 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
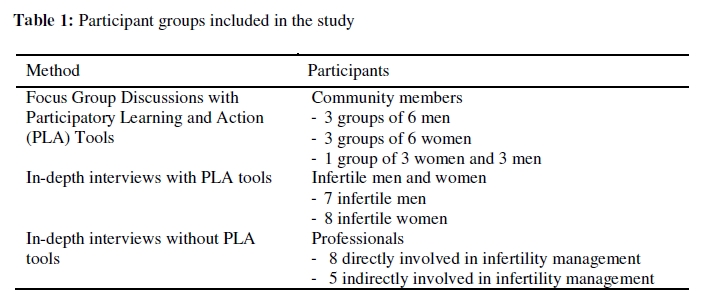
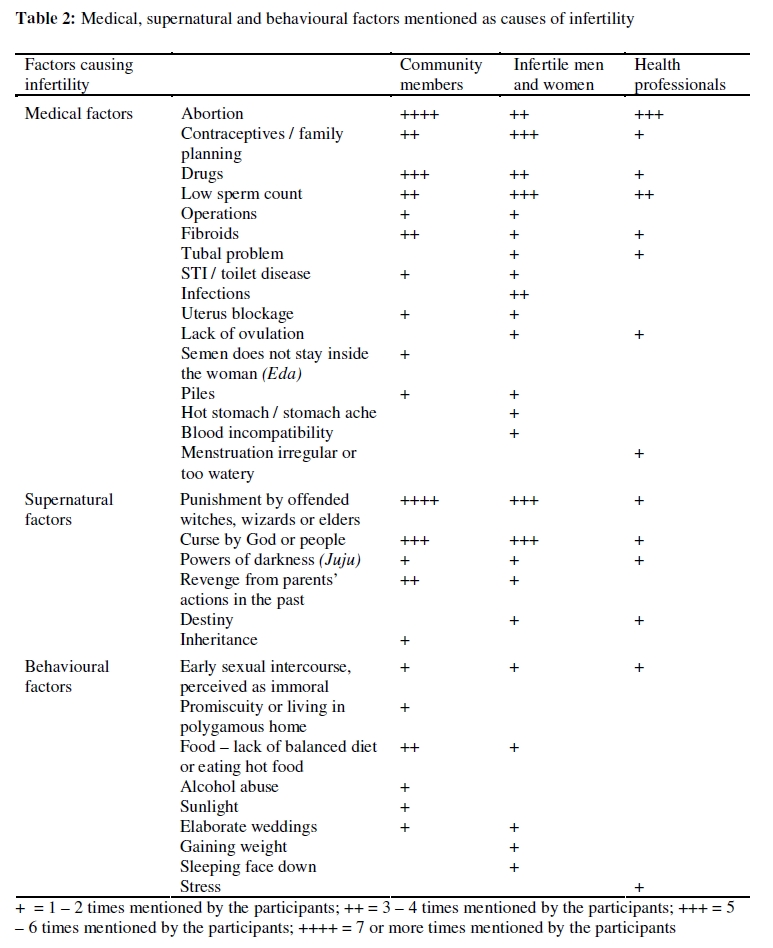
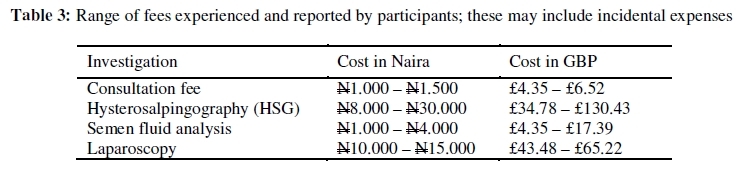
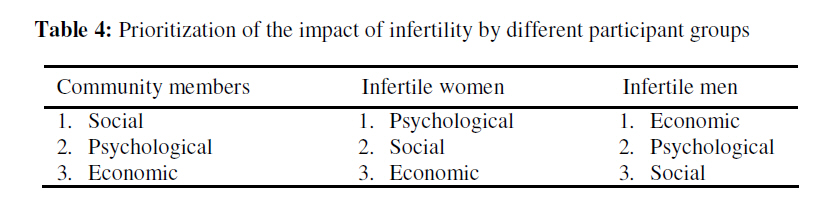
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 85-98 ORIGINAL RESEARCH ARTICLE The Impact of Infertility on Infertile Men and Women in Ibadan, Oyo State, Nigeria: A Qualitative Study Impact de la stérilité sur les hommes et les femmes fertiles à Ibadan, Etat d’Oyo, Nigéria : Une étude qualitative. Sonja L Nieuwenhuis1, Akin-Tunde A Odukogbe2 , Sally Theobald1 and Xiaoyun Liu1 1International Health Group, Liverpool School of Tropical Medicine, UK; *For correspondence: Sonja L Nieuwenhui Email: sonja.nieuwenhuis@hetnet.nl ABSTRACT This study explored the impact of infertility on infertile men and women in Ibadan, Nigeria. The qualitative study design included the application of focus group discussions with community members (7 FGDs, n=42), in-depth interviews with infertile men (n=7), infertile women (n=8) and professionals (n=13). The findings revealed that infertile men and women and community members commonly perceived that contraceptives and abortion cause infertility, as well as supernatural and behavioural factors. Measures to prevent infertility were not well known by the participants. Infertility treatment is sought from a mixture of biomedical, faith-based and traditional service providers. Infertile women prioritize the psychological impact of infertility while infertile men prioritize the economic impact, and reported spending between 55-100% of their income to address infertility. Infertility has a serious social, psychological and economic impact on women and men’s lives. Efforts to reduce the impact should prioritize education on the causes, prevention and treatment of infertility, offer psychological support and ensure an efficient referral system for managing infertility (Afr J Reprod Health 2009; 13[3]:8598). RĖSUMĖ Cette étude a exploré l’impact de la stérilité sur les hommes et les femmes fertiles à Ibadan. Le modèle de l’étude qualitative comprenait l’application des discussions à groupe cible avec les membres de la communauté(7DGC, n=42), des interviews en profondeur avec les hommes stériles (n=7), les femmes stériles (n=8) et les professionnels(n=13). Ces résultats ont révélé que les hommes et les femmes stériles aussi bien que les membres de la communauté ont communément aperçu que les contraceptives et l’avortement sont des causes de la stérilité aussi bien que les facteurs surnaturels et de comportement. Les participants n’etaient pas bien au courant des mesures de la prévention de la stérilité. On recherchait le traitement pour la stérilité auprès d’un mélange des services biomédicaux, des services fondés sur la foi et des services traditionnels. Les femmes stériles donnent la priorité à l’impact psychologique de la stérilité tandis que les hommes stériles donnent la priorité à l’impact économique et ils ont indiqué avoir dépensé entre 55% et 100% de leur revenu à s’occuper de la stérilité. La stérilté à un grand impact social, psychologique et économique sur la vie des hommes et des femmes. Les efforts destinés à la réduction de son impact doivent donner la priorité à la sensibilisation aux causes, à la prévention et au traitement de la stérilité, fournir un appui psychologique et assurer un système d’orientation efficace pour la conduite du traitement de la stérilité (Afr J Reprod Health 2009; 13[3]:85-98). KEYWORDS: Infertility, Perceptions, Social impact, Psychological impact, Economic Impact, Nigeria Introduction The ability to bear children is very important in Nigerian society.1 However, surveys indicate that since 1990 the prevalence of infertility is increasing and currently affects more than 30% of Nigerian women. 2 Previous exposure to Sexually Transmitted Infections (STIs) and infections after unsafe abortions or childbirth are the main causes of infertility in this context.3,4,5,6 The risk of infertility is 15-25% after one episode of pelvic inflammatory disease and as high as 50-60% after the third episode. When antibiotic treatment is not available, the rates are even higher.7 To treat infertility, a wide range of treatment options are available from the traditional and biomedical service providers. Infertility is not high on the agenda of policy makers. As with other countries in Sub-Saharan Africa, the Nigerian reproductive health strategy does not seek to reduce the prevalence or impact of infertility but instead aims to reduce the high fertility rate.8,9,10,11 Research in Nigeria1,12,13,14 and South-Africa 15,16 has shown that women are suffering from the social and psychological implications of infertility. Little is known about the impact on infertile men and the treatment seeking behaviour of infertile men and women in Sub-Saharan Africa. There is very limited research on the economic implications of infertility in Nigeria but these are likely to be substantial given the context. Poverty is widespread in Nigeria; more than 50% of the population lives on less than 1 US$ per day.17 Since the Nigerian health sector reform in the 1980s, health services in the public sector are no longer provided for free. User fees are the most common payment strategy in the public as well as the private sector taking its toll on the rural and the poor population.18 The purpose of the study was to gain an in-depth understanding of the perceptions of infertility among different groups, their experiences as well as their attitudes towards infertile men and women. The objectives of the study were (1) to investigate the perception of infertility and its treatment among infertile men and women, community members, traditional and faith-based healers and health professionals1 in Ibadan; (2) to describe the psychological, social and economic challenges faced by infertile men and women in Ibadan; and (3) to identify strategic options for how the health care system can improve its support to infertile men and women in Ibadan. 1 The term ‘traditional and faith-based healers’ refers to all service providers who did not receive biomedical training. The term ‘health professionals’ refers to biomedically trained service providers. The research team did not imply to judge the different systems by using these terms. Methods The study was conducted in Ibadan city, the capital of Oyo State in the southwest of Nigeria. It has an estimated population of 2.4 million19 and is predominantly inhabited by the Yoruba ethnic group. The data collection took place from April to June 2008. Qualitative research methods were used because of their appropriateness in obtaining an in-depth understanding of different groups’ experiences, beliefs and perceptions.20 Study participants A purposive sampling frame was deployed21: respondents were deliberately selected on the basis of features or characteristics that will enable a detailed understanding of the topic. Participants included primary and secondary infertile men and women; community members; health professionals and traditional healers directly involved in infertility investigations and treatment. Participants were recruited from various parts of the city, with different socio-economic backgrounds. A distinction was made between urban, semi-urban and rural areas to understand different points of view between richer and poorer participants. To be aware of the treatment seeking behaviour throughout their reproductive period, infertile men and women aged 50 – 60 years were also included in the study. Community members were recruited if they had not experienced infertility themselves but some of the community members recalled relatives who were / are infertile during the discussions. Professionals indirectly involved in the health care provision for infertile men and women were also recruited including a sociologist, a representative of the National Health Insurance Scheme, a lawyer experienced with the child adoption procedures, a representative of a non-governmental organization for reproductive and family health and a representative of a motherless babies’ home. The participants were indirectly recruited by the research team. A staff member from the Community Health Department of the University College Hospital (UCH) in Ibadan got in touch with the matrons in different community health centres. The matrons contacted the home visitors who identified and recruited participants for the interviews in the semi-urban and rural areas. Participants from the urban areas were recruited by a gynaecologist at UCH. Data collection Before data collection started, ethical approval was obtained from the Research Ethics Committee of the Liverpool School of Tropical Medicine and the Institutional Review Committee of the University of Ibadan and University College Hospital in Ibadan. Written informed consent was obtained from all participants. FGDs were held with community members only as infertility is a very sensitive topic and infertile men and women might not have been comfortable to discuss their experiences in a group. In-depth interviews (IDIs) were held with infertile men and women, traditional and faith-based healers and professionals such as nurses, general practitioners and gynaecologists. Three infertile couples agreed to participate in the study, but the husband and wife were interviewed separately. Ten interviews were held in English, while the other participants preferred the Yoruba language. The researcher was assisted by two research assistants, who received training in qualitative research methods before the start of the interviews. The female research assistant asked the questions during the interviews, while the male research assistant took notes. The interviews were transcribed verbatim into English and analyzed by the researcher. Participatory Learning and Action (PLA) tools22 were used within individual interviews and FGDs, to enable further discussion and reflection. The participants were asked to rank the challenges faced by infertile men and women. To understand the economic impact of infertility, the participants were given 20 beads and asked to indicate how many beads were spent on infertility investigations and treatment. Table 1 summarizes the participant groups included in the study. To assure the quality of the study, data collection continued till saturation point (the point at which no new data was emerging)23 was reached. To further ensure trustworthiness, triangulation of methods and respondent type was undertaken and the preliminary results were discussed with people outside the research team. Data analysis The data analysis started simultaneously with the data collection and was an iterative and continuous process. The analysis followed the analytic hierarchy, from data management to descriptive and explanatory account, as discussed by Spencer.24 The tape recorded interviews were transcribed verbatim into English. After familiarization with the data, the research team identified a set of common themes that emerged from the data. MAXqda, a code and retriever software programme was used to attach codes to segments of the data. The research team discussed the different segments to identify patterns, commonalities and differences. During the second stage, the range of perceptions, views and experiences within an identified theme, were analyzed by the research team. Finally, links between experiences, behaviour, perspectives and characteristics of the participants were identified. Results The following section illustrates the major themes that emerged from the interviews. Causes of infertility The findings reveal 3 key categories of causes of infertility: medical, supernatural and behavioural factors (Table 2). Family planning, especially the use of oral contraceptives, was mentioned by many community members and infertile men and women as a cause of infertility. Condoms, IUDs and Depo Provera were not mentioned by participants. Abortion and the use of drugs were also frequently mentioned causes of infertility in women. The participants explained that abortions could lead to infertility because of damage to the womb, when the procedure is performed by a quack doctor or a woman goes to the chemist to buy drugs to terminate the pregnancy. STIs were not often mentioned as a cause of infertility by infertile men, women, community members or health workers. “Infertility can come as a result of what we had done or caused by ourselves, for example doing family planning. If anybody should do that, she is the one causing problems for herself. God has already designed the programme that we should continue to conceive and multiply all over the earth.” [FGD 5, rural men] Supernatural factors are also believed to cause infertility. A person could be punished by offended witches, wizards or elders. Infertility could also be caused by powers of darkness, called ‘Juju.’ Another reason is that a person might be destined not to have any children in the physical world or is cursed by other people or God Himself. Someone’s behaviour in the past or present is believed to be another reason for infertility. Sexual intercourse, outside of marriage which was construed as immoral, was mentioned by all participant groups as the most important behavioural factor for infertility. Prevention of infertility Measures that could be taken to prevent infertility were not well known by the participants. Many said that only God can prevent infertility in a couple. The participants that mentioned that prevention was possible pointed out that infertility can be prevented by educating children; abstinence from sex before marriage and being faithful during marriage; seeking treatment or ensuring the gods are appeased. Traditional healers reported they can make special soup for children to prevent infertility in the future. “A parent who has only one child may want to prevent infertility in the child when he or she is married. There is a special soup we prepare, as soon as the soup is eaten, if the person wants to have 20 children, nothing will stop it.” [IDI 13, rural traditional healer] Infertility treatment Most of the infertile men and women would seek treatment between one and three years after the wedding, although one participant waited for nine years after her wedding. They would advise other people in the same situation to seek treatment earlier than they sought treatment themselves. Most participants will advise someone that expects to be infertile to seek medical attention within one year after marriage. Where they advise such a person to go depends on their own experience as well as their religion. It is often the infertile woman who would go to a service provider as the infertility problem is perceived to be the woman’s. If anyone accompanies her, it is likely to be her husband, although both partners could also go to different service providers. A woman could visit a gynaecologist at a district hospital, while her husband visits a private clinic at the same time. Diagnosis and treatment for infertility in hospitals and clinics may include hysterosalpingography (HSG), semen fluid analysis and laparoscopy. Among community members and health professionals, there is no agreement whether infertile men and women should be advised to adopt a child. Community members are in agreement that child adoption is not a lasting solution as it might cause serious problems in the future. It is very difficult for the parents to explain why the child does not look like them and sooner or later, the relatives will find out that the child has been adopted. Health professionals are not likely to advise child adoption because it could add to the stress infertile men and women already experience by going through examinations and infertility treatment. Child adoption from state or private motherless babies’ homes will only be advised by health professionals after childbearing age when it is obvious that only adoption will give the couple a child to raise. The infertile men and women interviewed did not mention adoption as a solution to their infertility problem. Fostering – whereby – a couple raise a child born in the family network was mentioned by some as a potential solution, although it was stressed that the child would still ‘belong’ to its biological parents and not the foster parents. “Adopting a child may lead to problems in one’s life. There was a case of a couple who adopted a child and at midnight, the child will turn into a snake and go inside the cupboard and eat the soup, it nearly broke the relationship and the problem continued like that until they sought the face of the Lord before it was revealed to them and the child was caught.” [FGD 5, rural men] The husband taking another wife was frequently mentioned as a response to infertility. If there is a suspicion that the couple is infertile, community members would first advise the husband to take another wife. One participant mentioned that the woman’s family members will advice that she tries another man to confirm who the problem is between her and her husband. Social impact The social pressure to have children is very high. After the wedding, the wife is expected to show signs of pregnancy within one year. If she fails to conceive, she may be taunted by her in-laws, neighbours and relatives and called different names, such as male pawpaw, barren sister, empty basket, witch or walnut. Lack of support from family members, neighbours, relatives and friends was often mentioned by infertile men and women. Infertile women are verbally abused, mocked and jeered at. Advice is often given regarding where the infertile men and women should seek help, even when it is against their religious beliefs. Christians are not expected to visit a traditional healer but infertile Christian men and women can be advised to visit a traditional healer experienced in infertility treatment. If they are reluctant to visit these healers, the relatives will question the seriousness of the couple’s wish to conceive. “A childless home is not regarded as a home in Yorubaland. It is always believed that children make a home. So if a woman is finding it difficult to reproduce, she is looked at as a failure.” [FGD 6, rural women] Psychological impact The psychological disturbances faced by infertile men and women are often inextricably linked to the social impact. Infertile women worry about their situation; and reported being unhappy or are depressed. They report ‘bitterness of heart’ and could become suicidal because of their infertility problem. “Being human, I cannot but think and worry about my situation… this often makes me unhappy. Sometimes when I have a disagreement with my husband I will feel that if only I have children for him we will not be disagreeing like this often.” [IDI 4, semiurban infertile woman] Infertile men cope with infertility differently. They either accept the situation or try not to think about it. They often referred to the psychological problems their wives were facing. “At times my wife will refuse to eat, even if I talk to her, she might refuse to respond. She might even be crying. She will look sad and unpleasant. She might even be querying the God for creating her without an issue (child) of her own.” [IDI 5, semi-urban infertile man] Economic impact The cost for infertility investigations and treatment is different for each service provider. Faith-based healers are considered cheap. Traditional healers are considered more expensive than faithbased healers and equally expensive or more expensive than biomedical treatment. Traditional healers are reported to be expensive because of the collection of materials and the preparations of concoctions. Infertile men and women often visit more than one and a combination of different service providers during the woman’s childbearing age. During the interview, they were given 20 beads and asked to indicate how many beads they spent on infertility investigations and treatment so far. On average infertile men and women had spent 55% but it could be as high as 100% of their income depending on their treatment seeking behaviour and socio-economic background. The economic impact was bigger for the infertile men and women living in the semi-urban and rural areas than the ones living in the urban areas. “We have spent a lot of money but money is nothing compared with children. A man who is wealthy but has no child has no value in this world.” [IDI 6, semi-urban infertile woman] Table 3 shows some of the fees charged at biomedical facilities, to illustrate how much patients are charged for each consultation and investigation. The prices differ between providers and are generally higher in private facilities. Prioritizing of problems To understand which impact was perceived to have the biggest influence on the lives of infertile men and women, community members and infertile men and women were asked to rank the social, psychological and economic impact in order of importance. The community members expected that the social impact would be the most difficult for infertile men and women to deal with, followed by the psychological and lastly the economic impact of infertility. Community members debated whether the social or psychological impact was impacting infertile men and women most but agreed that the economic impact was least. The economic impact was also least important for the infertile women. They prioritized the psychological impact, followed by the social impact. The psychological impact was very important for most of the infertile women interviewed. For the infertile men, the economic impact was the most important problem, followed by the psychological and then the social impact of infertility (Table 4). “I think it is the psychological that is the most important. Money is meant to be spent. What is the use of the money anyway when there is no child to spend it on? It is the problem you face with the in-laws when she comes in to tell you, in a house that you managed to build with your husband, that since you are a man like my son, why don’t you allow him to bring in another woman that can give him a child? We spend money but no one is interested in that because they think the woman is the problem. Or is it the social problem when you sit in a society and there is no one to run to you to say mummy? So I think the psychological problem is the most important. I always have money in my pocket to spend.” [IDI 5, urban infertile woman] Discussion Despite surveys indicating that the prevalence of infertility is increasing in Nigeria2, it has received little attention from policy makers. The impact of infertility on infertile men and women is not well understood; and there are debates in the literature25 and the Nigerian context on whether efforts to reduce the impact of infertility should focus on prevention of infertility or the availability of infertility treatment. Previous studies on the impact of infertility did not include infertile men and the economic impact of infertility has not been studied before. This study has included infertile men and women as well as community members and health professionals to bring out the voices and experiences of different groups. The study revealed three key themes which will be discussed in turn; the misperceptions of causes of infertility; the different impact of infertility on women and men; and the implications for health seeking behaviour. The findings revealed misperceptions on the causes of infertility amongst all participant groups. Abortion and the use of contraceptives were frequently mentioned causes of infertility. Abortion is currently the main method to resolve an unwanted pregnancy in Nigeria, especially amongst unmarried women. 26 The fear of infertility could partly explain the low contraceptive usage in Nigeria. A study among Nigerian students showed that 41% of the students believed that oral contraception could cause infertility.27 Results of this and other studies do raise the need to emphasize that contraceptives can protect against infertility and are not causing it.2 If appropriate family planning techniques were used, women would not need to resort to abortion, which can lead to STIs and infertility. STIs were not mentioned by most of the participants as a cause of infertility. There is a need to make communities aware that STIs can lead to infertility, without inadvertently intensifying the stigma already associated with infertility. It is important to include the youth in these awareness raising programs, especially in southwest Nigeria.28 Among the Yoruba, it is estimated that 55% of women have premarital sexual intercourse, which is one of the highest levels in the country.29 A reduction of the number of unsafe abortions and STIs will reduce the prevalence of infertility but infertility cannot be eliminated. Treatment options for infertility will continue to be necessary. Health education strategies need to focus on raising awareness on prevention and causes of infertility, specifically targeting the youth and potential contraceptive users. The impact of infertility is different for infertile men and women. Infertility is stigmatized. Women lack support from the extended family, while the men suffer because of the impact of infertility on themselves and psychological impact on their wives. The economic impact of infertility is prioritized by infertile men. They are expected to pay for the investigations and treatment and use a significant part of their income on it. Infertile women prioritized the psychological impact. The psychological reactions were often due to the intense social pressure to become pregnant and comments from other family members and relatives. It is thus important to ensure that psychological support services are available to infertile women. It was surprising that community members expected the social impact to be worst for infertile men and women. They may be more concerned about the family name being stigmatized. In Yorubaland, the family name is held in very high esteem. And families without children are isolated. Although they realized that the social impact is very important, community members did not identify measures to support infertile men and women. In the literature it is suggested that the type of service provider chosen depends on the perceived cause of infertility.30 This might be true for the first contact but this study reveals complex pathways: infertile men and women are consulting more than one type of service provider sometime sequentially and sometimes simultaneously. If one type of service provider is unsuccessful, infertile men and women will go to another, even if their religious leaders do not allow certain service providers to be visited. Another reason is that due to pressure from family members and relatives, infertile men and women need to show that they are serious about their desire to conceive and need to prove they have done everything they could. The tendency for infertile men and women to visit different service providers makes the economic impact very high. Traditional healers were considered as or more expensive than the biomedical service providers, which contradicts previous findings.31,32,33 The results of this study indicate that the economic impact of infertility is considerable. It is important that infertile men and women visit the hospital for investigations and treatment before they spend a lot of money on traditional, and at times harmful, practices or expensive private providers. Health care providers at primary and secondary levels need to be informed about the referral pathways for infertility and be aware of the services that can be offered at the different hospitals. Infertility deserves more attention than it has received in the previous years.9,11 It should be brought back on the agenda of policy makers and be integrated into the sexual and reproductive health strategy in countries in Sub-Saharan Africa. A joined up approach is pragmatic and appropriate given limited resources. Swift treatment for STIs is important to reduce infertility as well as vulnerability to HIV. People need to be aware how infertility can be prevented and need to know the factors that are and are not causing infertility. Tackling the stigma of infertility is critical and lessons learnt in other areas such as HIV could be used to develop an approach to reduce stigma and support infertile men and women. Psychological support services should be made available to infertile women, involving referral hospitals and religious leaders. In the short term the available resources should not be used to subsidize infertility treatment but should focus on the prevention of infertility and psychological support. Acknowledgements The Kenneth Newel Trust Award supported the writing of this manuscript. References 1 Umezulike, A. and E. Efetie, The psychological trauma of infertility in Nigeria. International Journal of Gynecology & Obstetrics, 2004. 84: p. 178-180. 2 Rutstein, S., DHS Comparative Reports No 9 -Infecundity, Infertility, and Childlessness in Developing Countries. 2004. 3 Larsen, U., Trends in infertility in Cameroon and Nigeria. International Family Planning Perspectives, 1995. 21: p. 138-142. 4 Omo-Aghoja, L., et al., Association of Chlamydia trachomatis serology with tubal infertility in Nigerian women. Journal of Obstetrics and Gynaecology, 2007. 33(5): p. 688-695 5 Okonofua, F., Infertility and women's reproductive health in Africa. African Journal of Reproductive Health, 1999. 3(1): p. 7-12. 6 Ericksen, K. and T. Brunette, Patterns and predictors of infertility among African women: a cross-national survey of twenty seven nations. Soc. Sci. Med., 1996. 42(2): p. 209-220. 7 World Health Organization, Sexually transmitted and other reproductive tract infections. 2005, World Health Organization: Geneva. p. 182-184. 8 National Population Commission of Nigeria. The Nigerian Population Policy 2006 [cited 26-06-2008]; Available from: http://www.population.gov.ng/policy.htm. 9 Butler, P., Assisted reproduction in developing countries -facing up the issues, in Progress in reproductive health research. World Health Organization, Geneva, 2003 10 Sundby, J. and A. Jacobus, Health and traditional care for infertility in the Gambia and Zimbabwe, in Women and Infertility in sub-Saharan Africa, J. Boerma and Z. Mgalla, Editors. KIT Publishers: Amsterdam. 2001 p. 257-268. 11 van Balen, F., Interpreting infertility: social science research on childlessness in a global perspective. African Journal of Reproductive Health, 2000. 4(1): p. 120-122. 12 Okonofua, F., et al., The social meaning of infertility in southwest Nigeria. Health Transition Review, 1997. 7: p. 205-220. 13 Aghanwa, H.S., F.O. Dare, and S.O. Ogunniyi, Sociodemographic factors in mental disorders associated with infertility in Nigeria. Journal of Psychosomatic Research, 1999. 46(2): p. 117-123. 14 Orji, E., O. Kuti, and O. Fasubaa, Impact of infertility on marital life in Nigeria. International Journal of Gynecology & Obstetrics, 2002. 79: p. 61-62. 15 Dyer, S.J., et al., Psychological distress among women suffering from couple infertility in South Africa: a quantitative assessment. Human Reproduction, 2005. 20(7): p. 19381943. 16 Dyer, S., et al., `You are a man because you have children': experiences, reproductive health knowledge and treatment-seeking behaviour among men suffering from couple infertility in South Africa. Human Reproduction, 2004. 19(4): p. 960-967. 17 World Bank. Nigeria Country Brief. 2007 [cited 02-11-2007; Available from: http://web.worldbank.org/WBSITE/EXTERN AL/COUNTRIES/AFRICAEXT/NIGERIAE XTN/0,,menuPK:368906~pagePK:141132~pi PK:141107~theSitePK:368896,00.html. 18 Onwujekwe, O. and B. Uzochukwu, Socioeconomic and geographic differentials in cost and payment strategies for primary healthcare services in southeast Nigeria. Health Policy, 2005. 71: p. 383-397. 19 Mabogunje, A., Nigeria: physical and social geography, in Europe regional surveys of the world: Africa south of the Sahara. 2007, Routledge 2007. p. 896. 20 Malterud, K., The art and science of clinical knowledge: evidence beyond measures and numbers. The Lancet, 2001. 358: p. 397-399. 21 Ritchie J, Lewis J and Elam G. Chapter 4 ‘Designing and selecting samples’ in Eds. J. Ritchie and J. Lewis Qualitative Research Practice: A guide for Social Science Students and Researchers: SAGE, 2003. 22 Chambers, R. (1992). Actual or potential uses of RRA/PRA methods in health and nutrition. [Special Issue on Applications for Health]. RRA Notes, 16. 23 Mays, N. and Pope, C. ‘Assessing quality in qualitative research’, British Medical Journal; 2000; 320:50-52 24 Spencer, L., J. Richie, and O. O' Connor, Analysis: practices, principles and processes, in Qualitative research practice: a guide for social science students and researchers, J. Richie and J. Lewis (eds). Sage publications: London, 2003 p. 212-216. 25 Butler, P., Assisted reproduction in developing countries -facing up the issues, in Progress in reproductive health research. World Health Organization, Geneva, 2003. 26 Okonofua, F., Unwanted pregnancy, unsafe abortion and the law in Nigeria. Trop. J. Obstet. Gynaecol., 2002. 19(Suppl 1) 27 Adinma, J. and A. Okeke, The pill: perceptions and usage among Nigerian students. Advances in Contraception, 1993 9: p. 341-349. 28 Ikechebulu, J., et al., High prevalence of male infertility in southeastern Nigeria. Journal of Obstetrics and Gynaecology, 2003. 23(6): p. 657-659. 29 Garenne, M. and J. Zwang, Premarital Fertility and Ethnicity in Africa. DHS Comparative Reports No. 13. 2006, Macro International Inc.: Calverton, Maryland, USA. 30 Pearce, T., Hated by society: perceptions of female infertility among the Yoruba, in Thirty-seventh annual meeting of the African studies association. Toronto, Canada. 1994 p. 1-21. 31 Ayonrinde, F., Socio-economic determinants of health facility usage in Oyo State. The Nigerian Journal of Economic and Social Studies, 2001. 43(3): p. 497-514. 32 Ademuwagun, Z., The relevance of Yoruba medicine men in public practice in Nigeria. Public Health Reports, 1969. 84(12): p. 10851091. 33 Barnett, B., Helping Men Understand Infertility. Network, 2003(2):19. The following images related to this document are available:Photo images[rh09037t4.jpg] [rh09037t2.jpg] [rh09037t3.jpg] [rh09037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}