 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
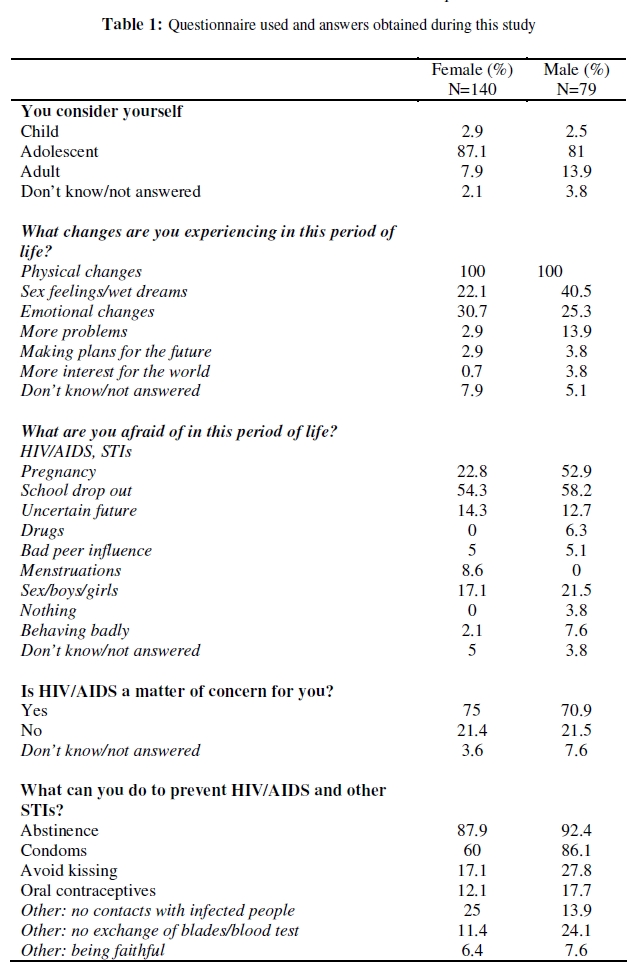
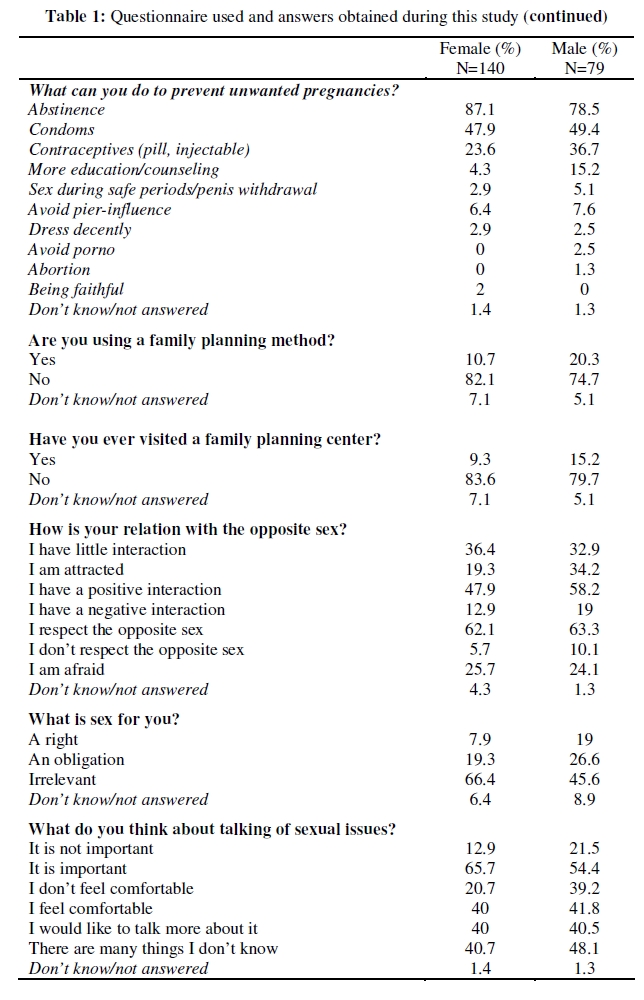
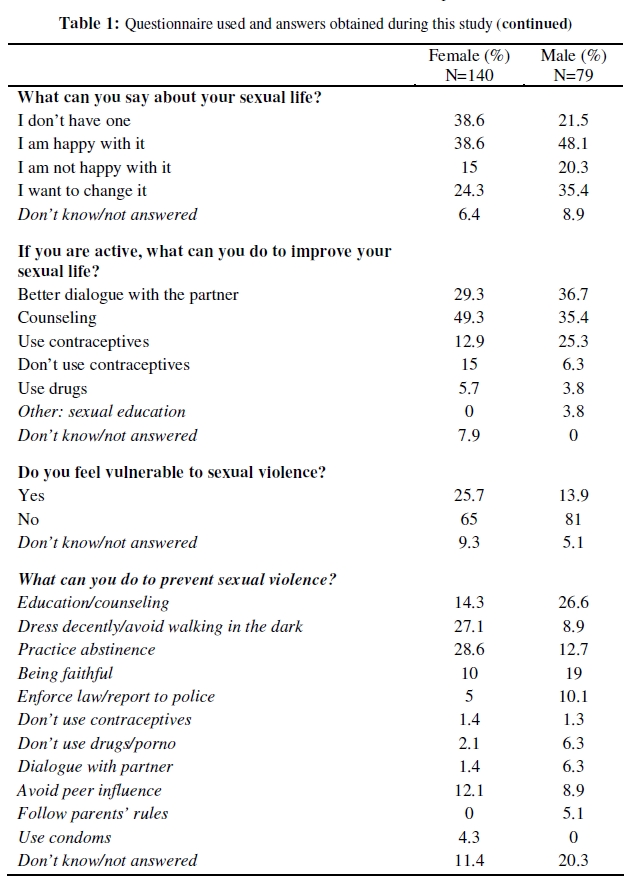
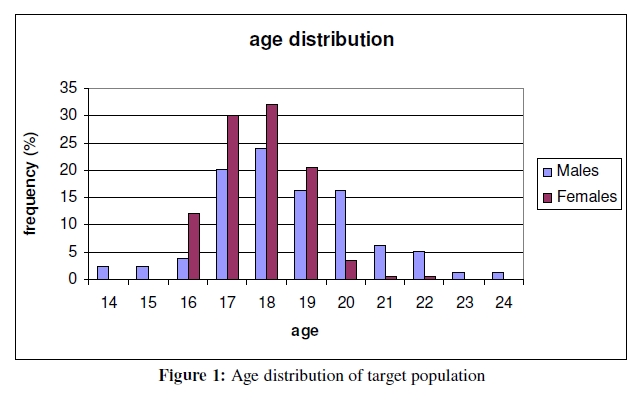
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 51-66 ORIGINAL RESEARCH ARTICLE Knowledge, Attitude and Practices Study on Reproductive Health Among Secondary School Students in Bolgatanga, Upper East Region, Ghana Etude de la connaissance, de l’attitude et des pratiques concernant santé de la reproduction chez les secondaires à Bolgatanga, à Upper East Région au GhanaSimona Rondini1 and John Kingsley Krugu2 1Novartis Vaccines Institute of Global Health, via Fiorentina 1, 53100 Siena, Italy; Code Number: rh09046 ABSTRACT This study was conducted within the secondary school student population of the Bolgatanga community, in Northern Ghana, to learn about knowledge, attitude and practices of reproductive health of this adolescent student population. Both quantitative and qualitative data were collected on adolescence perception, STIs and HIV/AIDS, family planning, male-female relationship, and vulnerability to sexual violence. The data collected show a concerning low familiarity of the student population with family planning methods and HIV/AIDS transmission, which, combined with minimal contraceptive use, pose them at high risk for unwanted pregnancies and sexual infections transmission. We argue that poor infrastructures and low accessibility of these rural areas in Northern Ghana may have led to uneven distribution of reproductive health educational programs in the country, urging more programs and interventions aimed particularly at these high risk groups (Afr J Reprod Health 2009; 13[4]:51-66). RĖSUMĖ Cette étude a été menée au sein de la population des étudiants des écoles secondaires dans la communauté de Bolgatanga au nord du Ghana afin de nous renseigner sur la connaissance, l’attitude et les pratiques de la santé de reproduction chez cette population adolescente. Nous avons collecté des données quantitatives et qualitatives sur la perception de l’adolescence, les ISTs et le VIH/SIDA, la planification familiale, le rapport hommefemme et la vulnérabilité à la violence sexuelle. Les données collectées ont montré une faible familiarité inquiétante au sein de la population estudiantine avec les méthodes de la planification familiale et la transmission du VIH/SIDA qui, combinée avec l’emploi minimal du contraceptif, les expose à un haut risque pour des grossesses non voulues et la transmission des infections sexuelles. Nous soutenons que les mauvaises infrastructures et la basse accessibilité de ces régions rurales au Ghana du nord ont peut-être conduit à la distribution inégale des programmes éducatifs de la santé de la reproduction dans le pays en recommandant davantage de programmes et d’interventions qui visent en particulier ces groupes à très haut risque (Afr J Reprod Health 2009; 13[4]:51-66). KEYWORDS: In-School Adolescence; Reproductive health; Northern Ghana Introduction Adolescence is a challenging phase of life, within which the individual attains physical, sexual and social maturity. Being an adolescent in Northern Ghana is especially challenging: the youth is mostly left alone to face the HIV/AIDS epidemic, the risks of sexually transmitted illnesses (STIs), unwanted pregnancies and unsafe illegal* abortions. Furthermore, sexual violence is becoming increasingly prevalent. There are 920.000 people living in the Upper East Region1 , and approximately 70.000 live in Bolgatanga. According to national statistics, 47.7% of the population in Bolgatanga District is less than 15 years old. Only 15.7% of the population lives in urban areas, making the Upper East Region the least urbanized region in the country (www.ghanadistricts.com). The youth is particularly at risk for STIs, among which HIV/AIDS, whose occurrence has been on the increase in Ghana since 2000, after a seeming decline in the late nineties. HIV/AIDS prevalence rate increased from 2.3% in 2000 to 3.6% in 2003 in the 15-24 year old age group2 . The slight abating in frequency recorded in 2004 (3.1%) represented the first decrease over the past previous four years. However, this positive trend did not reflect the situation of the Bolgatanga community, where HIV/AIDS prevalence peaked to 3.8% in 2004. As a matter of fact, Bolgatanga was one of only three sentinel sites, among the 35 chosen to represent the entire Ghanaian territory, to show a constant increase of HIV/AIDS prevalence rate over the last four years. The highest mean HIV prevalence was recorded in the 25-29 year old age group (4.5%), while the mean prevalence in the 15-19 group was 2.0% and in the 15-24 group was 2.5%3 . Considering the time gap between infection and HIV/AIDS manifestation, it correlates that a large number of infections occur during adolescence. Although educational campaigns on HIV/AIDS prevention and family planning had a strong positive impact on married women, with a recorded 41% increase of modern contraceptives use from 1998 to 2003 (and a dramatic decline of fertility from 6.4 births per woman in 1998 to 4.4 in 2003), this downward turn has stalled in more recent years3 . More worrisome are the data obtained from sexually active Ghanaian adolescents, who, since the revision of the National Population Policy in 1994 (after the Cairo International Conference on Population and Development)4 , became the target of many of such programs like the “ABC” campaign, promoting abstinence, being faithful and utilizing condoms5,6 . Despite those efforts, it is estimated that 80% of females and 63% of males in the 15-19 year old group currently do not use any modern method of contraception5 and analysis of links between knowledge, behavior and HIV serostatus have shown little translation of health knowledge into protective behavior7 . It is difficult to define which factors influence adolescent risk-taking and health-seeking behavior, since multiple categories of risk-related factors operating at individual, family, community and societal level play important contributions8 . More specifically, in a region such as Northern Ghana where it is societal taboo to discuss issues of sexuality, it is possible that educational campaigns could not always guarantee that adolescents received accurate information to halt the perpetuation of myths and misconceptions. This report, part of a broader initiative of the Youth Harvest Foundation Ghana (YHFG, www.yhfg.org) on adolescent sexual reproductive health, presents findings from a baseline study conducted within the secondary school student population of the Bolgatanga community, to evaluate pre-existing knowledge and practices among this high-risk age group. Materials and Methods Study goal The aim of the present study was to learn about the knowledge, attitudes and practices of reproductive health among adolescent students in Bolgatanga. Although studies on adolescence usually consider a five-year age range (15 to 19) as their primary source of data, we used the term adolescence flexibly, allowing it to stretch into the early twenties. Both the possibility of secondary school completion and the increase of average age at first marriage can in fact be considered factors that contribute to widen the transition from childhood to adulthood9 . Study area This study was carried out in Bolgatanga, district capital of the Bolgatanga Municipal District, and regional capital of the Upper East Region. The Upper East Region is located in the Northeastern corner of the country and bordered by Burkina Faso to the North and Togo to the East. The Upper East Region is divided into 8 districts and the Bolgatanga Municipal District is located in the center of the region. It has a total land area of 729 sq km and is bordered to the North by the Bongo District, South and East by Talensi-Nabdam District and Kassena-Nankana District to the West. Although the majority of the inhabitants are from northern ethnic origins, there has been a huge influx of the major ethnic groups of Ghana (including the Akans, Ewes, and Ga-Adanbge) into the town because of its regional capital status. The settlement pattern is predominantly rural (about 95%) with dispersed buildings. The Upper East is the only region in Ghana where adherents of traditional religion (in comparison with Christians and Muslims) are close to one-half of the population. Although the Upper East Region has an overall level of educational attainment much lower than the country as a whole, with a level of illiteracy (78.1%) significantly higher than the national average (45.9%), Bolgatanga records the highest literacy rate of the region (27.7%). Similarly, Bolgatanga records the lowest proportion of the population aged 6 years and over who have never attended school (61.2%) within the Upper East Region (71.8%). Among the ones who had ever attended school, about the half attains primary level, while just 5.2% attains vocational/technical/commercial education. At every level of education, there is a higher proportion of males than females. Basic education in Ghana consists of nine years of schooling: six years of primary school (6-11 year old pupils) and three years of junior secondary school (12-14 year-old pupils). The basic nineyear schooling is compulsory. Basic education is followed by three years of secondary education, either in senior secondary school (SSC), vocational school, or technical school. The age range for this level is typically 15-17. The tertiary level consists of all postsecondary education like polytechnic, university and teacher and nurse training. Study design The study took place in March 2007, and participation in the study was voluntary. The study population comprised students from five different schools in Bolgatanga: Bolgatanga Technical Institute (Botech), Bolgatanga Secondary School (Bigboss), Zuarungo Secondary School (Zuss), Zamse Secondary Technical School (Zamsetech) and the female-only Bolgatanga Girls Secondary School (Bogiss). An additional femaleonly school, the Bolgatanga Vocational Institute (formerly known as Women Training Institute, WTI) participated exclusively in the focus group discussions and not in the survey. The schools represent different typologies: Botech is a technical institute, WTI is a vocational institute, and the other four are secondary schools. Zamsetech and Zuss are both day/boarding schools, the others are full boarding schools. The target schools were chosen for their proximity to the YHFG office. Both qualitative and quantitative data were collected for this study (Table 1 a, b, c). Qualitative data were collected through 12 focus group discussions (FGD), where 6 groups of 20 to 40 students from each school participated in two consecutive meetings. A total of about 250 students aged 15-24 were involved. The discussions were facilitated by a guide prepared to lead the meeting, supported by another YHFG member. Quantitative data were collected through a questionnaire, which included open and closed questions on knowledge, attitudes and practices related to reproductive health. The questionnaire was in English, since all the students were completely proficient in the English language. A sample size of 219 students from the selected schools (except for the Women Training Institute) answered the questionnaire. This study took advantage of prior research conducted in three Ghanaian regional capitals (Takoradi, Also in the current study, both the FGD Sunyani and Tamale)10 , and in Dodowa11 , and the questionnaire contained aspects where a wider range of reproductive related to adolescence, STIs and health and gender issues were addressed. HIV/AIDS awareness, male-female relationships and vulnerability to sexual violence. Results General characteristics of target population In the overall sample, there were more females than males (Table 2) due to the participation of one female-only school in the survey. The data obtained from the survey were initially stratified by sex and school to see if differences in the school determined different answers among the students. No significant differences imputable to the school were found, therefore all the data were pooled together and just the sex stratification was maintained. On the other hand, the FGD manifested a different dynamic when they took place in mixed-sex schools versus female-only schools (Bogiss and WTI). The typical pattern was that the female students were less likely to participate in the discussion in the presence of their male colleagues. Despite the increased shyness noted in the mixed schools, the students demonstrated a general openness and interest in talking about reproductive health topics. Age-related changes and perceptions The median age (Figure 1) of both groups was 18 (range male population: 14-24, range female population: 16-23), and 81% of males and 87% of females considered themselves adolescents. A higher proportion of males (13.9% versus 7.9% of females) considered themselves adults. To the open-ended question about what major changes they are experiencing in this period of life, 100% of both sexes perceived that physical changes (growth of hair, enlargement of body parts such as breasts, chest and hips, change of voice, beginning of menstruations etc.) represented the major transformations. Almost a double percentage of males compared to females indicated an increase of sexual feelings (40.5% versus 22.1%), while females addressed more often emotional changes (30.7% versus 25.3% in the male population). Interestingly, male students seemed to be more worried about “problems” in general compared to females (13.9% versus 2.9% males). Specifically they mentioned school fees, food provision, problems of concentration, etc., while females mentioned “disturbance from the opposite sex” as their main problem. When confronted with the open question of what they fear most in this period of their lives, the most prevalent answer for both groups was STIs transmission and HIV/AIDS (58.2% males and 54.3% females). In particular, when they were asked if HIV/AIDS represented a matter of concern to them, both groups homogeneously answered “yes” in more than 70% of the cases (70.9% males and 75% females). Among the other STIs, the most frequently cited were gonorrhea followed by syphilis, but both groups demonstrated very little knowledge of other STIs and their symptoms. Lack of trust in the local health service was mentioned, with the health providers perceived as people that “give you a drug without telling you what it is and what you have”. Pregnancy was another cause of major concern, specifically among females (52.9% versus 22.8% males). For both groups, “dropping out of school” and general “uncertainty in the future” were matters of concern (19% and 12.7% among males and 15% and 14.3% among females). Similarly, “negative peer influence” was mentioned by both groups (5.1% males and 5% females). Two genderspecific fears were the “use of drugs”, mentioned just by the male population (6.3%), and, predictably, “menstruations” mentioned just by females (8.6%). During the FGD, many girls said that they did not know how to handle menstrual pain; additionally they were worried because of irregular cycles, and they expressed concern about the coincidence of sex and menstruation. One of their beliefs was that “blood would go up to the stomach if having sex when menstruating”. Prevention of STIs and HIV/AIDS To the open-ended question of how they can prevent HIV/AIDS and other STIs, both groups mentioned abstinence as the method of choice (92.4% males and 87.9% females). Condom use was mentioned by 86.1% of the males and by only 60% of females. Condom use was a highly controversial topic; in fact, the widespread knowledge of condoms’ availability did not seem to translate into their consistent use. “I don’t use condoms because they are not effective” was a common statement. Additionally, many students believed that “they are not made for Africans and they cannot resist the African heat”. Just a few students admitted not to know their correct use, and a general reported malpractice was to start using them after sexual intercourse has already begun. Another debated issue was on “how many times a condom can be used”, which illustrated the poor understanding of their correct utilization. Female condoms were very little known and very few students could explain how to use them. Additionally, the students showed a significant attitudinal barrier to condom use: females would not purchase condoms out of shyness and fear of being judged as “bad girls”. Males, on the other hand, would not accept a condom from a girl, because this implied that “the girl is not to be trusted”. Condom use, in fact, seemed to be highly linked with trust, therefore its negotiation can become extremely difficult, with girls unable to enforce their use due to the risk of being stigmatized. In both groups, the use of contraceptive pills (mentioned by 17.7% males and 12.1% females) and avoidance of kissing (mentioned by 27.8% males and 17.1% females) was considered a way to prevent HIV/AIDS infection. Also, avoiding contact with an infected person (13.9% males and 25% females) and being faithful to the partner (7.6% males and 6.4 % females) were considered methods to preventing infection. These data show the incomplete knowledge about STIs and HIV/AIDS transmission among adolescents, which puts them at high risk. Furthermore, their reliance on fidelity did not seem to take into account the possibility that a partner may have had multiple sexual relations before the present one, where he may have contracted (and transmitted) the disease. Blood testing to check HIV infection was rarely taken under consideration. Family planning As in the case of STIs and HIV/AIDS prevention, the most common response to how to prevent unwanted pregnancies was “abstinence” in 78.5% of males and 87.1% of females. Condoms were mentioned by about 48% of both groups, and other contraceptives (oral and injectables) were mentioned by 36.7% of males and 23.6% of females. Fewer students (5.1% males and 2.9% females) mentioned “penis withdrawal”, or limiting sexual practice to “safe periods”, even though they had a very vague idea of what “safe periods” signify. Particularly among males, an emphasis was placed on sexual education and counseling in order to prevent unwanted pregnancies (15.2% males versus 4.3 females). When asked whether they use any family planning method, 74.7% of males and 82.1% of females answered “no”. Additionally, about 80% of both males and females answered that they never visited a family planning center. Perception of sex When asked about their relation with the opposite sex in a multiple choice question, 58.2% of males and 47.9% of females selected “positive”, while almost the double percentage of males (34.2% versus 19.3% females) chose “I feel attracted by the opposite sex”. More than 62% of both groups selected “I respect the opposite sex”, while almost a double percentage of males (10.1% versus 5.7% females) chose “I don’t respect the opposite sex”. About 1 in 5 students of both groups selected “I am afraid of the opposite sex”. The perception they had of sex was mainly described as being “irrelevant” for both groups (45.6% males and 66.4% females). In the male population, the proportion of responders who considered sex an “obligation” (26.6%) was 8percentage points higher than those who considered sex a “right” (19%). In the female population this disparity was higher (obligation: 18.3%, right: 7.9%). The perception of sex as an obligation may come from widespread beliefs, such as “if a boy at that age does not have sex becomes blind, or if it is a girl, she becomes stupid”, and from the equation that love is sex. As in a previous study (10), our FGDs similarly highlighted the fact that most adolescents approach sex without any preparation and with an all-or-nothing tactic12 . Some girls did not know “if it is normal to have pain or bleed while having sex”, and they did not seem to experience all the intermediary steps before sexual intercourse. Especially the male group stated discomfort in discussing sexual issues (39.2% versus 20.7% female), but both groups perceived it as important (54.4% males, 65.7% females). They affirmed they would like to talk about it more (about 40% both groups) since there are many things they do not know (48.1% males versus 40.7% females). While declaring to be happy with their sexual life (48.1% males and 38.6% females), many would still like to change it (35.4% of the males and 24.3% of the females). It is interesting to note that the same percentage of females who declared to be happy with their sex life, also stated not to be sexually active. Ways to improve sexual life were identified as creating a better dialogue with the partner and receiving counseling. Also, either contraceptive use (25.3% males, 12.8% females), or the avoidance of contraceptives (6.3% males, 15% females) was similarly considered a way to improve sexual satisfaction. Vulnerability to sexual violence 25.7% of females versus 13.9% of males felt vulnerable to sexual violence and, when asked how they think they could prevent it, both groups highly ranked “education and counseling” (26.6% males, 14.3% females). Interestingly, in the female group the most common answers were “dress decently”, or “do not walk in the dark” (27.1% versus 8.9% males). Discussion Adolescence as a transition phase between childhood and adulthood is a relatively new concept in developing countries, where such transition tended to be a more rapid event marked by the beginning of reproductive maturity. Adolescent reproductive health is receiving increased attention in Ghana, where almost half of the population is below 15 year-old2 with teenage pregnancy being a prominent social and health issue. Early initiation of sexual activity and non use of contraception have increased the period of risk for nonmarital pregnancy and exposure to STIs, which beyond the repercussions on young individuals and their families impose a heavy cost on society. Ghanaian society is made of about 40% of the population who lives in poverty, with the Upper East, Upper West and Northern regions being the most affected13 . Poverty and poor school attendance are among the factors that correlate with the current disuse of contraception14 . As a matter of fact, the Upper East together with the Northern Region report the lowest use of contraceptives (12%) in Ghana2 . Additionally, rural women have nearly twice as many children as urban women2 . The Upper East population lives mostly in rural areas (85%) (ghanadistricts.com), yet there are fewer well equipped health facilities compared to the southern regions. Since the introduction of reproductive health campaigns, more than 90% of adolescents reported knowing at least one modern method of family planning15 . In our study group, abstinence was indicated as the method of choice to prevent both STIs and pregnancy, while male condoms were only mentioned by less than half of the respondents in both groups. This provides a much lower percentage compared to what recorded in the 2004 survey5 , where 88% females and 91% males indicated the use of male condoms to prevent unwanted pregnancies. A similar discrepancy was seen regarding the use of oral and injectable contraceptives, which in our study group was reported just by one in three males and one in four females, while in the 2004 HIV survey3 more than half of the adolescents mentioned them. Such differences may reflect an uneven distribution of reproductive health programs, which are less available for adolescent populations in the North of Ghana compared to the national coverage. On the other hand, the reproductive health campaigns to which the students have been exposed seemed to emphasize abstinence over other family planning methods. This may result in lacunae among sexually active youth in their familiarity with the available tools that can be used for adequate protection. During the FGD in fact, knowledge appeared to be very superficial, and it was clear that at least part of the inefficacy of condoms claimed by the students is due to poor notions of their correct use. Also in the 2004 survey5 it was reported that one in five male adolescents start having sex before putting on a condom, thus compromising its protective effect. Beyond this, condoms are seen as a male responsibility, with females too embarrassed to purchase them and even to propose them to their partners. The survey did not produce quantitative data, but it seems in line with a study carried out in the Central Region, where 40% of adolescents aged 12-24 would consider a girl carrying a condom in her purse “bad” 16 . The low level of contraceptive use was also very alarming, with 74.7% of males and 82.1% of females reporting not to use any family planning method. Of course a portion of the students may not be sexually active, but considering that it is estimated that 30% of females and 16% of males 15–19 years have had sex15 , and that in our study the median was 18 for both groups, at least a part of both populations can be considered sexually experienced. Moreover, subnational studies have shown different median ages of sexual initiation. For example, a study conducted in Keto South, Upper Denkyira and Offinso electoral constituencies showed a median age of 16 (17), while another survey conducted in 9 secondary schools showed that 15 was the average age18 . It is interesting in this regard to notice that although females may be proportionally more active than their male colleagues, they reported a lower use of family planning methods. This observation may be linked with the answer to the question on “how you can improve your sexual life”, where more than twice as many females than males responded with “avoidance of contraceptives”. This may come from pressure exerted by their older partners. The fact that these data come from a student population is particularly worrying. In fact, according to national statistics, women with some secondary education are more than twice as likely to use contraception as women with no education. Additionally, women in urban areas are more likely to use contraceptive methods than their rural counterparts (31 versus 21%). 2 Although many media campaigns developed by the Ghana Social Marketing Foundation and youth-focused services promoted by the Ghana Health Service were aimed to provide information on HIV/AIDS, since “nobody should die of ignorance”, there are still serious gaps of knowledge about disease transmission. According to the 2004 national survey5 , 95% of adolescents heard about HIV/AIDS, however one in five reported misconceptions on HIV/AIDS transmission. Our study evidences that this absence of correct information is present especially among females, where just 60% of them mentioned condom use as a prevention method. Additionally, erroneous ideas such as using contraceptive pills, or avoiding contact with an infected person in order to prevent the disease, were widespread. Those dangerous convictions constitute signs of risky behavior, which can further contribute to the stigmatization of the people affected by AIDS. As a consequence, in fact, it has been reported that one in five people would not buy fresh vegetables from a vendor with AIDS, and between 51 and 63% thought that a female teacher with AIDS should not be allowed to teach3 . Also the youth reproductive health survey of 2000showed that although the overall awareness of STDs and HIV/AIDS is high among the youth, significant misconceptions remained (e.g. “you can tell someone has an STD by looking at them”). According to the 2004 national survey of adolescents15 , 7% of males and 16% of females were forced into their first sexual experience, which increases to 8% and 25% in adolescents who have ever been coerced to have sex at some point in time19 . Another study performed in Dodowa, Greater Accra, showed that 27% of females in junior secondary school were forced to have sex11 and the youth reproductive health survey of 200012 indicate that 8% of males (with the highest proportion occurring in the Upper East) and 25% of females have ever been coerced to have sex. The relationship that adolescents have with sex among our study population showed that it is considered more an obligation than a right for both groups, and that many girls are unaware of being at risk of sexual violence. Many girls may fall victim to sexual violence without being able to recognize it: psychological coercion, bribery, failing to identify the right to say no to their partner or to change their minds, all contribute to the silent acceptance of violence. Because they are not prepared for sex, and may not have been able to use precautions, they are at risk of infection and pregnancy. The new Ghanaian law about domestic violence (Bill on Domestic Violence, 2007) does not seem to be considered, with just 5% of the female students considering law enforcement and police a way of preventing sexual abuse. Rather, they hold themselves responsible for sexual violence by “not behaving adequately to prevent it”. Acceptance of violence was also shown by Tweedie and Witte20 , who reported that 13% of males and 14% of females who ever had sex, consider it acceptable for a boyfriend to beat his girlfriend if she does not want to provide sex. On the other side of coercion is the fact that more than 2-thirds of all youth agreed that most girls do not mean it when they say no to sex, an attitude that can easily result into violence12 . We did not include questions related to the issue of female genital mutilation, which is a problem particularly prevalent in the North of the country. Specifically in the Bolgatanga district, the overall prevalence in second cycle girls is 6.3%, with girls not in school running almost four times the risk of being cut than their counterparts in school21 . During the FGD, the students manifested opposition to this practice and none of them presented any argument to support it. Conclusion The data presented in this report highlight the fact that the general awareness and fear of STIs and HIV/AIDS, and of unwanted pregnancies, does not directly translate into protective behavior. This is not a new finding; it confirms the gap between information acquisition and behavior modification16 . More in detail, this particular study showed that there is a relevant difference, concerning both knowledge and practices, between the Bolgatanga student population and the national average. The low familiarity with family planning methods and HIV/AIDS transmission, combined with minimal contraceptive use and frequentation of family planning centers, highlights the need of youth programs focused in this area. The poor infrastructures and the difficulties in accessing rural areas in the North of Ghana have led, in fact, to an uneven distribution of educational programs in the country. Additionally, although sex education should be theoretically covered at school, in practice few schools have a comprehensive program on family life education. Policy makers, perhaps for the fear of arousing religious opposition, tend to be ambivalent on issues concerning sex education: it is part of the school curricula but it is not effectively taught, thus pacifying the moral and religious critics22 . Learning from previous approaches in re-thinking sexual health education, it is more likely to influence adolescents’ behavior by providing detailed information on a wide range of issues, including reproductive health during various stages of development and targeting contextual factors specific to the youth8 . A more holistic, comprehensive program, which would take into account the delicate psychology of this phase of life, could provide fertile ground for discussion, counseling and participatory action. Such programs should become mandatory in schools, youth associations and clubs and should be accessible far before adolescents become sexually active, in order to dispel misconceptions about sex, and to address the risks of sexual violence. To be mostly effective, they should provide a non-judgmental, supportive, positive and thoughtstimulating environment. It is also critical for this type of intervention to be linked to existing services, like family planning centers, which should promote themselves as welcoming and youthfriendly centers. * Abortions is illegal in Ghana except in cases of rape and incest, or when the mother is at risk of harm or the fetus is at risk of serious disease or abnormality (Center for Reproductive Law and Policy (CRLP), Women of the World: Laws and Policies affecting Their Reproductive Lives, Anglophone Africa, New York: CRLP, 1997) Acknowledgements The research for this report was conducted under the Youth Harvest Foundation Ghana (YHFG) initiative project on Adolescent Sexual and Reproductive Health. Acknowledgments go to the entire team of Youth Harvest Foundation Ghana who provided all the necessary support to conduct the study. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09046f1.jpg] [rh09046t1a.jpg] [rh09046t1c.jpg] [rh09046t1b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}