 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
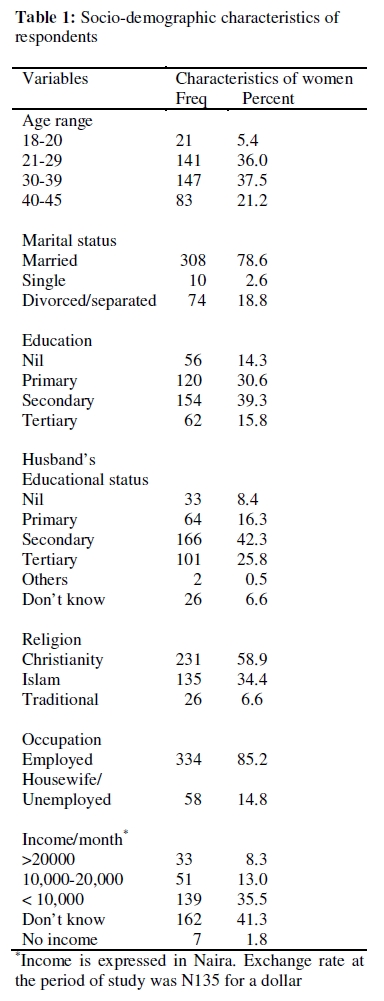
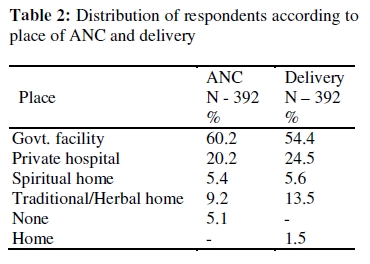
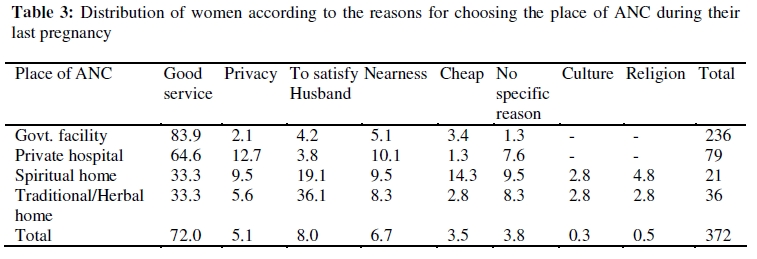
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 111-122 ORIGINAL RESEARCH ARTICLE Utilization of Antenatal care and Delivery services in Sagamu, South Western Nigeria Utilisation des services prénatals et d’accouchements à Sagamu, au sud-ouest du Nigéria C A Iyaniwura1 and Q Yussuf2 1Department of Community Health and Primary Health Care, Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State, Nigeria; For correspondence: Dr (Mrs) C A Iyaniwura, Reproductive and Family Health Unit, Department of Community Health and Primary Health Care, Olabisi Onabanjo University Teaching Hospital Sagamu, Ogun State, Nigeria. Email: christywura@yahoo.com ABSTRACT A survey of 392 women who had carried at least one pregnancy to term in Sagamu, South-Western Nigeria was conducted to determine the pattern of use of maternity services and assess factors that may influence the observed pattern. Majority of the women received antenatal care (84.6%) during their last pregnancy. Four-fifth of those who received ANC first attended the clinic during the second trimester (79.6%). The places of delivery were government facilities (54.8%), private hospital (24.5%), traditional birth attendants (13.5%) and spiritual healing homes (5.6%). Higher educational status and higher level of income positively affected the pattern of use of these services (p<0.05). Perceived quality of service was the most important factor which influenced the choice of facility for obstetric care. A considerable proportion of those who used traditional birth attendants (36.1%) used it to please their husbands. Our findings suggest that improving the socioeconomic status of men and women in the community is a key factor to improving utilization of maternity care services (Afr J Reprod Health 2009; 13[3]:111-122). RĖSUMĖ Une enquête sur 392 femmes qui ont eu au moins un accouchement à terme à Sagamu au sud-ouest du Nigéria a été menée. Ceci pour déterminer la tendance de l’utilisation des services de gynécologieobstétrique et pour évaluer les tendances observées. La plupart des femmes ont obtenu des soins prénatals (84,6%) pendant leur grossesse. 4/5 de celles qui ont obtenu les soins prénatals se sont présentées à la Clinique pour la première fois au cours du second trimestre (79,6%). Les lieux d’accouchement étaient des établissements gouvernementaux (54,8%), les hôpitaux privés (24,5%), chez les sages-femmes traditionnelles (13,5%) et dans les maisons de guérison spirituelle (5,6%). L’utilisation de ces services est influencée positivement par le niveau supérieur de l’instruction acquise et un niveau élevé de revenu (p<0,05). La qualité perçue du service était le facteur le plus important qui a influencé le choix de l’établissement pour les soins obstétriques. Une proportion considérable de celles qui se sont servies des sages-femmes traditionnelles (36,1%) le faisant pour faire plaisir à leurs maris. Notre étude a montré que si la situation socio-économique des hommes et des femmes dans la communauté est améliorée, cela sera un facteur clé pour l’utilisation des services des soins gynécologie-obstétrique (Afr J Reprod Health 2009; 13[3]:111-122). KEYWORDS: Utilization, Antenatal care, Delivery services, Sagamu, South Western Nigeria Introduction Many women lose their lives in the process of procreation. Every year, more than half a million women die from pregnancy related causes and majority of these deaths occur in sub-Saharan Africa1. Every minute at least one woman dies from pregnancy and childbirth. In Nigeria, an average of 704 women die out of every 100,000 women who bring forth a live birth. Maternal Mortality Ratio (MMR) ranges from 166 per 100,000 in the South West to 1,549 per 100,000 live births in the North East2. Fortunately, most of these deaths are preventable. High quality accessible health care has made maternal deaths a rare event in developed countries. While the risk of maternal death for a pregnant woman in developing countries is 1 in every 48 deliveries, the risk for a pregnant North American woman is only 1 in 3,2003. Adequate antenatal care (ANC) and skilled obstetric assistance during delivery are important strategies that significantly reduce maternal mortality and morbidity. ANC provides avenue to provide pregnant women with information, treat existing social and medical conditions and screen for risk factors. However it is not enough to receive ANC, since majority of the fatal complications occur during or shortly after delivery4. It is therefore important that pregnant women have skilled obstetric attendance during delivery. While an estimate of 97% of the pregnant women in developed countries receive ANC and 99% use skilled obstetric service at delivery, 65% and 53% of women in developing countries use ANC and skilled obstetric care respectively4. In Nigeria, National HIV/AIDS and Reproductive Health Survey (2003) showed that 62% of women who gave birth within the past year before the survey received ANC while 34% had skilled attendance during delivery2. At the Safe Motherhood Initiative (SMI) Conference Kenya in 1987 the participating countries agreed to decrease maternal mortality by 50% by the year 2000. Despite all the initiatives to reduce maternal deaths in Nigeria, MMR remains persistently high. Similar to data from other parts of Nigeria5, in Olabisi Onabanjo Teaching Hospital, Sagamu the maternal mortality ratio in the past two decades have remained persistently high. A decade review of maternal mortality in the teaching hospital between 1988 and 1997 revealed an average MMR of 1936.1 per 100,0006. Between January 2002 and December 2004, Oladapo et al reported a MMR of 2931.4 per 100,0007. Majority of the deaths occur among unbooked patients6-8. Some of these authors expressed that the statistic may be worse in the community6. Poor utilization of quality reproductive health service continues to contribute to maternal morbidity and mortality in developing countries2,9 . Understanding the preferences of the people and the various factors that influence their preferences will help to put in strategies that will improve utilization of skilled obstetric services and thereby reduce unnecessary loss of lives. This study therefore assessed the awareness of ANC and delivery services, the preferences and the factors underlying these preferences among child-bearing women in a sub-urban population in South-west Nigeria. Methods This is a descriptive cross sectional study that was conducted in Sagamu town between the months of September and October 2005. Sagamu is a suburban town and a local government headquarters in South Western Nigeria. Sagamu is a Yoruba town though people from other tribes also live there. The major occupations of the people are farming and trading. Private and public health institutions as well as local traditional and spiritual healers provide health care services for the people. Health institutions are well distributed in different parts of the town. The public health institutions included a teaching hospital (Olabisi Onabanjo University Teaching Hospital) and three (3) primary health care centres. At the public institutions, while ANC services are delivered on specific days of the week, labour cases are attended to at any time of the day. Women of childbearing age who had at least one pregnancy carried to term in the past 5 years were the study population. The questionnaire was pretested among 20 women of childbearing age in a neighbouring community and corrections were subsequently effected. The sample size for the study population was determined using the formula, n= z2pq/d2, where z is 1.96 at 95% confidence interval, prevalence (p) of 65%2 and d, the tolerable standard error of 0.05. The calculated minimum sample size was 346, a non response rate of 10% was added to the minimum sample size and the figure and rounded up to 390. Sagamu town is made up of 11 wards. Using the ballot paper method, three (3) wards were randomly selected out of the 11 wards. Five streets were randomly chosen from each ward, which gave a total of 15 streets. Starting from any house on the selected streets (n=15) and moving from one house to another, questionnaires were administered to 26 eligible respondents. In the houses where there were many households with eligible women, a maximum of two eligible women were chosen. Interviewers were five female Community Health Extension Workers who were trained to collect the data. Verbal consent was first obtained from the respondents before proceeding on the interview. Structured questionnaire was used to gather information about the respondent’s awareness of ANC and delivery facilities in their community, the facility used during their last pregnancy and the reason for their choice. The questionnaires were analysed using Statistical Package for Social Sciences version 10. The results are presented as frequency tables and percentages. The chi-square statistic was used to evaluate association between certain variables and use of ANC and delivery services. P value less than 0.05 was accepted as being statistically significant. Results A total of 392 women were involved in the study. Table 1 shows that the age range of the women was 18-45 years, majority of them were between 21-39years of age (73.5%). Three hundred and eight (78.8%) were married, while 2.3% were single. Of the 351 who indicated their type of marriage, almost two-thirds (61.8%) were in monogamous union. The majority (58.9%) were Christians, 34.4% were Muslims and 6.6% practiced the traditional religion. More than four fifths were Yorubas, 9.9% were Ibos while 7.1% were Hausas. Fifty six (14.3%) had no formal education, 55.1% had more than primary school education. Fifty eight (14.8%) were not gainfully employed. Because many of them were petty traders (63.5%) who lived off daily gains it was not easy for some to estimate their monthly income (42.1%). Almost all (96.7%) reported that their husbands were employed but majority did not know their husbands monthly income (72.3%). Three hundred and thirty (84.2%) had their first pregnancy between the ages of 20-29 years, 12% had the first pregnancy in their teens. Almost all the women (97.2%) indicated that antenatal care is important for pregnant women; only 0.8% said it was not necessary while 1.8% were not sure. Three hundred and forty one (87%) were aware of antenatal care facilities in the community. The known facilities were government facilities (59.7%), private hospitals (16.3%), traditional/ herbal homes (9.9%) and spiritual healing homes (3.1%). The reported sources of information about place of ANC were friends (30.1%), relations (27.0%), health worker (19.1%) and others (12.2%). Utilization of ANC during last pregnancy Three hundred and seventy two (84.6%) received ANC during their last pregnancy. Most of the women who received ANC used a government facility (63.4%), 21.2% attended a private clinic. Almost one in every ten (9.7%) used traditional herbal home (Table 2). Table 3 summarizes the reasons for their choice of a place for ANC. The highest consideration for their choice of facility was that the service was good (71.5%). While 8% used the facility of their husband’s choice, 6.9% chose the facility because of proximity to their house. Women who used government facilities were most likely to indicate that the service was good (83.9%). Considerations for choosing private clinics were good service (64.6%), privacy (12.7%) and nearness (10.1%). Irrespective of their primary consideration, 94.3% still sought their husband’s permission before using a facility. Compared to users of other facilities, more women who used traditional birth attendant (TBA) facilities (36.1%) and spiritual homes (19.1%) indicated that they did so to please their husbands. During their last pregnancy, majority of those who received ANC first attended the clinic during the second trimester. Almost half (49.6%) attended at 3-4 months of gestation, 30% at 5-6months, 8.2% at 7-6months. Few booked at the extremes of gestation, 6.1% at 9months and 5.6% at 1-2 months. Most women (46.4%) visited the clinic more than 4 times, 14.8% made three to four visits, 3.6% made one to two visits while 30.6% could not remember the number of ANC attendances. Sixty eight percent (68%) received two doses of tetanus toxoid, 9% received one while 13% received none. A higher proportion of the women who were aged less than 20 years (19%) did not use ANC facilities compared to women in the older age groups (<10%) (p < 0.05). The proportion of the women that had ANC increased with respondent’s educational status (p<0.0001) and the husband’s educational level (p< 0.005). The traditional worshippers were less likely to have received ANC compared to Christians and Muslims (p<0.010). All the women who earned more than N10,000 ($74) per month received ANC while 6.5% of those who earned less than N10,000 ($74) per month did not receive any ANC (Table 4). Majority of the women did not know their husband’s income. Compared to those who were employed, women who indicated that their husband were unemployed were less likely to use ANC (p< 0.05). Fifty percent (50%) of those who reported that their husbands were unemployed did not use ANC service. Education and income affected pattern of use of ANC by the respondents. Uneducated women had fewer ANC attendances compared to the well educated women. Thirty nine percent (38.7%) of the women who had no formal education had four or less antenatal attendances compared to (18.1%) of the women with tertiary education. Women who earned less than N20,000 ($148) per month also had fewer ANC attendances compared to women who earned more than that. Only 3.9% of the women who earned more than N20,000 ($148) per month had four or fewer ANC attendances compared to 23.5% of those who earned less than N10,000 ($74). Place of delivery Of all the women, only six (1.5%) delivered at home. The preferred places of delivery were government facilities (54.8%), private hospital (24.5%) and traditional/herbal homes (13.5%). Few women delivered at spiritual healing homes (5.6%). A lower proportion of women who received ANC at government facilities eventually delivered there while the proportion of the women who delivered at private clinics and TBA increased compared to ANC attendance (Table 2). Women who had none or primary education, traditional worshippers and those who had low income were more likely to use traditional birth attendants/herbal (TBA) home for delivery compared to other women (Table 5). Of the 177 who did not deliver their babies in government facilities, 31.6% gave no reason, 29.4% complained of the long waiting time, bad attitude of staff (11.3%), non-availability of government facility in their community (10.2%) and transportation problem (8.0%). Discussion Antenatal care and skilled obstetric care are important strategies for improving maternal and newborn health but many women in developing countries continue to go through pregnancy and delivery without using these services. In this study, there was a high level of awareness of the need for special care for women during pregnancy and majority of the women knew where they could receive ANC in their community. This can be attributed to the high proportion of women who had formal education and that the study was located in a semiurban community where there was easy access to the mass media. Majority of the women received ANC, booked during the second trimester and had more than 4 ANC visits. However many of the women who received ANC did not attend antenatal clinic until the second or third trimester by which time it may be too late to benefit maximally from some of the services delivered at the clinic. The reported widespread use of ANC (84.6%) in this study supports the findings of the National HIV/AIDS Reproductive Health Survey in 2003 where 89.4% of the women from South Western Nigeria reported that they received ANC during their last pregnancy2. This is much higher than the rate of use reported in other parts of Nigeria such as Northern Nigeria (10), Eastern Nigeria11 and rural South-South Nigeria12 . In a study of 107 women in rural Kano, Northern Nigeria, 88% did not attend ANC and 96.3% had delivered or planned to deliver at home10 . The disparity in use of maternity services in various parts of Nigeria may partly account for the vast difference in maternal mortality in the different regions, varying from 166/100,000 in South-West to over 1500/100,000 in Northern Nigeria2. Despite the relatively high rate of use of maternity services in this study, hospital statistics show that some women in this area still die from complications of pregnancy and child bearing7,8 . Use of ANC maternity services in this study is relatively higher than in many other parts of Nigeria but it is much lower than what is reported from other countries or regions such as East Asia or North America where all or almost all pregnant women received ANC and deliver in health institutions13. In this study, one in five women (20%) did not use ANC service at all or they used non-health institutions such as TBA or spiritual homes. The rate of non-use of maternity services may also be much higher in the rural areas compared to suburban and urban areas. Bawa et al in a study of a rural area in South west Nigeria found that although many women attended at least one ANC, most of them refused to deliver in the hospital14 . It is important that all pregnant women access quality ANC and have skilled attendant at delivery. Perceived quality of service is a major factor that influence people’s decision to use health care facility 16,17 . Though many of those who used the services expressed that the service was good, the main reasons given for nonutilization of government services for delivery by those who used other facilities were linked to quality of care. Similarly, in a community based survey in Eastern Nigeria, Uzochukwu et al found that 94.3% and 95.8% of the women were satisfied with the ANC and delivery services at the health centres. However, they also complained of long waiting queues, provider behaviour and lack of doctors as factors which militate against use 15 . Government facilities are usually associated with long waiting time and poor staff attitude which discourages many women from using these facilities14, 15 . In Enugu, South-Eastern Nigeria, promptness of care and friendliness of staff featured prominently as factors which encourage maternity utilization16 . Effort should be made to reduce waiting time at the hospitals, train health workers to be empathetic, improve the facilities at the health clinics and make the system as patient responsive as much as possible. These improvements may reduce the problem of ‘empty bed syndrome” in Nigerian public hospitals. A lower proportion of the women who received ANC at the government facility eventually delivered there while more women delivered at private clinics and TBA centres compared to those who received ANC at these facilities. This may be due to easier accessibility of these facilities. The increased proportion of deliveries at TBA home may also be associated with the prevalent supernatural concept of diseases in many African communities. Twenty nine percent (29%) of ANC attendees in Equitoria Guinea expressed that TBAs were better than orthodox practitioners in some respects because TBAs possess spiritual powers and can intervene in certain situations where medical interventions cannot help17 . Among professionals, opinions differ about the role of TBAs in maternity care. While some insist that in the interest of maternal health, empowering TBA through training and retraining is the best option because community members will continue to patronise them, others express that TBAs have little role in obstetric care 18 . Similarly, spiritual healing centres are also well patronised by women in many parts of Nigeria16 and therefore should receive due attention by policy makers and programme planners who seek to reduce maternal and neonatal mortality. Though majority of the women received ANC and sought assistance during delivery, some women were more likely to receive maternity care or use non-health institutions compared to others. Our result is consistent with findings from other studies that formal education has a positive effect on the use of ANC services16, 17 . Educated women in this study were more likely to have received ANC during pregnancy, had more frequent visits and used health facilities for delivery. The effect was more significant among women with at least secondary school education. The effect of education may be associated with better exposure to information and higher income. A well-educated woman may have a good job and earn more money, which improves economic access and reinforces the effect of adequate information. Though very few women indicated cost consideration as the reason for their choice of ANC facility, our findings suggest that high income is associated with good obstetric behaviour. All the women who earned more than N20, 000 ($148) per month received ANC, had more frequent antenatal visits, were more likely to use orthodox facilities for delivery and none of them delivered at home. However this amount is almost thrice the official minimum wage of N7,500 ($55.6) in the state and few women do earn that much. It is interesting to note that the low-income women were more likely to use private clinics compared to women with higher income. This may be because low cadre workers may have less control over their time at work and therefore have to seek ANC outside the normal clinic hours. Due to the long waiting time at government institutions, petty traders may consider the opportunity cost of leaving their trade for long hours. Cost of care varies widely at private facilities; low cadre workers may find low cost, small scale maternity homes more affordable. Mode of payment may also be more flexible than the public sector and therefore more convenient for lowincome workers. It is therefore important that quality of care in private maternity homes should be well monitored. The influence of education and income suggests that with adequate education and improvement of the economic status of women in this community, near universal use of orthodox maternity services may be achieved. Across age groups, majority of the women used ANC services, however young women who were 20years of age or younger were less likely to use ANC facilities than older women. Although the few number of women in the youngest age group make it a bit difficult to draw a firm conclusion, similar pattern of lower utilization of ANC and delivery services among young mothers aged less than 19years have been described in many communities13 . A review of the use of ANC services by women in many developing countries between 1990 and 2001 showed that the youngest and oldest age groups were slightly less likely to use ANC services19 . Young women may be unmarried and may lack social support. They may be unable or unwilling to use maternity health services depending on the circumstances surrounding their pregnancy. It is unfortunate that women who appear to be at higher risk such as young, uneducated and poor women are less likely to access the appropriate services. Religion was also found to influence the choice of place of delivery by the women. The traditional worshippers were more likely to deliver with traditional birth attendants (TBAs). A similar relationship was found between religion and place of delivery among women in Eastern Nigeria 16. This relationship can be partly explained by the fact that those who are traditional worshippers may be less educated than Christians and the less educated are more likely to use nonhealth institutions. However, the effect of religion has been found to be significant even after education is controlled for 21. Onah et al further suggested that the quest of non-Christians for privacy and the fact that most of them are unskilled workers who may not be able to afford the cost of care may make them seek care at non-health care institutions11. Data from this study has further emphasised the need for male involvement in women reproductive health issues. Almost all the married women usually seek spousal approval of their choice of ANC and delivery facilities. Majority of the women who used TBA facility indicated that it was to satisfy their husband. Therefore in patriarchal societies like Nigeria, efforts to decrease maternal deaths should increasingly target men with necessary information about appropriate obstetric services. This is quite different from the situation in Kenya where most women made independent decision to attend ANC 21. Conclusion The women in this study are aware of the need for antenatal care and assistance during labour. Most use orthodox health facilities for ANC and delivery services but a considerable proportion still use non-medical institutions or do not use at all. The major factors that deter women from using government facilities for delivery include long waiting time and perceived poor attitude of the staff. Effort should therefore be made to improve the quality of services at the health facilities, minimise waiting time and train health care providers to communicate better with patients. Community education should also emphasise the need to book early for ANC so that women could maximise the benefits from the services. The World Health Organization recommendation of minimum of four visits should be encouraged (especially for eligible women of low socioeconomic status) so that their few visits can be appropriately timed and maximised. Universal education at least to secondary school level, improvement of the economic status of women and targeting men with information will significantly improve utilization of obstetric services with resultant reduction in maternal deaths in this community. References
The following images related to this document are available:Photo images[rh09039t2.jpg] [rh09039t3.jpg] [rh09039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}