 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 81-93 ORIGINAL RESEARCH ARTICLE Coping Strategies of Women Seeking Infertility Treatment in Southern Ghana Stratégies d’adaptation au problème de la stérilité chez les femmes qui recherchent un traitement au sud du GhanaErnestina S Donkor and Jane Sandall 1 School of Nursing, College of Health Sciences, University of Ghana, Legon, Accra, Ghana. Postal
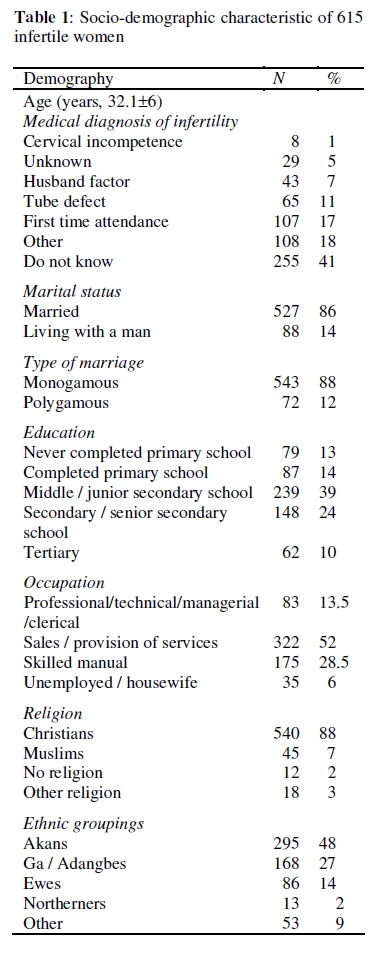
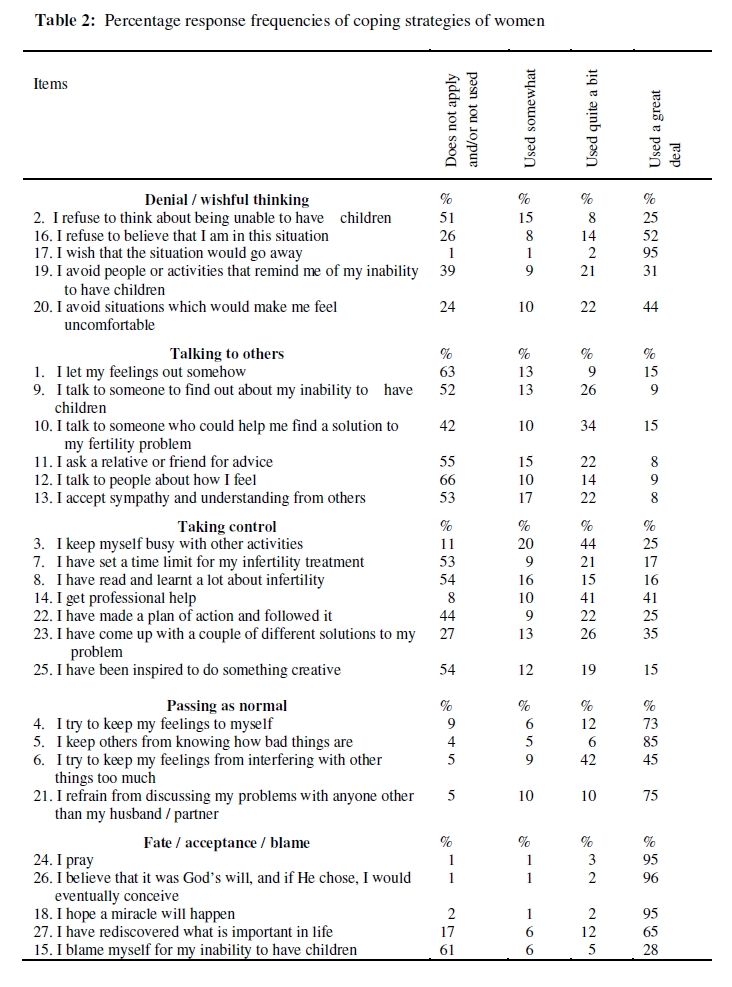
Address: PO Box DS2334, Dansoman, Accra, Ghana, West Africa Mobile: +233243114968 E-mail: tinadonkor@yahoo.co.uk; Code Number: rh09049 ABSTRACT Infertility is a health problem faced by an estimated 15% of women of childbearing age in Ghana. This study explores the coping strategies adopted by 615 women seeking infertility treatment in southern Ghana. Both closed and open-ended questions were used through a survey conducted using face-to-face interviews in three languages at three health sites – a hospital, a health centre and a private clinic. The findings suggest that the majority of the women preferred to keep issues of their fertility problems to themselves. The reason could be due to the associated stigma of infertility. Further, the majority of the women coped through drawing on their Christian faith. Others also coped through the support they received from their husbands, their occupation by way of achieving economic independence, and some avoided situations that reminded them of their infertility problem. The findings should have implications for health personnel as some strategies infertile women use may do more harm than good (Afr J Reprod Health 2009; 13[4]:81-93). RĖSUMĖ La stérilité est un problème auquel font face environ 15% des femmes en âge d’avoir des enfants au Ghana. Cette étude explore les stratégies adoptées par 615 femmes qui recherchent un traitement de la stérilité au sud du Ghana pour faire face au problème. On s’est servi des questions de nature limitées et illimitées à travers une enquête menée à l’aide des interviews face à face en trois langues dans trois établissements de santé : un hôpital, un centre médicosocial et une clinique privée, les résultats ont montré que la plupart des femmes préfèrent garder tout ce qui concerne leurs problèmes de la stérilité à elles-mêmes. La raison pourrait être à cause de la stigmatisation liée à la stérilité. De plus, la plupart des femmes se sont débrouillées en s’appuyant sur leur foi chrétienne. Les autres se sont débrouillées à travers le soutien de la part de leurs maris, à travers leurs occupations quand elle accomplissent l’indépendance économique et certaines d’entre elles ont évité des situations qui leur rappelaient leur problème de stérilité. Les résultats devraient avoir des implications pour les membres du personnel médical puisque certaines stratégies adoptées par les femmes stériles peuvent être plus nuisibles que bénéfiques (Afr J Reprod Health 2009; 13[4]:81-93). KEYWORDS: Coping strategies, Infertility treatment, Southern Ghana Introduction The Ghana Demographic Health Survey1 reports that involuntary childlessness is not common in Ghana, and currently married women with no live births are likely to be those in relationships with fertility problems. According to Larsen2 in Ghana the prevalence rates of primary and secondary infertility are 2% and 14% respectively. Research from other cultures3-5 indicates that women may experience pressures to procreate, especially from their in-laws. Women have reported being stressed due to their inability to have children6-9 . In other studies, women have expressed feeling of stigmatisation as a consequence of infertility.10-16 If infertility is associated with such problems, how do individuals faced with fertility problems cope? This paper sought to examine the coping strategies that a cross-section of women in Ghana utilised as they underwent infertility diagnosis and treatment. In a qualitative study conducted in the United States, Davis and Dearman17 found that women used a variety of coping strategies in dealing with the problems of infertility. These were: avoidance of reminders of infertility, regaining control, being the best, looking for hidden meaning, giving in to feelings, and sharing the burden. In Pakistan some women resorted to adoption in coping with infertility.18 However, from a cultural and social point of view, adoption remains an undesirable option in India19 . Another study also conducted in the United States, Stanton et al20 found that women who coped through escapeavoidance and through accepting responsibility for their infertility showed more distress, whereas women who sought more social support were less distressed. It was pointed out that drawing on their findings for the provision of support and professional intervention must be done with caution, the reason being that findings might lead to the conclusion that professionals should discourage avoidance and encourage support mobilisation. A study by Morrow et al21 gave credence to that of Stanton et al20 where avoidance strategy of coping in infertility was found to be associated with increased distress. A study conducted in Taiwan22 lends support to the findings of Morrow et al 21 and Stanton et al20 where infertile wives coping strategies of accepting responsibility and escape-avoidance were significantly and positively correlated with emotional disturbance. Boivin et al23 found that the most frequently used sources of support were talking with the spouse, family and friends, and using documentation on emotional aspects of infertility obtained through the clinic, newspapers or television programmes. It was pointed out that while infertility can be quite distressing for patients, external support from family and friends, new treatment opportunities could all mitigate emotional distress. Social support has been identified as playing a positive role in the experience of infertility.24 Research findings indicate that social support has buffering effect in the presence of stress25 . Social support is beneficial to recipients but the recipient should perceive it as such. If someone does not feel supported, then they will not experience the benefits of social support, even though other people might have considered the provider’s words or deeds to be supportive.26 This research study sought to ascertain the coping strategies adopted in Ghana by women encountering fertility problems. Through a literature search, no study was identified that had delineated coping strategies that were specific to individuals encountering fertility problems in Ghana. This study has the potential of assisting healthcare personnel or redirecting their focus in designing and implementing psychological support programmes for women faced with fertility problems. Through this it is hoped that the stigma, stresses and other adverse conditions associated with infertility would be reduced. Further, the findings of the study is intended to bring to the attention of policy makers the plight of infertile individuals so as to assist in the area of infertility prevention and its treatment, as the cost involved could be prohibitive. Definition of key terms Infertility – Inability to achieve conception despite the desire to do so at the time of data collection. Coping mechanism – Strategy adopted in managing the experience of infertility. Methods Research setting The research sites were three outpatients departments (OPD) of the gynaecology clinics of a hospital (n=324), healthcare centre (n=250) and a private clinic (n=41), all in Accra, Ghana. Ghana is located in south central coast of West African sub-region. It shares boundaries with Burkina Faso in the north, Togo in the east, Cote d’Ivoire in the west, and south by the Gulf of Guinea. It is one of the Anglophone countries surrounded by Francophone countries. Accra is the capital city of Ghana found in the southern portion. The hospital was selected because it was the largest and the most sophisticated in the country. It was a referral hospital that received patients from all parts of the country and other neighbouring countries. It attended to cases from both rural and urban areas. However, most of its clients were from the Greater Accra region, which was a cosmopolitan. The hospital had major specialties and accompanying services. It was the gynaecology unit of this hospital where part of the data of this study were collected. The second research site was a healthcare centre run by the Ministry of Health, Ghana. It was located in one of the sub-districts of Accra Metropolis. The inhabitants comprised people from various ethnic groups such as the Gas, Adangbes, Akans, Ewes, and Northerners. The third research site was a private clinic, which was also located in Accra. Although the clinic was community-based, it also catered for numerous businesses and organisations such as banks, insurance companies within its environs as well as the general population. Sample The sample involved 615 women attending gynaecology clinics at three sites at public and private settings – a hospital, a healthcare centre and a private clinic. They were women undergoing infertility diagnosis / treatment at OPD. Research Instrument The coping strategies adopted by women experiencing infertility were explored using closed and opened questions. The closed questions were constructed by selecting some questions considered appropriate for infertile woman in Ghana from the revised version of the Ways of Coping Checklist27 .This checklist is designed to assess an individual’s personal coping strategies in a stressful encounter. In this study, in addition to selecting some questions from the Ways of Coping Checklist, coping strategies adopted by infertile/childless women in managing the experience of their situation reviewed in the literature, were drawn on.17 Some of the questions were reworded to reflect the situation of infertility. In total 27 questions were obtained to measure how women managed their experiences of infertility. Examples of some of the questions were: ‘I refuse to think about being unable to have children’, ‘I talk to someone to find out about my inability to have children’, and ‘I avoid situations which would make me feel uncomfortable’. Respondents were asked to indicate on a 4-point Likert scale how often they used each particular coping strategy. Thus 0=does not apply/or not used; 1=used somewhat; 2=used quite a bit; and 3=used a great deal. In addition to these closed questions, there was an open question, which enquired what women did to cope with their situation. Ethical consideration Ethical approval of the research proposal was obtained from the Institutional Review Board of Noguchi Memorial Institute, University of Ghana. Agreement to the research was sought from the gynaecologists and Nursing Officers in charge of the gynaecology clinics. Data collection procedure At the research sites, gynaecology clinics were held throughout the week from Monday to Friday; and in the private clinic Saturdays and Sundays were included. Women were identified through their hospital registers and with the help of their gynaecologists. Most of the women were interviewed whilst waiting to see the doctors. Those who agreed to participate were invited into a room at the OPD. Informed consent was sought from them. They were interviewed face-to-face by the first author (ED) (in English, and two local languages – Akan or Ga) using the questionnaire. Data analysis On scoring, the percentage response frequencies of women on the close-ended coping strategy questions were calculated. Women’s infertility coping strategies were therefore explained in terms of their overall percentage response. With the open-ended question, the information gathered was translated and transcribed into the English language. All the transcriptions were read through carefully. The ideas that emerged were put into themes. Results Socio-demographic information Table 1 presents the socio-demographic details of 615 women encountering fertility problems. The mean age was 32.1 ± 6 years, and the range was from 17 to 49 years. When women were asked what their doctors say was the cause of their infertility, 41% indicated that they did not know what they said it was, 11% said it was due to tube defect / blockage and 7% said it was attributed to their husbands. Fourteen per cent of the women completed primary school whilst 10% attained tertiary level of education. With respect to occupation, 13.5% were involved in professional / managerial jobs and 6% were unemployed. The majority (88%) were Christians. Coping strategies In reporting, the percentage response of women on items of how they coped with their fertility problems were grouped together using our own grouping themes in terms of denial / wishful thinking, talking to others, taking control, passing as normal, and fate/acceptance/blame (Table 2). Denial / wishful thinking – Some of the women admitted that they had a fertility problem, whereas others denied it. For example, about 74% refused to believe that they were in such situations (item 16), where the majority of the women (98%) wished the situation would go away (item 17). When asked whether they avoided people or activities that reminded them of their inability to have children (item 19), 61% of the women responded in the affirmative. In addition, about 76% of the women indicated that they avoided situations that would make them feel uncomfortable (item 20). Talking to others – Talking to others about fertility problems was not a common strategy that the women used. In response to a question to ascertain whether women let their feelings out somehow in dealing with their fertility problem (item 1), 63% indicated that the question did not apply to them. Considering the percentage of responses of talking to someone to find out about their inability to have children (item 9) did not apply to 52% of women; and 42% of the women did not talk to someone who could help them find a solution to fertility problems (item 10). Further, 55% of them did not ask a relative or friend for advice (item 11), 66% did not talk to people about how they felt (item 12), and 53% did not accept sympathy and understanding from others (item 13). These findings suggest that a high percentage of the women preferred to keep issues of their infertility problems to themselves. Passing as normal – A higher percentage of women (91%) tried to keep their feelings to themselves (item 4), 96% of women kept others from knowing how bad things were (item 5), and 95% tried to keep their feelings from interfering with other things too much (item 6). In addition, most women (95%) refrained from discussing their problems with anyone other than their husbands / partners (item 21). Taking control – When women were asked if they kept themselves busy with other activities as a way of coping with infertility (item 3), most of them (89%) said that they used this strategy. To a question on whether women had set a time limit for their infertility treatment (item 7), more than half (53%) indicated that they had not. Women were asked whether they had read and learned much about infertility (item 8) as a way of coping with their infertility experiences. More than half of the women (54%) indicated that they did not use this strategy. It could be that many of the women in the present study did not have access to reading materials or information on infertility, or perhaps many could not read and write. A finding of this study showed that 13% of the women had never completed primary education and 14% had completed only primary education. Women were asked whether they had made a plan of action and followed it in relation to their infertility problem (item 22); 56% mentioned they had made such plans. About 73% of the women indicated that they had come up with a couple of different solutions to their infertility problem (item 23); and when women were asked whether they had been inspired to do something creative (item 25), 54% of them replied in the negative. Despite their reluctance to talk to people about their fertility problem, they all sought professional help. This may suggest that women felt more comfortable to share their infertility issues or seek help from health professionals; doing so could serve as a way of taking control of their situation. Fate / acceptance / blame – In coping with their infertility problems, the majority of women (99%) prayed (item 24). Findings show that 99% of women believed it was God’s will and if He chose they would eventually conceive (item 26); and 98% hoped a miracle would happen (item 18). This finding could mean that women depended on their religion to cope with their situation. Is this common in other studies or more so in Ghana? About 83% of the women also mentioned that they had rediscovered what is important in life (item 27). The majority of the women (61%) did not blame themselves for their fertility problems (item 15). To an open question that asked women how they coped with their situation, the majority of the women relied on their religious beliefs. Thus, this supports the finding of the closed questions on coping strategies in which the majority of the women depended on their religious faith. Below were some of the statements from the women: ‘I pray to God because He alone can provide’ All these responses were from women who belonged to the Christian faith. No responses from other faiths were received. This might be due to the fact that the majority of the women (88%) were Christians. Some of the women reported that they were able to cope through the support they received from their husbands. The following were some of their responses: ‘My husband has been supportive’ Another strategy the women utilised in coping with their fertility problem was their awareness that they were not the only ones experiencing infertility. The following were some of the words of the women: ‘I console myself that I am not alone in this situation, other women also don’t have children’ Women comparing themselves to others who are in a similar situation could thereby reduce their sense of isolation. Other women engaged themselves in activities that took their minds off their infertility problems. Some of the responses were the following: ‘I keep myself busy with my job and get consolation from it’ Some of the women were able to cope by increasing the space between themselves and their problems of infertility. Some of the women stated: ‘I avoid situations which would make me feel uncomfortable’ Discussion The main aim of this study was to investigate the coping strategies of women in the experience of infertility. Both closed and open-ended questions were used. The findings suggest that the majority of the women in the sample preferred to keep information about their infertility to themselves and not to disclose to other people. In a study carried out in South Africa, several of the women did not want to speak to others about their involuntary childlessness. Davis & Dearman17 found that while many women found talking to others about their infertility proved helpful, other women did not discuss being infertile with anyone other than their spouses. This helped them to increase the space between themselves and their fertility problems. Remennick29 also found that women in Israel were concerned about their reputation after disclosure of their infertility. Miall’s10-11 study of women in the United States also found that most women in that setting reported that they were concerned that an awareness of problems with fertility would cause others to see them in a new and damaging light; it lessened the woman in the eyes of others. In managing information about themselves, women hesitated in telling others about their fertility problem, and some did not reveal the exact details of their condition11 .This appears to be a common strategy among those with stigmatising conditions. Goffman30 mentioned that the discreditable person has a problem of concealment and disclosure of information about himself / herself. If the fertility problem is not known, it becomes a ‘discreditable condition’ and individuals might tend to control information about their failing situation. By not disclosing what was stigmatising about oneself, the person can ‘pass’ as ‘normal’ as the failing situation is not readily visible.30 Further, since infertility could be seen as a ‘master status’ that overshadows the accomplishments of individuals10 , women preferred to keep their infertility problems to themselves. The findings showed that more than one-third (37%) of the women in coping with their fertility problem openly expressed their emotions. This finding ties in with that of Davis & Dearman.17 In their study in the United States many of the women reported having given in to their intense feelings of sadness and frustration with being unable to conceive. They mentioned that they had wept many times due to their infertility. By giving in to their emotions and crying, they felt better equipped to deal with their unmet desire. More than half of the women in coping with their infertility problems reported that they had been thinking about their inability to have children. This finding relates to the finding of Hjelmstedt et al31 where women acknowledged thinking about their infertility problem. However, some of the women in the present study reported keeping themselves busy with other activities that took their minds off their infertility problem, and some threw themselves into their occupation thereby distracting themselves. This finding ties in with that of Bhatti et al18 and Davis & Dearman17 . More than half (54%) of the women in this sample did not engage in reading and learning much about infertility as a means of managing their infertility experiences. The reason could be that some of these women were either not formally educated or were less educated as the finding of this study has shown. Woollett ,32 in a study carried out in the United Kingdom, found that in coping with infertility, infertile individuals sought medical help and became knowledgeable about infertility. In the study of Davis & Dearman17 , the majority of women reported regaining control of their infertility through reading and learning as much as possible on the subject to gain knowledge about the various causes and treatment of infertility. The finding of Parry33 of a study carried out in the United States is of a similar nature, in which women reported that they read and learned about their infertility; and that enabled them to play an active role in the decisionmaking process and influenced the medical processes affecting their lives. Thus the knowledge they had concerning their situation empowered them to make informed decisions and choices. The majority of women in the sample used their religious faith as a means of coping with their fertility problems (88% of the participants were Christians). For example, some of the women mentioned that they hoped that the Lord would answer their prayers at the appropriate time. Unisa15 also found in India that many women relied on their strong religious beliefs and varied religious practices in addressing their fertility problems. In the study of Davis & Dearman17 some of the women believed that their infertility was God’s will and if He chose they would eventually conceive. In this, they were looking for hidden reasons for their infertility. Similarly, in a study in South Africa,all the groups of women expressed religious belief as an important source of support. Studies in other areas of life situations such as mental illness34 , medical illness35 , and stressful situations36 have reported on the use of religious coping strategies. However, in secular societies religious beliefs may not be so important. Some of the women in this Ghana sample also reported coping through the support they received from their husbands. This finding is consistent with a further finding from South Africa28 where some of the women described their husbands as supportive, understanding, and trustworthy, and they saw them as friends. However, some women were concerned that the good relationship they were enjoying with their husbands might change if the fertility problem persisted. In other studies4 , infertile women have expressed similar sentiments in feeling supported by their partners. Boivin et al23 found that talking with one’s spouse served as a source of support. In the study of Lee et al37 in Taiwan, infertile women coped with fertility problems through sharing feelings related to infertility with their husbands. It is important that infertile women receive support from their spouses as lack of support has been found to be a key source of anxiety and depression.5 In a study in which perceptions of provided and received emotional support and disregard were examined among infertile couples, both significantly contributed to the quality of marital life.26 Some of the women also coped through the avoidance of situations that reminded them of their inability to have children. Blenner38 found that infertile women felt inadequate in the presence of pregnant women and babies; hence they tried to avoid pregnant women and babies. In research studies conducted in the United States, the use of avoidance as a coping strategy was found to be associated with increase in distress among individuals encountering fertility problems.20-21 Further, in a study carried out in Taiwan, the coping strategy of avoidance was found to be positively and significantly correlated with emotional disturbance,22 but this was not investigated in the current study. Conclusion When the women were asked about the strategies that they used to cope with the experience of infertility, they gave a range of answers. Avoidance of stigma was attempted by keeping information about their infertility to themselves, and some women avoided situations that reminded them of their infertility. Some women depended on their religious faith, some found comfort in their husbands’ support, and others became absorbed in their occupation or profession. Infertile women could be assisted to build on effective coping strategies. The findings of this study could be useful in designing and implementing psychological programmes for infertile women. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09049t2.jpg] [rh09049t1.jpg] |
| |||||||||

{kind=link}
{kind=link}