 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
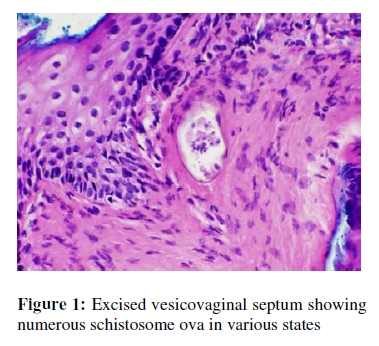
African Journal of Reproductive Health, Vol 13, No 3, September 2009, pp 137-140 CASE REPORT Schistosomiasis and Vesicovaginal Fistula Le schistosomiais et la fistule-vaginale Nora Dennis1,2, J Wilkinson3, S Robboy4 and A Idrissa5 1Duke University School of Medicine, Durham NC USA; For correspondence: Nora Dennis, MSPH, Duke University School of Medicine, Durham NC USA. Email: Nora.dennis@duke.edu ABSTRACT Schistosoma haematobium is presented as a cause of vesicovaginal fistula in a nulliparous adolescent. The possible role of S. haematobium in failure of fistula repair and the importance of screening and treatment in endemic areas prior to repair are discussed (Afr J Reprod Health 2009; 13[3]:137-140). RĖSUMĖ Le schistosoma haematobium est présenté comme une cause de la fistule vésico-vaginale chez une adolescente nullipare. Le rôle possible du schistosoma haematobium dans l’échec à l’égard de la refection de la fistule et l’importance du dépistage et du traitement dans les zones endémiques avant la refection sont discutés. (Afr J Reprod Health 2009; 13[3]: 137-140). KEYWORDS: Schistosomiasis, Schistosoma haematobium, Vesicovaginal fistula, Fistula repair Case History A 20-year old woman presented to Niamey National Hospital in Niger, West Africa with a five-year history of total urinary incontinence, with vaginal leakage of urine in all positions. She was nulligravid and never had been sexually active. At age 15, she experienced sudden onset of gross hematuria and was diagnosed with urinary schistosomiasis, which was subsequently treated with praziquantel. Following the onset of incontinence, a vesico-vaginal fistula was diagnosed. A first attempt at surgical repair failed within a month of surgery, resulting in a persistent vesicovaginal fistula. She presented four years later with persistent urinary incontinence. She had no recurrence of hematuria. Physical examination revealed a one centimeter vesicovaginal fistula in the mid-upper vagina. There was no hematuria and no evidence of recurrent schistosomiasis. Methylene blue instillation in the bladder confirmed the presence of a single fistula. Cystourethroscopy demonstrated a midline, supra-trigonal vesicovaginal fistula without inflammation or polyps. Speculum examination and bimanual examination were otherwise normal. Renal ultrasound revealed mild bilateral hydronephrosis and hydroureter consistent with the history of S. haematobium infection1,2. The vesicovaginal fistula was repaired using a transvaginal approach. The fistula tract was excised in its entirety after wide mobilization of the vaginal epithelium. The vaginal epithelium appeared normal with the exception of mild scarring around the fistula tract. The fistula was repaired in three layers using 2-0 polyglactin suture. At two weeks post-operative, the bladder was instilled with methylene blue and a successful repair was confirmed. She was re-treated with praziquantel after histologic analysis of the fistula tract revealed schistosomes. The patient remained dry at four weeks, but then presented at six weeks with recurrent urinary incontinence and a pinpoint fistula in the mid vagina at the level of the prior repair. She underwent a repeat repair of this pinpoint fistula and is currently dry at 10 weeks after surgery. Pathology The excised tissue from the vesicovaginal septum disclosed numerous Schistosome ova in various states. A rare ovum disclosed the typical terminal spine which is diagnostic of S. haematobium. A few ova appeared viable with discrete nuclear and cytoplasmic structures. The overwhelming number of ova were calcified and in various states of degeneration and mummification (Figure 1). Commentary Globally, 200 million individuals are infected with schistosomiasis. The three principal species are S. haematobium, S. mansoni, and S. japonicum. S. haematobium is responsible for most urinary schistosomiasis infections.3 In sub-Saharan Africa, where 77% of schis-tosomiasis cases are found, an estimated 43 million adults are symptomatic from S. haematobium infection, including nearly 7 million with major bladder wall pathology.3 Early signs and symptoms include hematuria, dysuria, polyuria, and proteinuria.3 Schistosome ova infiltrate blood vessels in the bladder plexus and can incite inflammatory lesions that induce the majority of associated bladder pathology.4 With severe infection, calcified ova can induce extensive fibrosis, which leads to contracted bladder mucosa5. Granulomatous inflammations can lead to ulceration and potentially fistula.6 In addition, severe chronic S. haematobium infection is associated with higher frequencies of upper urinary tract pathology.1,2 Although bladder disease, regardless of severity, generally resolves after treatment with praziquantel, upper urinary tract pathology tends not to disappear, leaving patients with persistent hydroureter, hydronephrosis, or both.6 The presence of S. haematobium ova in bladder tissue may reduce the likelihood of a successful surgical vesicovaginal fistula repair.7,8 Despite the potential for S. haematobium to cause vesicovaginal fistulae, women with urinary schistosomiasis were not found to be more likely than uninfected women to develop vesicovaginal fistulae secondary to obstructed labor.7 Impaired wound healing in the vagina has been attributed to schistosomiasis infection and this may suggest a role in fistula healing. 8 One recent case report suggests S. haematobium as a cause for vesicovaginal fistula, but causation was potentially confounded by a prior vaginal delivery. 9 This patient described in this case report had no history of sexual activity, trauma or pregnancy. The S. haematobium infection was the most likely etiology for her vesicovaginal fistula and the persistent infection may have been a significant factor in the failure of her repairs. The above data suggest that screening for schistosome ova in the urine of patients with vesicovaginal fistula could be an important pre-surgical step in areas endemic for S. haematobium. If a patient is found to be infected with schistosomiasis, treatment with praziquantel should be initiated and clearance of the infection should be confirmed prior to surgery. Dead ova may remain in the bladder tissues for months after treatment potentially inciting a persistent inflammatory response 7. At the time of surgery, fibrotic tissue around the fistula tract should be excised as this may represent the area of highest concentration of schistosomes. Knowledge of a history of schistosomiasis infection and the current stage of infection may assist in developing a realistic prognosis for repair.7 Vesicovaginal fistula is a devastating condition that generally occurs from obstructed labor and poor access to obstetric care in developing nations. Uncommon causes of vesicovaginal fistula include S. haematobium infection. This infection may also result in a higher failure rate of fistula repair. In areas where S. haematobium is endemic, it might be advisable to test for the infection preoperatively or treat empirically if testing is not available. Prospective analysis of these strategies and the impact of S. haematobium infection on vesicovaginal fistula development and repair success are recommended. References
The following images related to this document are available:Photo images[rh09042f1.jpg] |
| |||||||||

{kind=link}