, the OLS software computes by itself the average value of each variable as well as its minimum variance or the minimum distance of the data to its average value. This is why the OLS studies do not display the characteristics of the variables or those of the sample size of the population under study. Econometric textbooks on OLS regression technique do not display them either, because they are irrelevant. The OLS technique aims at determining whether the independent variables explain the dependent variable and whether the coefficients of the independent variables are statistically significant. References
The following images related to this document are available:Photo images[rh09035t1.jpg] [rh09035t2.jpg] |
| |||||||||

{kind=link}
{kind=link}