 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
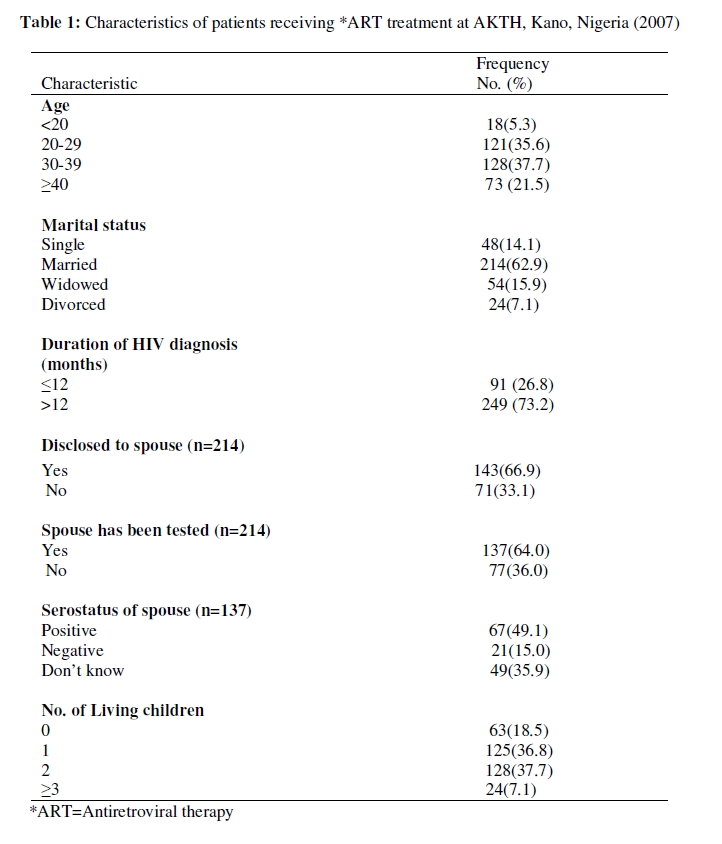
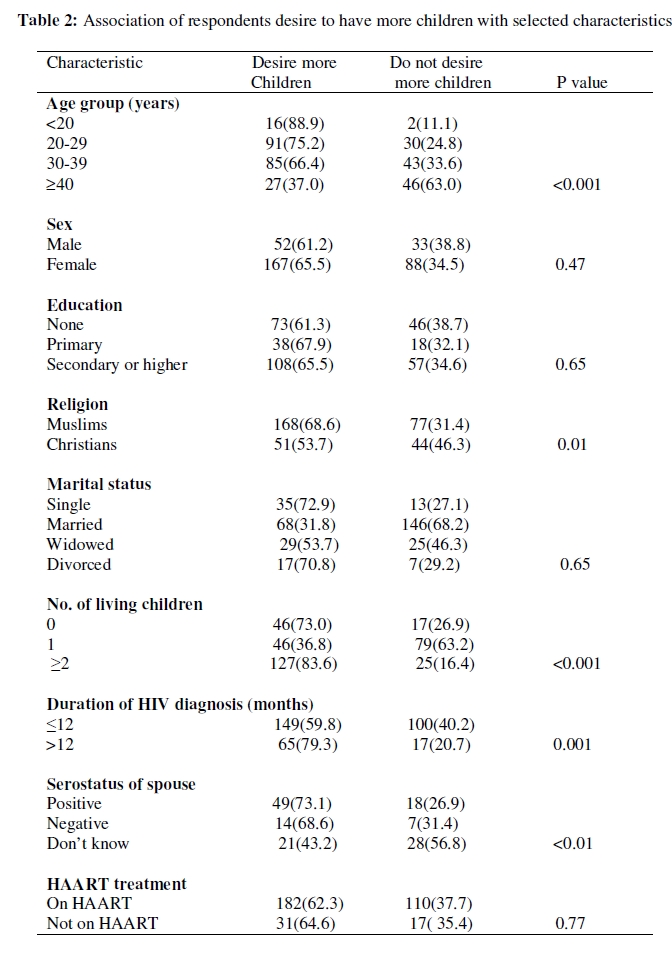
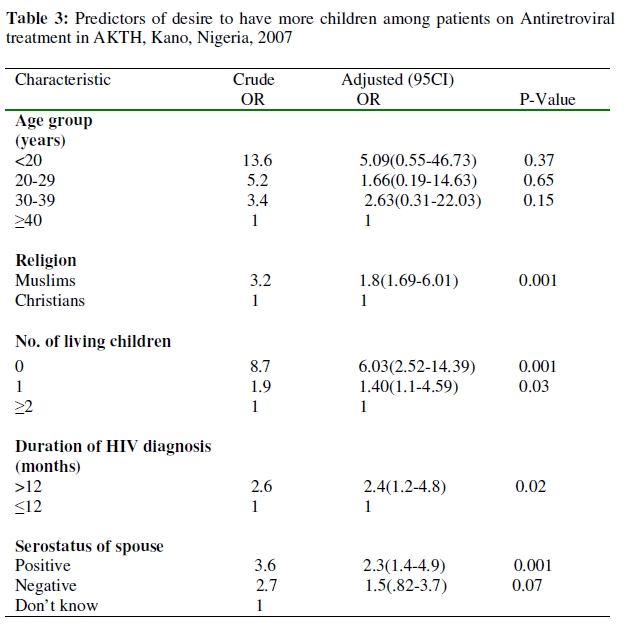
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 71-83 ORIGINAL RESEARCH ARTICLE Correlates of Fertility Intentions Among HIV/AIDS Patients in Northern Nigeria Corrélats des intentions de la fécondité chez les patients séropositifs au nord du Nigéria Zubairu Iliyasu1, Isa S Abubakar1, Mohammed Kabir1, Musa Babashani2 and Faisal Shuaib3, Muktar H Aliyu4 1Department of Community Medicine, Aminu Kano Teaching Hospital & Department of Community Medicine, Bayero University Kano, Nigeria. For correspondence: Dr. Zubairu Iliyasu, MBBS, MPH, FWACP, Department of Community Medicine Aminu Kano Teaching Hospital, PMB 3452 Kano, Nigeria. Email: ziliyasu@yahoo.com ABSTRACT Little research has been conducted regarding the reproductive intentions of people living with HIV/AIDS (PLWHA) in northern Nigeria. We studied reproductive desires and their predictors among 340 PLWHA receiving care at Aminu Kano Teaching Hospital. Of all respondents, 60(70.6%) of males and 177(69.4%) of females were sexually active. Only 65(19.4%) of them used condoms. One hundred and sixty seven females (65.5%) and 52(61.2%) males expressed a desire to have more children. Out of these, 16(7.3%), 106(48.4%) and 88(40.2%) wanted to have one, two and three or more children respectively. Significant predictors of higher fertility desires were; religion (OR=1.8), duration of diagnosis (OR=0.42), low parity (OR=6.03) and awareness of partner’s serostatus (OR=2.3). A large proportion of the HIV-positive individuals in the study were sexually active, desired to have children, and wanted to use family planning, indicating unmet need for reproductive health counseling in general and family planning in particular (Afr J Reprod Health 2009; 13[3]:71-83). RĖSUMĖ Peu de recherche a été menée à l’égard des intentions de reproduction chez les gens séropositifs au nord du Nigéria. Nous avons étudié les désirs de reproduction et leurs indices chez 340 personnes séropositives qui se faisaient soigner à l’hôpital universitaire Aminu Kano. Parmi les interviewés, 60 (70,6%) des hommes et 177 (69,4%) des femmes étaient sexuellement actifs. Il n’y avait que 65 (19,4%) parmi eux qui utilisaient des préservatifs. Cent soixante-cinq femelles (65,5%) étaient sexuellement actives et 52 mâles ont exprimé le désir d’avoir encore des enfants. Sur cette population, 16 (7,3%), 106 (48,4%) et 88 (40,2%) voulaient en avoir encore un, deux ou trios enfants respectivement. Des indices des désirs de la fécondité plus élevée étaient la religion (OR= 1,8), la durée du diagnostic (OR=0,42), une parité faible (OR=6,03) et une conscience de l’état sérologique (OR=2,3). Une grande proportion des individus séropositifs dans l’étude étaient sexuellement actifs, voulaient avoir des enfants et voulaient se servir de la planification familiale, ce qui a montré un besoin insatisfait pour l’assistance sociopsychologique par rapport à la santé de reproduction en général et à la planification familiale en particulier (Afr J Reprod Health 2009; 13[3]:71-83). KEYWORDS: Fertility desire, PLWHAs, Kano, Nigeria Introduction Of all infectious diseases, the HIV/AIDS pandemic remains the most serious challenge to public health. Globally, over 6,800 persons become infected with HIV and over 5,700 persons die from AIDS everyday.1 The estimated number of deaths due to AIDS in 2007 was 2.1 million worldwide, of which 76% occurred in sub-Saharan Africa.1 Worldwide, Nigeria has the third highest population of people living with HIV after South Africa and India.1 Median HIV prevalence among pregnant women attending antenatal clinics in Nigeria rose from 1.8% in 1991, to 5.4% in 2003. The estimated prevalence was 4.4% in 2005.2 The desire for HIV-infected patients to conceive has been a topic of recent research.3-5 Procreation is a basic human instinct. Expectedly, HIV-affected couples also desire to have children.4,6 Women living with the human immunodeficiency virus (HIV) face difficult decisions regarding childbearing. Despite the risks and challenges, many women with HIV are deciding to bear children. Chen and colleagues found that 28% to 29% of 1,421 HIV-infected adults surveyed desired to have children sometime in their lives.4 HIV-infected subjects cited raising children as a way to give purpose to life.7 In addition, many HIV infected women reported pregnancy and childbirth as a way to regain their sense of womanhood and sexuality, often making childbearing a high personal priority.8 Prior to the advent and availability of antiretroviral therapy, HIV-infected women had a 25% chance of delivering HIV-infected children. This possibility in an environment of limited supply of antiretroviral drugs prompted physicians to recommend bilateral tubal ligation to prevent perinatal HIV transmission.9,10 Between 1991 and 1993, early trials conducted by the Pediatric AIDS Clinical Trial Group (PACTG) found that Zidovudine reduced mother-to-child transmission from 25% to 8%.11 With antiretroviral therapy and elective cesarean section, the risk of perinatal transmission has dramatically decreased to 1% -2%. Recent studies have also demonstrated mother-to-child transmission rates as low as 1% to 2% in women with HIV RNA levels below 1000 copies/ml regardless of mode of delivery, suggesting that perinatal transmission can be prevented in 99% of all cases.10,12,13 In view of these data, health care professionals must balance concerns about the risks of HIV transmission with the patients’ desire to have children.14 Physicians must respect patient rights and autonomy by providing them with information that will allow them make informed reproductive decisions. These decisions and their determinants have been studied in the United States,4 Switzerlandand15 southwestern Nigeria.16 Northwest Nigeria is socioculturally distinct from other regions; therefore, the present study is aimed at assessing the fertility desires and factors that influence reproductive decisions of PLWHA. The study is based on responses from HIV/AIDS patients receiving treatment at a large Teaching Hospital in the commercial nerve centre of northern Nigeria-Kano. The study will improve our understanding of the way multiple factors influence reproductive decisions of PLWHA, thereby informing the implementation of services and health policies that promote and improve the quality of their life. Methods Setting Established in 1988, the Aminu Kano Teaching Hospital is situated in Kano city, the commercial nerve centre of northern Nigeria with over 9 million people.17 It is a 500-bed hospital which receives patients from within Kano, the neighbouring states of Jigawa, Katsina, Kaduna, Bauchi and Zamfara states. The majority of patients are indigenous Hausa Fulani, although the Ibo and Yoruba ethnic groups are well represented. Most of the people are farmers, traders, businessmen and civil servants. The hospital operates a multidisciplinary specialist clinic located at Prof. S.S. Wali centre for HIV/AIDS patients five days a week. Investigations and antiretroviral drugs are provided free of charge to all patients. Study participants The study population consisted of HIV/AIDS patients attending Aminu Kano Teaching Hospital HIV/AIDS specialist clinic from the 1st to the 30th of November 2007. The systematic sampling technique was used. All men and women with HIV, who had made at least one visit to the ART unit, were included in the study. Those clients that were too ill to participate in an interview were excluded from the study. During recruitment, participants were given an explanation of the purpose of the study and asked if they would like to participate. They were assured of confidentiality. Upon approval, the informed consent process was described and participants were asked to read and sign the consent form after all questions were answered. Those without formal western education had the consent translated to them in the locally spoken Hausa language and they elected to thumbprint. Informed consent was secured from each participant. Participation in the study was voluntary and no incentives were provided. Ethical clearance was obtained from the Aminu Kano Teaching Hospital institutional review board. Sample size determination The study was descriptive and crosssectional in design. A sample size of 356 was obtained using the hypothesis method 18 and based on a similar study which found 71.4% of respondents desired to have children.19 Our assumptions were a 95% confidence limit, a 5% margin of error and allowance made for 10% attrition rate (Statcalc, Epi Info version 6). Study instrument and data collection A pre-tested structured intervieweradministered questionnaire containing open and closed ended questions was used. The questionnaire was adapted from one used in an earlier study in southwest Nigeria.16 It was made up of the following moieties: questions on socio-demographic characteristics, HIV diagnosis and treatment, sexual behaviour, childbearing desire, family planning use and contraceptive choice. Revalidation was done at the nearby Infectious disease hospital, Kano. Participants engaged in the latter exercise were invariably excluded from the study. All PLWHA fulfilling the inclusion criteria were interviewed during their exit from the anti-retroviral therapy (ART) units. The interviews were continued until the required number of respondents was obtained. Four Hausa speaking medical students specifically trained in the conduct of interviews collected data. The authors supervised the data collection process. Data analysis The data from the questionnaires were entered and analyzed using SPSS version 12 software.20 Odds ratios (95% confidence intervals) were used to determine the association of different factors with fertility desire and family planning use. Logistic regression analysis was used to assess the relative effect of determinants. Adjustment was made for predictor variables that were significantly related to the outcome variable at the bivariate level. A P<0.05 was considered statistically significant in all tests of significance. Results Socio-demographic characteristics Out of 356 PLWHA approached for the study, 4(1.1%) were excluded from the study due to severe dehydration following chronic diarrhea. Three hundred and forty agreed to participate giving a response rate of 95.5%. The participants consisted of 85 (25.0%) males and 255 females (75%) with a sex ratio of 1:3. The age range of the study participants was 15 to 55 years. The mean age (±SD) of the male and female clients, respectively, was 32.9 (±7.7) and 31.6 (±8.1) years. The majority of the respondents 245 (72.1%) were Muslims most 219 (64.0%) of whom belong to the Hausa/Fulani ethnic group. Other respondents were Igbo 43 (12.7%), Yoruba 25 (7.4%) or members of other minor Nigerian tribes 53(15.9%). One hundred and six respondents (31.2%) were employed privately or by government, while 117(34.6%) were unemployed; 13.1% were housewives, 9.2% were daily labourers, and the rest were self-employed and engaged in different types of work. About 49% of the participants had at least secondary school education, about 35% had no formal education, and the rest had primary school education. Most respondents were married 214 (62.9%), while others were either widowed 54 (15.9%) single 45 (13.2%) or divorced 21 (6.2%). Of the 214 who were married, 143 (66.9%) had disclosed their HIV serostatus to their spouse, and the partners of 137 (64.1%) had had an HIV test. Of those with partners who had tested, almost half had concordant partners 67 (49.1%), while 21(15.0%) had discordant partners. Of all respondents, 60(70.6%) of males and 177(69.4%) of females were sexually active within the preceding 6 months. The sexual partners of sexually active respondents included spouse (86.8%), girlfriends/boyfriends (8.5%), casual partners (3.8%) and commercial sex workers (0.9%) (Table 1). ART treatment and health status The majority of the respondents 292(85.9%) were on highly active antiretroviral therapy (HAART), while 48(14.1%) were not receiving this treatment. The later were on regular follow up every 3 to 6 months. During each visit, clinical history and examination were conducted to monitor for any opportunistic infections. CD4 count was checked and they were given a prescription of co-trimoxazole tablets for Pneumocystis carinii pneumonia prophylaxis. Patients were health educated on positive living. When asked to rate their physical functioning and overall health, 35.9%, 36.8%, 20.0% and 7.4% of those on HAART assessed themselves as very good, good, fair and poor respectively. Only 71(20.9%) respondents reported that they had been counselled about sexuality, family planning and childbearing. When asked about the possibility of transmission of HIV during delivery and breastfeeding, 73.5% and 82.9% of the respondents answered in the affirmative. Two hundred and seventy seven respondents said mother to child transmission was preventable and 311 (91.5%) participants said they knew about the Prevention of Mother-to-Child Transmission (PMTCT) program. Fertility desire One hundred and sixty seven females (65.5%) and 52(61.2%) males expressed the desire to have more children. Out of the 219 (64.4%) who desired to have children, 16(7.3%) wanted to have one child, 106(48.4%) wanted to have two, while 88(40.2%) wanted three or more children. Three of the respondents wanted as many as possible. Univariate analysis showed significant association between desire for children and age, religion, number of living children, duration of HIV/AIDS diagnosis and serostatus of spouse as shown in Table 2. However, multivariate analysis shows that Muslim respondents were almost twice as likely as Christians to desire having children (adjusted odds ratio [OR]: 1.8, 95% confidence interval [CI]: 1.69–6.01). Those diagnosed within the preceding year were less likely to wish for more children compared with those diagnosed for a longer period (adjusted OR: 0.42, 95% CI: 0.21-0.86). Respondents who had no children were more likely to want to have children than those who had at least two children (adjusted OR: 6.03, 95% CI: 2.52-14.39). Furthermore, those that knew their partner’s serostatus were more likely to want children compared to those that were ignorant (adjusted OR: 2.3, 95% CI: 1.4-4.9) as shown in Table 3. There were no significant interactions between the dependent variables. Family-planning use and demand Sixty-two of the PLWHA (18.3%) had ever used at least one method of contraception before their HIV diagnosis; oral contraceptive pills (5.1%), condoms (4.2%) and injectables (3.0%) were the most commonly used contraceptives before HIV diagnosis. At the time of the study, 85 respondents (25.1%) were using different methods of family planning; of these, 65(19.4%) used condoms, while 8(2.4%) used oral contraceptive pills and only 2(0.6%) practiced abstinence. About 31(9.1%) of the respondents had considered abortion for unwanted pregnancy, but this has increased to 140(41.4%) after been diagnosed. Additionally, 125(36.8%) of the respondents considered sterilization as an option for PLWHAs. Out of the 255 respondents who were not using a family planning method during the study period, 45(17.6%) wanted to use family planning in the future. Discussion This study found that a high proportion (64.4%) of people living with HIV/AIDS expressed a desire for having more children. This figure is similar to the finding among PLWHAs in Sagamu, southwest Nigeria 16 (63.3%) but lower than those reported from Maiduguri 19 , northeast Nigeria (71.5%) and among the general population (73%).21 However, it was higher than the proportion of PLWHA that were desirous of reproduction in the United States (28-29%). This shows that being HIV positive modified but did not remove reproductive desires, and diversity existed in reproductive intentions. Some HIV positive individuals wished to avoid pregnancy. Fears of partner and infant infection and having a previously infected baby could deter some individuals from considering having children. Strong desires to experience parenthood, mediated by prevailing social and cultural norms that encouraged childbearing in society is in consonance with what was observed in South Africa.22 Other researchers have reported reasons for such desire to include the fact that PLWHAs considered raising children as a way to give purpose to life.7 In addition, many HIV infected women reported pregnancy and childbirth as a way to regain their sense of womanhood and sexuality, often making childbearing a high personal priority.8 In contrast, those that were not desirous of reproduction cited fear of infecting the child and uncertainty of care if they leave many orphans. Surprisingly, educational attainment and respondents’ sex did not significantly affect their desire for children even on univariate analysis. These variables are known to strongly determine fertility preferences in the general population as observed in the 2003 Nigeria demographic and health survey. 21 The reverse gender discrimination in study participants may be due to the higher opportunity of women undergoing HIV testing as part of PMTCT compared to men. Similarly, the literacy rate of PLWHAs that participated in the present study is higher than the national average. 23 This could be due to selection factors, as education positively influences health-seeking behaviour. Muslim respondents were almost twice more likely than Christians to desire more children. This is a reflection of sociocultural life in the study area. The practice of polygamy is allowed in Islam, which is the predominant religion of the study populace. Apart from polygamy itself, another factor that may increase family size is the ensuing competition between the wives to have as many children as possible, especially sons, as this would increase their share of the husband’s estate and property. It is also noteworthy that a large portion of the study subjects either did not know their partner’s serostatus (35.9%) or were serodiscordant (15%). In addition, more than a third of married respondents (36%) had not disclosed their serostatus to their partners. Individuals in such situations are less likely to take the necessary care to protect their partners or themselves from HIV infection or re-infection, or to prevent vertical transmission to a newborn. The prevention of sexual transmission of HIV within the couple requires HIV testing for each partner and the systematic use of condoms if one of the members is HIV positive or until both partners have been tested HIV negative and adopt safe sex practices. The fact that majority of HIV transmission in developing countries is through heterosexual encounters and most pediatric infections are acquired vertically has implications for programming. Studies exploring the risk of sexual transmission of HIV among couples in sub-Saharan Africa indicate that simple principles of management are unfortunately, rarely implemented.24 High proportions (15.9%) of our respondents were widows/widowers. Studies among the Luos of Western Kenya also indicated high levels of widowhood 25 which is however countered by the unfortunate continued practice of widow inheritance. Consequent upon the HIV/AIDS epidemic, widows are constrained to find new sexual partners; hence, they are unable to fulfill their aspirations for procreation. Evidence suggests widow remarriage rates have fallen due to fear of HIV.30 A quarter of the respondents reported that they were currently using a family planning method, as compared to 18.3% before HIV diagnosis. This is higher than the proportion of women reportedly using a method during the 2003 NDHS (8.9%).21 The most commonly used family planning method before HIV diagnosis was combined oral contraceptive pills as compared to condoms after diagnosis. This is similar to what was found during the 2003 NDHS where the commonest method in use in the general populace was the male condom (3.4%). This may be related to the promotion of condoms among PLWHA and the general public as a dual method to protect from unwanted pregnancy and STI/HIV transmission. One of the family planning methods that have been resisted in Africa for cultural and other reasons is the condom. Poignantly, with the HIV/AIDS epidemic, the resistance is slowly giving way as seen in studies in Zimbabwe and Uganda where 21% and 26% of women respectively reported ever use of condoms for HIV prevention.26,27 There is also evidence that HIV/AIDS has increased the use of contraception. For instance the proportion of HIV positive women using modern contraceptives was 34.5% compared to 17.5% among HIV negative women in Yaoundé, Cameroon 28 and 20.3% compared to 14.8% respectively in Ndola, Zambia.29 This increased contraceptive use was for HIV infected women to meet their objective of reducing their family sizes. The threat of contracting HIV guided the decision by some respondents to produce fewer children than hitherto desired. Concern about the cost of raising children and indeed the welfare of orphans left behind also modulates their reproductive health projects. There are several limitations to this study. The first is the selection of patients attending HIV treatment clinic in a teaching hospital located in a large urban centre in northern Nigeria. The respondents’ characteristics and fertility intentions may differ from those not attending clinics and those living in rural areas. For instance, despite the elimination of cost of antiretroviral drugs in Nigerian government hospitals, differences in utilization of health services may still exist between the poor and the wealthy and between urban and rural dwellers as observed during the NDHS in 2003. 21 In addition, fear of stigmatization could prevent some patients from accessing health care within their community preferring to go to centers away from their community. Furthermore, skewed distribution of VCT sites and health facilities provide undue advantage to urban dwellers in availing themselves of the opportunity of knowing their serostatus and hence attending ART treatment centres compared to their rural counterparts. Secondly, the gender bias in sampling may result from the increased likelihood of HIV testing of women during antenatal care. Finally, questions relating to sexual behaviour and HIV/AIDS may elicit only socially desirable responses in view of the stigma associated with this disease. However, our interviewers assured respondents of confidentiality prior to the conduct of the interview. We are conscious of the fact that our study is hospital based with dominance of urban dwellers and overrepresentation of women leading to sampling bias compared to population based studies. The later are hard to come by except during NDHS. The inclusion of questions relating to HIV infection and fertility in subsequent NDHS will make this picture clearer. This necessitates the need for caution in extrapolating our findings unto the general populace. Nevertheless, our findings underscore the importance of formulating policy and practice guidelines for health workers addressing the provision of culturally sensitive family planning counseling, services and protection of reproductive rights of PLWHA. The policy should; expand access to modern contraceptive methods; ensure that information provision on contraceptive methods is tailored to the needs of PLWHA and protect the right of PLWHA to have children when they want to, and they should be supported to do so without judgment and with access to antenatal, delivery and postnatal care. Conclusion A large portion of the HIV-positive individuals in the study were sexually active, desired to have children, and wanted to use family planning, indicating unmet need for reproductive health counseling in general and family planning in particular. The results of this study, when compared to studies of uninfected women, suggest that HIVinfected women behave similarly in many respects to uninfected women in their childbearing decisions. They have similar desires for motherhood at similar points in their lives. Nevertheless, the family life choices made by these women is influenced and shaped by their serostatus. Balancing this competing desire for motherhood with the desire to protect innocent children from suffering, while at the same time dealing with one’s illness, is a complicated and emotionallytaxing process. Reproductive counseling by HIV care providers needs to be sensitive to all the issues faced by these women. A client-centred approach may be most useful in counseling regarding reproductive decision-making. Available reproductive health services at the ART units do not seem to fulfil the needs and demands of PLWHA. The findings indicate that adequate information on HIV prevention, and counseling about available and practicable reproductive options should be a priority and rendered as part of appropriate family planning and reproductive health services to HIVpositive individuals. Appropriate information, education and communiation materials should be provided for PLWHAs at the clinics. Effective family planning counseling and services should also be provided. References
The following images related to this document are available:Photo images[rh09036t1.jpg] [rh09036t2.jpg] [rh09036t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}