 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 25-36 ORIGINAL RESEARCH ARTICLE Hypertension in Pregnancy among HIV-Infected Women in Sub-Saharan Africa: Prevalence and Infant Outcomes L’hypertension pendant la grossesse chez les femmes séropositives en Afrique subsaharienne : Prévalence et les résultats infantiles.C Kilewo1 , UCM Natchu2, A Young3, D Donnell3, E Brown4, JS Read5, U Sharma6, BH Chi7, R Goldenberg8, I Hoffman9, TE Taha10 and WW Fawzi2, 11 1 Department of Obstetrics and Gynaecology, Muhimbili University of Health and Allied Sciences; Dar es Salaam,
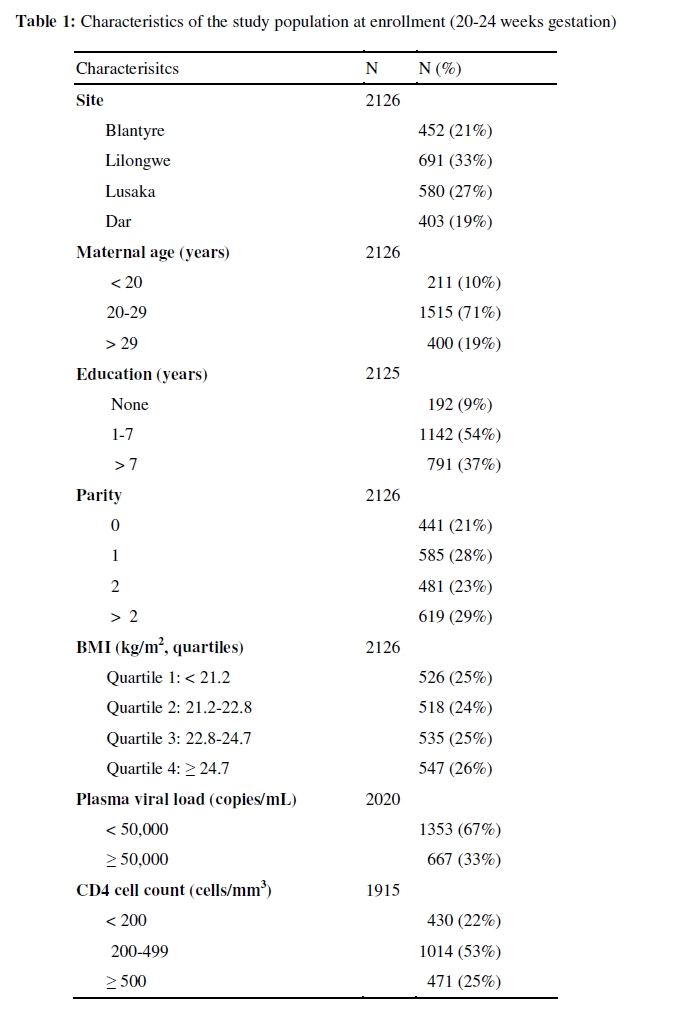
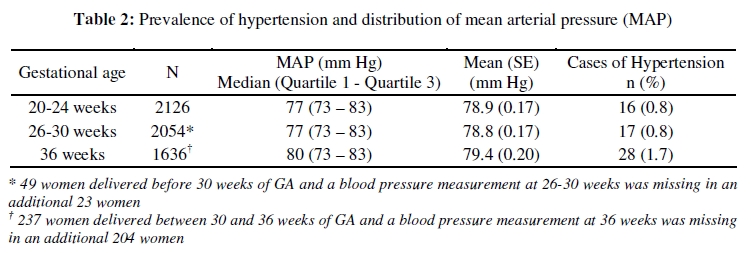
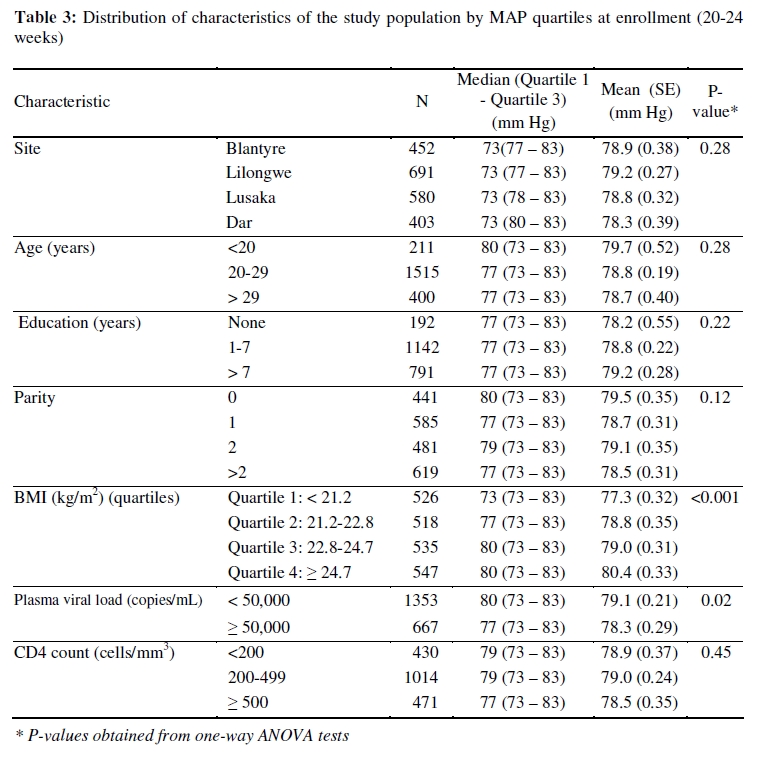
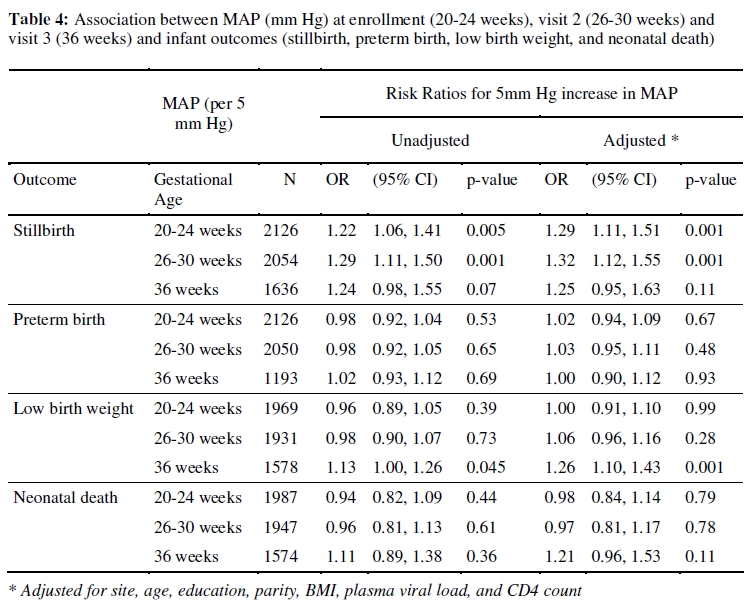
Tanzania; Code Number: rh09044 ABSTRACT This analysis was performed to determine the prevalence of hypertension and association of MAP (mean arterial pressure) with birth outcomes among HIV-infected pregnant women not taking antiretrovirals. HIV-infected pregnant women, enrolled into the HPTN024 trial in Tanzania, Malawi and Zambia were followed up at 26-30, 36 weeks, and delivery. The prevalence of hypertension was <1% at both 20-24 weeks and 26-30 weeks and 1.7% by 36 weeks. A 5 mm Hg elevation in MAP increased the risk of stillbirth at 20-24 weeks by 29% (p=0.001), 32% (p=0.001) at 26-30 weeks and of low birth weight (LBW) at 36 weeks by 26% (p=0.001). MAP was not associated with stillbirth at 36 weeks, LBW prior to 36 weeks, preterm birth, neonatal mortality or the risk of maternal to child transmission (MTCT) of HIV (Afr J Reprod Health 2009; 13[4]:25-36). RĖSUMĖ On a fait cette analyse pour déterminer la prévalence de l’hypertension et l’association de la PAM (Pression Artérielle Moyenne) avec les résultats de naissance chez les femmes séropositives enceintes qui ne prennent pas des médicaments antirétroviraux. Les femmes séropositives enceintes inscrites pour l’essai PHTNO24 en Tanzanie, au Malawi et en Zambie ont été suivies à 26 – 30, 36 semaines et à l’accouchement. La prévalence de l’hypertension était <1% à la fin de 20 – 24 semaines et à la fin de 26 – 30 semaines et 1,7% à la fin de 36 semaines. Une hausse de 5mm Hg de la PAM a augmente le risque de la mortinatalité à la fin de 20 – 24 semaines de 29% (p = 0,001), 32% (p = 0,001) à la fin de 26 – 30 semaines et de la faible poids de naissance (FPN) à la fin de 36 semaines de 26% (p = 0,001). La PAM n’était pas liée à la mortinatalité à la fin de 36 semaines, à la FPN avant 36 semaines, à la naissance avant-terme, à la mortalité néonatale ou au risque de la transmission de la mère à l’enfant (TME) du VIH (Afr J Reprod Health 2009; 13[4]:25-36). KEYWORDS: Perinatal mortality, hypertension, Africa, stillbirth, low birth weight, mean arterial pressure, pregnancy Introduction A systolic blood pressure ≥140 mm Hg or a diastolic blood pressure ≥90 mm Hg after 20 weeks of gestation is defined as gestational hypertension1 . Hypertension diagnosed prior to 20 weeks of gestation is thought to be chronic hypertension manifesting itself during pregnancy. Complications associated with hypertension during pregnancy include placental abruption and antepartum hemorrhage, eclamptic seizures, pulmonary edema and myocardial dysfunction, proteinuria, renal failure and haemolysis, elevated liver enzymes and low platelet (HELLP) syndrome 2,3 . Preterm labor and preterm birth, fetoplacental insufficiency and intrauterine growth restriction (IUGR) resulting in low birth weight and increased rates of stillbirth also have been associated with hypertension in pregnancy2,3 . Hypertension is the second most common cause of maternal mortality in Africa based on data from the World Health Organization4 . These estimates have been severely limited, however, by a lack of data from much of Africa. The prevalence of hypertension in antenatal clinics in rural Tanzania has ranged from 1.1% when blood pressures were measured by health care workers to 3.2% when measured by research study physicians5 . Rates of hypertension in pregnancy less than 2% have been reported from other countries in sub Saharan Africa6 . Infection with the human immunodeficiency virus type 1 (HIV) in pregnant women represents an independent risk factor for maternal mortality, stillbirth and IUGR 7,8 . Immune hyperactivity to paternal antigens has been hypothesized to play a role in the development of hypertension, and the immunosuppression caused by HIV could temper the immune response at the placental site and reduce placental vasoconstriction9 . This potential protection may be a function of the intensity of immunosuppression and may depend on the severity of HIV disease and the use of antiretroviral therapy. Little information is available regarding hypertension during pregnancy, its prevalence, risk factors and the effects of blood pressures on pregnancy outcomes among HIV-infected women in sub-Saharan Africa. Few interventions are currently proven to reduce the incidence of gestational hypertension. The effects of aspirin and supplementation with calcium, vitamin C, or vitamin E are yet to be studied in HIV-infected women 10-12 . Multivitamin supplementation to HIVinfected women recently has been reported to reduce the incidence of hypertension during pregnancy by 38% in a randomized trial in Tanzania13 . In the absence of consistent interventions to prevent hypertension during pregnancy, early diagnosis and management of hypertension is the only practical approach to reduce the burden of poor maternal and fetal outcomes attributable to hypertension. The usual approach to evaluating blood pressure in pregnancy has been to categorize patients into hypertensive and non-hypertensive groups. Mean arterial pressure (MAP) is considered an indicator of tissue perfusion including placental perfusion in pregnancy, and has been used as a predictor of hypertension in pregnancy 14- 16 . We therefore used the MAP as a continuous measure of blood pressure and a potential measure of placental perfusion in this study. Apart from estimating the frequency of hypertension among HIV-infected pregnant women, it is important to determine if the consequences of hypertension in this group of women are similar to those among HIV-uninfected women. The objectives of this analysis were to i) estimate the prevalence of hypertension during pregnancy among HIV-infected women not receiving antiretrovirals (ARVs) enrolled in a large clinical trial in sub-Saharan Africa, ii) to identify factors associated with MAP in these women and iii) to assess the association between MAP and stillbirth, preterm birth, low birth weight and neonatal mortality after adjusting for potential confounders. Materials and Methods HPTN 024 was a randomized, placebo-controlled trial of antibiotics to reduce mother-to-child transmission of HIV related to chorioamnionitis from July 2001 to August 2003. The study was approved by each of the in-country institutional review boards of participating clinical sites in Malawi, Tanzania and Zambia as well as U.S. partner institutions. HPTN 024 recruited patients from Blantyre and Lilongwe, Malawi; Dar es Salaam, Tanzania; and Lusaka, Zambia. Details of the study design and methods have been published previously17,18 . Briefly, women who were documented to be HIV-infected between 16-23 weeks of gestation and were willing to deliver at a study site and participate in the trial were enrolled following informed written consent at 20-24 weeks. Demographic and obstetric characteristics as well as clinical history, examination (including blood pressure measurements) and laboratory samples were obtained at enrollment (baseline visit 1 at 20-24 weeks), 26-30 weeks (Visit 2), and 36 weeks (Visit 3). Single diastolic and systolic blood pressures were measured by antenatal nurses with pregnant women in a sitting position at the study clinics using a mercury sphygmomanometer. The fifth Korotkoff’s sound (absence of sounds) was used to determine diastolic blood pressures. Complete blood counts, CD4 cell counts, and plasma viral load were measured from maternal blood samples collected during screening. Plasma viral load measurements were performed at the University of North Carolina, Chapel Hill, NC, USA, using the Roche HIV-1 Amplicor Monitor assay, version 1.5 (Roche, Branchburg, New Jersey, USA). Study Population and Definitions HIV-infected pregnant women enrolled in HPTN 024 who were known to have delivered and who had at least one blood pressure measurement prior to delivery were included in the analysis. Women were defined as hypertensive if the systolic blood pressure was > 140 mm Hg or the diastolic pressure was ≥90 mm Hg during any clinical examination. The MAP was calculated at each visit using the following formula: MAP = (systolic blood pressure + 2 x diastolic blood pressure)/3. Infants with a birth weight < 2500 g were categorized as low birth weight. Preterm birth was defined as a gestational age < 37 weeks, as assessed by fundal height measurement at the first study visit. All pregnancies that did not result in the delivery of a live born infant were defined as stillbirths. Deaths of infants within 28 days after birth were classified as neonatal deaths. Statistical Analysis Descriptive statistics were calculated for categories of maternal characteristics, and one way ANOVA tests were performed to compare the mean MAP values. Univariate and multivariable logistic regression models were fit to predict various outcomes (stillbirth, preterm birth, low birth weight, and neonatal death) from MAP and these maternal characteristics. Unadjusted and adjusted models were fit for each outcome at each time point MAP was measured. Women who delivered prior to the 26-30 week visit were excluded from the analyses at 26-30 weeks and 36 weeks, and women who delivered prior to 36 weeks were excluded from the analysis at 36 weeks. Study site, maternal age and education, parity, baseline BMI, plasma viral load and CD4 cell count were included a priori in multivariate modeling. Results Of the 2294 HIV-infected women enrolled in the HPTN 024 study, 2126 (92.7%) had at least one blood pressure measurement and delivery information available. Characteristics of these 2126 women are shown in Table 1. Table 2 displays information regarding MAPs at 20-24 weeks, 26-30 weeks, and 36 weeks, along with the number of cases of hypertension at each of these time periods. Mean MAPs at the screening visit were compared across categories of variables included in Table 1. As shown in Table 3, the mean MAP was significantly associated with BMI and plasma viral loads. Analyses of MAP at 26-30 weeks and 36 weeks yielded similar results (data not shown). Seventy-four of 2126 (3.5%) pregnancies ended in stillbirth (15/26 deliveries before visit 2, 31/384 deliveries between visit 2 and visit 3 at 36 weeks, and 28/1716 of deliveries after visit 3). Preterm birth occurred in 547 of the 2126 (26%) pregnancies. Low birth weight was observed in 288 of 1969 (15%) pregnancies that resulted in live births where birth weight was recorded. Neonatal deaths occurred among 89 of 2061 (4.3%) live born infants. In unadjusted analyses, a higher mean arterial pressure at enrollment and at 2630 weeks was associated with a greater risk of stillbirth (Table 4). Also, a higher mean arterial pressure at 36 weeks was associated with low birth weight. These associations remained statistically significant in analyses adjusted for study site, age, education, parity, BMI, viral load, and CD4 count. MAP at 36 weeks was not associated with stillbirths and MAPs at enrollment and at 26-30 weeks were not associated with low birth weights in unadjusted and adjusted analyses. In both unadjusted analysis and analysis adjusted for the above parameters, mean arterial pressures at any of the three time points were not associated with preterm delivery, neonatal death or maternal to child transmission of HIV (Table 4). Discussion The prevalence of hypertension was 1.7% at 36 weeks of gestation, lower than most studies from Africa19 . However, studies of hypertension in pregnancy from Africa have mostly focused on high risk groups or hospital-based populations which yield higher and potentially biased rates of hypertension in pregnancy 20,22,23 . These women were enrolled at their first contact with health care services and, HIV infection status aside, are likely to be a representative sample of pregnant women in these areas. The lack of blood pressure measurements during the intrapartum and immediate postpartum period also contributes to a lower prevalence of pregnancy induced hypertension. Women who become pregnant before the age of 18 or after the age of 35 years have been shown to be at an altered risk for hypertension and obstetric complications 21,22 . Women below the age of 18 years were excluded in the HPTN 024 trial, and only 3% of enrolled women were older than 35 years (n=69/2126). This may also contribute to the lower frequency of hypertension in this analysis. Higher BMI and a viral load lower than 50,000 copies/mL predicted higher mean arterial pressures in our study. Throughout the entire follow up period from 20-24 weeks to 36 weeks, the difference in mean MAP between the lowest and highest quartile of BMI was only 3.0 mm of Hg, suggesting a low variability in blood pressures in this study population. Despite being in the second or third trimester of pregnancy, only 25% of the population had a BMI greater than 24.7. Yet, in a population with very few “overweight or obese” pregnant women, we observed higher MAP to be associated with higher BMI. The association of lower mean MAPs with higher viral loads seen here could be explained by lower BMIs seen among women with higher viral loads or may support a hypothesis that implicates the immune system in the etiology of gestational hypertension9 . Blood pressure measurements at three intervals in the second and third trimesters allowed us to study the associations of elevations in MAPs on stillbirth and preterm birth at various stages of pregnancy. We found that higher MAP readings at 20-24 and 26-30 weeks were associated with an increased risk of stillbirth. The lack of a significant association between MAP and stillbirth at 36 weeks could be explained by two possibilities. The first is that a large proportion of fetuses at risk for fetal loss ended in stillbirth prior to 36 weeks and the remaining pregnancies that ended in stillbirth were inadequate to provide sufficient power. The other explanation is that small increases in MAP late in pregnancy (near term) are insufficient to lead to stillbirth but are sufficient to impede fetal growth and contribute to low birth weight. This latter explanation is supported by a very significant association found between MAP and low birth weight near term. We found no association between MAP and other infant outcomes (preterm birth, neonatal mortality and maternal-to-child transmission (MTCT) of HIV) in this study. Only a few maternal deaths were observed and, therefore, associations between MAP and maternal mortality were not described. In experimental models, adequate feto-placental perfusion has been shown to depend on optimum blood pressures and uterine blood flow24 . The relationship between MAP and fetoplacental perfusion is yet to be clearly elucidated. Given its ease of measurement, our study explores the use of MAP as a risk factor for adverse infant outcomes (stillbirth, low birth weight, and neonatal mortality). Nearly 99% of our study population had blood pressures in the non-hypertensive range; very few, therefore, had higher than normal MAPs. One of our limitations was that this trial was not primarily designed to assess hypertension in pregnancy; therefore blood pressures were not measured twice at 4 hour intervals or on successive days as would be indicated in strict research protocols to capture and control variability in blood pressure measurements. During routine antenatal care, only one blood pressure measurement is made during each visit, as was done in this study, making the results directly interpretable for practical use during routine antenatal care. Antenatal nurses recruited and trained for this tral performed blood pressure measurements at each of their antenatal centers. Multiple measurements by more than one observer were not performed and inter and intra-observer viariability could not be estimated. Similarly, fundal height is likely to remain the best measure to determine gestational age in large populations with limited access to antenatal ultrasonography. This study is one of the few studies on hypertension during pregnancy to be conducted on a large population of HIVinfected women who were not receiving ARVs in sub-Saharan Africa. Our results suggest that this population has a low incidence of hypertension during pregnancy. Nevertheless, higher MAPs are associated with poor perinatal outcomes such as stillbirth and low birth weight in this population. Antiretroviral therapy may be associated with metabolic changes in the body, which predispose to an increase in MAP, hypertension and other cardiovascular morbidity25 . As more pregnant women in these regions gain access to ARVs, changes in immune status, BMI, metabolism and blood pressure might occur. These changes could lead to higher rates of hypertension, pre-eclampsia and stillbirth 26. The associations observed in our analysis, if replicated in other populations, will provide support to use MAPs during antenatal care to identify high-risk pregnancies and for measures that can prevent population changes in blood pressures thereby influencing the incidence of low birth weight and stillbirth in such populations. Financial Support and Sources The HPTN 024 Trial was supported by the HIV Network for Prevention Trials (HIVNET) and sponsored by the US National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Health (NIH), Department of Health and Human Services, through contracts NO1-AI-35173 with Family Health International, NO1-AI-45200 with Fred Hutchinson Cancer Research Center, and subcontract NO1-AI-35173117/412 with Johns Hopkins University. In addition, the trial was supported by the HIV Prevention Trials Network (HPTN) and sponsored by NIAID, the National Institute of Child Health and Human Development, National Institute on Drug Abuse, the National Institutes of Mental Health, and the Office of AIDS Research of the National Institutes of Health, U.S. Department of Health and Human Services, Harvard University (U01-AI48006), Johns Hopkins University (U01-AI-48005), and the University of Alabama at Birmingham (U01-AI47972). Nevirapine (Viramune®) for the study was provided by Boehringer Ingelheim Pharmaceuticals, Inc. The conclusions and opinions expressed in this paper are those of the authors and do not necessarily reflect those of the funding agencies and participating institutions. Acknowledgments HPTN 024 Team: Protocol Co-Chairs: Taha E. Taha, MD, PhD (Johns Hopkins University Bloomberg School of Public Health); Robert Goldenberg, MD (University of Alabama at Birmingham); In-Country Co-Chairs/Investigators of Record: Newton Kumwenda, PhD, George Kafulafula, MBBS, FCOG (Blantyre, Malawi); Francis Martinson, MD, PhD (Lilongwe, Malawi); Gernard Msamanga, MD, ScD (Dar es Salaam, Tanzania); Moses Sinkala, MD, MPH, Jeffrey Stringer, MD (Lusaka, Zambia); US Co-Chairs: Irving Hoffman, PA, MPH (University of North Carolina, Chapel Hill); Wafaie Fawzi, MD, DrPH (Harvard School of Public Health); In-Country Investigators, Consultants, and Key Site Personnel: Robin Broadhead, MBBS, FRCP, George Liomba, MBBS, FRCPath, Johnstone Kumwenda, MBChB, MRCP, Tsedal Mebrahtu, ScM, Pauline Katundu, MHS, Maysoon Dahab, MHS (Blantyre, Malawi); Peter Kazembe, MBChB, David Chilongozi, CO, MPH, Charles Chasela, CO, MPH, George Joaki, MD, Willard Dzinyemba, Sam Kamanga (Lilongwe, Malawi); Elgius Lyamuya, MD, PhD, Charles Kilewo, MD, MMed, Karim Manji, MD, MMed, Sylvia Kaaya, MD, MS, Said Aboud, MD, MMed, Muhsin Sheriff, MD, MPH, Elmar Saathoff, PhD, Priya Satow, MPH, Illuminata Ballonzi, SRN, Gretchen Antelman, ScD, Edgar Basheka, BPharm (Dar es Salaam, Tanzania); Victor Mudenda, MD, Christine Kaseba, MD, Maureen Njobvu, MD, Makungu Kabaso, MD, Muzala Kapina, MD, Anthony Yeta, MD, Seraphine Kaminsa, MD, MPH, Constantine Malama, MD, Dara Potter, MBA, Maclean Ukwimi, RN, Alison Taylor, BSc, Patrick Chipaila, MSc, Bernice Mwale, BPharm (Lusaka, Zambia); US Investigators, Consultants, and Key Site Personnel: Priya Joshi, BS, Ada Cachafeiro, BS, Shermalyn Greene, PhD, Marker Turner, BS, Melissa Kerkau, BS, Paul Alabanza, BS, Amy James, BS, Som Siharath, BS, Tiffany Tribull, MS (UNC-CH); Saidi Kapiga, MD, ScD, George Seage, PhD (HSPH); Sten Vermund, MD, PhD, William Andrews, PhD, MD, Deedee Lyon, BS, MT(ASCP) (UAB); NIAID Medical Officer: Samuel Adeniyi-Jones, MD; NICHD Medical Officer: Jennifer S. Read, MD, MS, MPH, DTM&H; Protocol Pharmacologist: Scharla Estep, RPh, MS; Protocol Statisticians: Elizabeth R. Brown, ScD, Thomas R. Fleming, PhD, Anthony Mwatha, MS, Lei Wang, PhD, Ying Q. Chen, PhD; Protocol Virologist: Susan Fiscus, PhD; Protocol Operations Coordinator: Lynda Emel, PhD; Data Coordinators: Debra J. Lands, Ed.M, Ceceilia J. Dominique; Systems Analyst Programmers: Alice H. Fisher, BA, Martha Doyle; Protocol Specialist: Megan Valentine, PA-C, MS. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09044t2.jpg] [rh09044t4.jpg] [rh09044t3.jpg] [rh09044t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}