 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
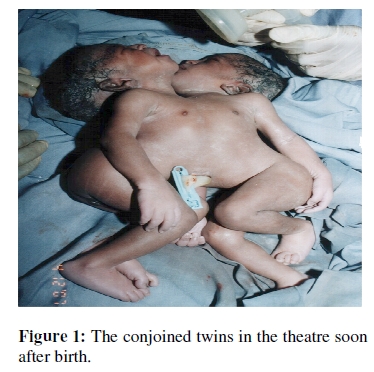
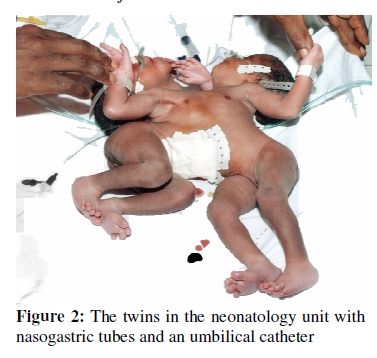
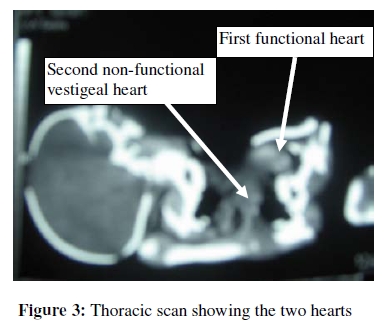
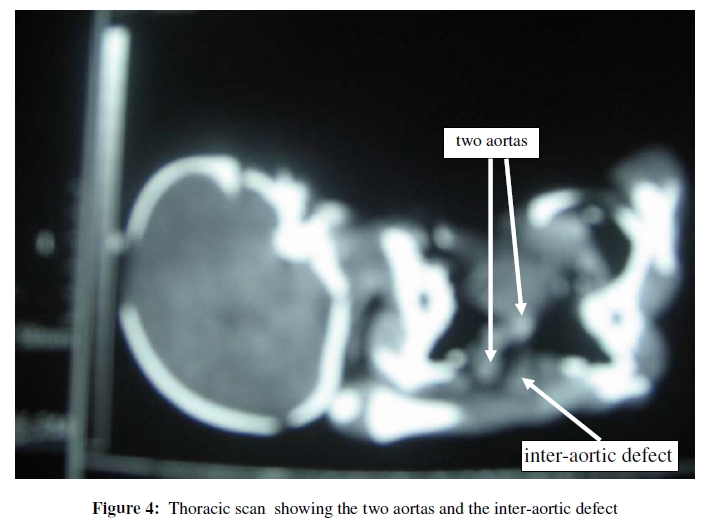
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 127-135 CASE REPORT Conjoined Twins in Cameroon: Issues Inherent in Diagnosis and Management in the African Context Les jumeaux siamois au Cameroun : Problèmes qui se rattachent au diagnostic et à la prise en charge dans le contexte africain. Andreas Chiabi 1, Denis Nkemayim 2, Pierre-Fernand Tchokoteu 1, Emilienne G. Guegang 3, Nkele Ndeki N. 2, Jacqueline Z. Minkande 4, Joseph Gonsu 3 and Anderson S.Doh 2 1 Pediatric Unit, Yaounde Gynaeco-Obstetric and Pediatric Hospital, Cameroon; For correspondence: Dr. Andreas Chiabi, Yaounde Gynaeco-Obstetric and Pediatric Hospital, Cameroon. P.O. Box 4362, Yaounde, Cameroon. Email: andy_chiabi@yahoo.co.uk ABSTRACT Conjoined twins represent one of the rarest forms of congenital abnormalities. We present a case of conjoined twins delivered at born in the Yaounde Gynaeco-Obstetric and Pediatric Hospital in Cameroon. They were joined at the chest and abdomen, and had one functional heart. The outcome was fatal on the seventh day of life, despite appropriate reanimation measures. This case highlights the difficulties inherent in the diagnosis and management of conjoined twins in low resource settings (Afr J Reprod Health 2009; 13[3]:127-135). RĖSUMĖ Les jumeaux siamois représentent une des très rares malformations congénitales. Nous présentons un cas des jumeaux siamois nés à l’hôpital Gynéco-Obstétrique et Pédiatrique de Yaoundé au Cameroun. Leur fusion se situait au niveau du thorax et de l’abdomen et ils avaient un cœur fonctionnel, l’autre étant resté vestigeale. L’issue a été fatale au septième jour de vie, malgré les mesures d’animation appropriées qui ont été mises en œuvre. Ce cas illustre les difficultes liées au diagnostic et à la prise en charge des jumeaux siamois dans les pays en voie de développement. (Afr J Reprod Health 2009; 13[3]:127-135). KEYWORDS: Conjoined twins, Prenatal diagnosis, Management, Cameroon. Introduction Conjoined or “Siamese” twins represent one of the rarest forms of congenital anomalies with an incidence of 1:200,000 live births 1, 2. The incidence in West Africa is not precisely known 3. The term “conjoined (Siamese) twins” is usually applied to twins who are united bodily but possessed of two separate personalities. It has therefore been used to include a wide variety of twins monstrously joined, and has included those who have shared various combinations of the trunk and limbs 4. Descriptions of conjoined twins date back to the ancient Egyptians but the first well documented case was the Bideen Maids, born in 1100 in Kent, England, and called Mary and Eliza Chulkhurst. They were joined at the hips and shoulders and lived together until 34 years. Conjoined twins have been viewed with fascination since antiquity. Interest has ranged from suspicion and fear of the birth being an omen of impending disaster to exhibitionism and more recently as a subject of intense media interest 5. Surgical management requires an experienced team of surgeons, anaesthetists and intensivists 1. This can be difficult in developing countries especially Africa where diagnosis is often late due to late prenatal consultations, lack of adequately trained personnel and appropriate infrastructures for surgery. We report a case of conjoined twins born in the Yaounde Gynaeco-Obstetric and Pediatric Hospital, whose outcome was fatal. The purpose of this report is to illustrate difficulties encountered in the diagnosis and management in a lowresource setting. Case Report Twin female conjoined new-borns were admitted in the neonatology unit of the Yaounde Gynaeco-Obstetric and Pediatric Hospital on 4/12/2007 following a caesarean section, at 37 weeks of pregnancy. The mother was 29 years old and teacher by profession and the father 35, and a computer engineer. The mother was G1 P000, irregularly followed up for her pregnancy in a district hospital. No particular illnesses were noted during the pregnancy. The first obstetrical ultrasound was done on the 19/11/2007 at 37 weeks and showed a twin pregnancy with fusion on the chest and abdomen, unique heart, umbilical cord and placenta and abundant amniotic fluid. The estimated gestational age from ultrasound was 33 weeks. Following these results, the patient was referred to our hospital where another ultrasound done three days later confirmed the conjoined foetuses with two fused hearts (one residual and non functional), interaortic defect and gestational age estimated at 35 weeks. A caesarean section was then done on the 4/12/2007. The uterus was opened through a vertical incision to facilitate extraction and the presentation of both twins was breech, and there was only one placenta. Post operative follow-up was uneventful. At birth, the Apgar score at the 1st and 5th minute for the first and second twins were 7/10, 9/10 and 3/10, 7/10 respectively. Both weighed 3.830 kg with no other visible morphologic abnormalities (Figure 1). Neurological examination showed axial hypotony of both babies with weak primitive reflexes. The babies were then transferred to the neonatology unit. Oxygen was administered (2 litres/minute) because of the cyanosis and umbilical catheterization was done and a 10% glucose drip administered. Nasogastric tubes were also placed and permeability of the digestive tract verified (Figure 2). Initial work-up consisting of a complete blood count, C-reactive protein, glycemia, blood electrolytes, urea and creatinine were all normal. Standard thoraco-abdominal plain radiographs of the babies were all normal. A contrast thoraco-abdominal scan showed two hearts with one functional and the other residual and non functional and an interaortic defect. All the other organs were normal (Figure 3 and Figure 4). On the first day of life, they developed intermittent episodes of cyanosis. Tube feeding was started on the second day and was tolerated by both babies. As from the fourth day, the cyanotic episodes became more severe and prolonged, with apnea and respiratory distress culminating in permanent cyanosis and death on day seven despite appropriate reanimation measures. It should be noted that since the birth of these twins the parents were scared and later depressed despite the fact that they had been informed and counselled after the first ultrasound of the morphology of the babies. Discussion The etiology of conjoined twins remains unclear, but two theories have been proposed1,6, 7: 1- Fission theory which postulates incomplete division of the embryonic disc from a single fertilized ovum between the 15th and 17th day of gestation. 2-Fusion theory which proposes secondary fusion of two originally separate monovular embryonic discs. Rowena 6 , showed that fission of the developing embryo is unlikely to result in conjoined twins, but that secondary fusion of two originally separate monovular embryonic discs could be a plausible explanation. Also, it was postulated that intact skin will not fuse to intact skin, including the ectoderm of the embryo, and that two embryonic discs could be united only in those locations in which the ectoderm is normally absent or normally destined to fuse or to break down. More unusual, they may occur in triplet pregnancy 8. They are classified according to the most prominent site of union together with the suffix “pagus”, the Greek term for fixed, and are more common in females in the ratio of 3:1 1, 9. In a review of multiple pregnancies in Zaria, Northern Nigeria, Harrison and Rossiter 10 , noted that in a group of 15,020 booked women there were 357 twin pairs, six sets of triplets and one pair of conjoined twins compared with 392 twin pairs, ten sets of triplets, two sets of quadruplets and two sets of conjoined twins in 7654 emergency admissions (unbooked women). Rising maternal age, parity and height were all associated with rising twinning rate 10 . In a series of eleven sets of conjoined twins born in Southern Africa in a period of twelve months, it was postulated that conjoined twining may be the result of the interactions of an environmental agent and a latent genetic predisposition, acting at a crucial stage of fission of the embryo 11. The most common varieties and their relative frequencies are: thoracopagus or xiphopagus (joined at chest) 40%; omphalopagus (joined at the abdomen) 34%; pyopagus (joined at the buttocks) 18%; ischiopagus (joined at the ischium) 6%; craniopagus (joined at the head) 2% 1, 2,4. In a series of 12 cases of conjoined twins from West Africa between 1936 and 1978, the most common type and the ones most likely to be born alive were the omphalopagi 3. According to Rowena 12, embryologically they are classified by the proposed site of union and divided into two groups depending on the aspect of the embryonic disc involved:
The perpetual wonder, fascination and complexity of conjoined twins merits that issues relating to diagnosis, ethics and management be reviewed in a low resource context. Diagnosis The diagnosis by ultrasound was made at 37 weeks of pregnancy. Justification for this late diagnosis could be that prenatal consultations in this woman were irregular and in a district hospital with no ultrasound equipment. The diagnosis can be suspected on a prenatal ultrasound scan as early as 12 weeks of gestation, and polyhydramnios occurs in 50% of cases. The suspicious signs include inseparable foetal bodies and skin contours, unchanged relative position of the foetuses, both foetal heads persistently at the same level, and a single umbilical cord containing more than three vessels. A detailed scanning at 20 weeks will define the extent of the conjoined area and which viscera are likely to be shared. Magnetic resonance imaging (MRI) can provide a more accurate anatomical detail 1. According to Sepulveda et al 13, diagnosis in the first trimester is not always easy, with significant pitfalls in normal monoamniotic foetuses mimicking conjoined twins. The advent of transvaginal three dimensional ultrasound has permitted accurate diagnosis minimizing the possibilities of diagnostic error. An additional advantage of prenatal diagnosis is that, the time, place and mode of delivery can be planned. This is a problem in African countries where there is frequent lack of diagnostic equipment and well-trained personnel, and irregular prenatal consultations. Vaginal delivery of conjoined twins at term is virtually impossible (because of the structural morphology), that is why we deemed it necessary to do an elective caesarean section in our patient, irrespective of the poor prognostic of foetal survival. Although ultrasound estimated the gestational age of the twins at 33-35 weeks we based our decision to deliver from that of the last menstrual period (LMP) of 37 weeks. It is clear that ultrasound at this stage of pregnancy is no longer helpful in determining with precision the exact age of pregnancy. Besides, fetal biometrics from ultrasound was rendered difficult due to the multiple malformations, thus increasing the error margin of the estimated ultrasound gestational age. Ethics Infants born with severe disabilities raise unavoidable bioethical issues for parents, doctors, nurses and therapists, and the society in a broader sense. Their birth inevitably leads to controversial issues as autonomy, quality of life, acts of kindness, subjective interpretations of medical risks, and how risks and benefits are compared by doctors and theologians 14. This is also true for conjoined twins as they may be interpreted in most African societies as a sign of witchcraft in the family or a sign of bad omen inflicted on the family by its ancestors. In our case, soon after birth, the parents manifested reject and unwillingness to accept these children. Had the diagnosis been made even earlier, it would not have been possible to terminate the pregnancy as the Cameroonian penal code does not legalise abortion. Many moral, ethical and legal issues have been raised in current literature, highlighting the complex nature of decisions to be made following the birth of conjoined twins 15, 16, 17, 18, 19. Management Our conjoined twins were joined at the chest and abdomen forming a thoracoomphalopagus, with two hearts with one residual and non-functional, one liver and a defect between the two aortas. They fall in the group where non-operative management is indicated. Surgical experience with conjoined twins distinguishes three distinct categories 1, 2 : Group I: No surgical procedure would be offered where there is a complex cardiac fusion without the likelihood of constructing even a single functioning heart. Group II: Emergency separation is undertaken when one twin is dead or dying and threatening the survival of the other or when there is a correctable anomaly present which if untreated is incompatible with survival. Group III: Planned separation carried out when the infants’ condition is stable and there is time to carry out all the necessary imaging investigations to precisely define the anatomy of the union. Planned separation should ideally take place around 3 months of age when the tissues are pliable and the infants are in an optimal physiological status. Surgical management requires an experienced team of surgeons, anaesthetists, and intensivists functioning in a tertiary referral centre with the full range of medical and surgical specialities, and success depends on previous experience 1, 20. Putting together such a team in developing countries is not easy as highly trained personnel is often lacking, and coupled with poorly equipped health facilities, failures are likely to be reported than successes. Published reports of the management of conjoined twins in the African context are rare, and experience limited probably because of lack of adequate infrastructures and specialized teams. One of the earliest prowesses in the surgical separation of conjoined twins is that reported by Aird 4, on the “Kano twins” from Kano, Nigeria in 1954. They were joined by a bridge extending from the sixth costal cartilage to the navel (thoracoplagus), and were successfully separated in the Hammersmith hospital, London. Unfortunately one died one hour after surgery from adrenocortical insufficiency. Prognosis Our twins died 7 days after birth. The prognosis was certainly bad due to the associated cardiac malformation. The prognosis for conjoined twins depends on the presence of other anomalies, the extent of the union of the intracranial, intrathoracic and intra-abdominal structures, and abnormal vascular connections 21. The fatal outcome of our twins within the first 10 days after birth is consistent with data from other studies 2, 22. The survival rate also varies from one surgical team to the other, depending on their experience, 44% for Spitz and Kiely 20, in London, and 50% in those operated in the neonatal period, and 90% in those operated after 4 months for O’Neil et al, in Pennsylvania 23 . Improved recent survival is probably the result of availability of more accurate investigational studies and better anaesthetic and operative techniques with great emphasis on performing immediate reconstruction whenever possible. In future, ex vivo cardiac reconstruction and autotransplantation may permit separation of twins with complicated conjoined hearts 23. A question open to debate is whether pregnancy could be terminated in cases with poor prognosis. This raises a legal issue in countries where abortion is not legalised and should be settled within the appropriate legislative framework. Conclusion Conjoined twins, because of their complex anatomic malformation are a challenge in developing countries. This is so because early prenatal diagnosis is not often possible, due to irregular prenatal consultations coupled with inadequate antenatal care, and lack of ultrasound equipment in most health facilities. Also, lack of specialized teams, equipment and more advanced imaging techniques poses a major therapeutic challenge. It is hoped that North-South cooperation (as illustrated with the Kano twins) will help improve this situation and thus the survival rate of conjoined twins in lowresource settings. References
The following images related to this document are available:Photo images[rh09041f3.jpg] [rh09041f1.jpg] [rh09041f2.jpg] [rh09041f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}