 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
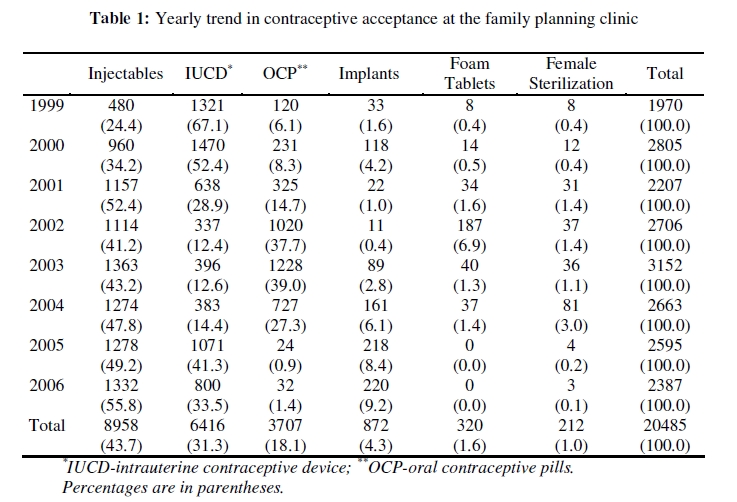
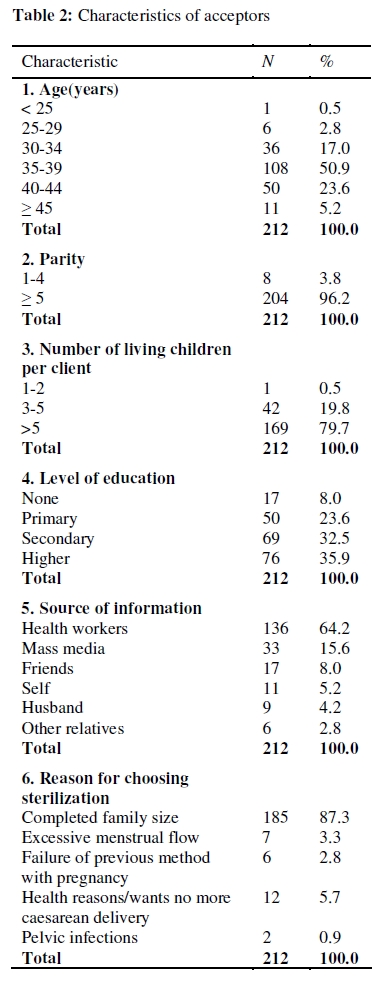
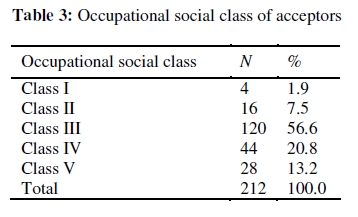
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 105-111 ORIGINAL RESEARCH ARTICLE Sterilization by Minilaparotomy in South-Eastern Nigeria Stérilisation à travers la minilaparotomie au sud-est du Nigéria.Eric E Nwogu-Ikojo*, Hyginus U Ezegwui and Sylvester O Nweze Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Enugu, Nigeria. Code Number: rh09051 ABSTRACT The study aimed to assess the trend in acceptance and characteristics of acceptors of female sterilization between January 1999 and December 2006 at the University of Nigeria Teaching Hospital, Enugu, South-Eastern Nigeria. There were a total of 20,485 new clients, with 212 (1.0%) accepting sterilization between January 1999 and December 2006. There was an initial rise in acceptance from 0.4% in 1999 to 3.0% in 2004, then a decline. 108 (50.9%) were between 35-39 years. 169(79.7%) had more than five living children. 69 (32.5%) and 76 (35.9%) had secondary and higher education respectively. Health workers were the main source of information. Completed family size was the reason for choosing sterilization in 185 clients (87.3%). 120 (56.6%) were in occupational social class 3. 106 (50.0%) did not practice any form of family planning prior to the procedure. 184 (86.8%) had interval sterilization and the rest (13.2%) postpartum. Acceptance of tubal sterilization is still low in our community (Afr J Reprod Health 2009; 13[4]:105-111). RĖSUMĖ L’étude avait pour objectif d’évaluer la tendance de l’acceptation et les caractéristiques des accepteuses de la stérilisation féminine entre janvier 1999 et décembre 2006 au Centre Hospitalier Universitaire d’Enugu, au sud-est du Nigéria. Il y avait au total 20,485 nouvelles clientes dont 212 (1,0%) ont accepté la stérilisation entre janvier 1999 et décembre 2006. il y avait une hausse initiale dans l’acceptation de 0,4% en 1999 jusqu'à 3,0% en 2004, puis un déclin. 108 (50,9%) étaient âgés d’entre 35 et 39 ans. 169 (79,7%) avaient plus de cinq enfants encore vivants. 69 (32,5%) et 76 (35,9%) ont fait des études secondaires et supérieures respectivement. Les membres du personnel soignant ont été la source principale d’information. Ayant eu le nombre d’enfants désiré constituait la raison pour laquelle 185 clients (87,3%) ont choisi la stérilisation. 120 (56,6%) appartenaient à la classe sociale professionnelle 3, 106 (50,0%) n’avaient pratique aucune forme de la planification familiale avant la procédure. 184 (86,8) ont eu une stérilisation par intervalles et le reste (13,2%) avaient le post-partum. L’acceptation de la stérilisation tubaire est encore faible dans notre communauté (Afr J Reprod Health 2009; 13[4]: 105-111). KEYWORDS: Female sterilization, Minilaparotomy, Tubal ligation Introduction Female sterilization is the most common form of modern contraception used all over the world. The safety of the procedures, simplicity, convenience, and effectiveness contributed to the increased acceptance of sterilization in the last three decades globally1 . However, it has not been widely accepted in sub-Saharan Africa as in other parts of the world.2 Nigeria is the most populous black nation in the world with an estimated population of over 140 million people.3 The Nigeria Demographic and Health Survey (NDHS) 20034 showed Crude Birth Rate (CBR) was 41.9 per 1000 population; and that Total Fertility Rate (TFR) was 5.7 per woman. It also showed that overall 12% of all women used a method of contraception, with only 8.1% of married women using a modern method. Only 0.2% of those surveyed accepted female sterilization. The level of education of the population, age, parity, and influence of religion strongly influence the level of acceptance of voluntary surgical contraception. Female sterilization is usually carried out by tubal ligation using the Pomeroy’s method in our centre. It is a one-time procedure that can be carried out either as an outpatient or inpatient basis (usually post partum or during caesarean section). It is usually considered a permanent method of contraception. The procedure is usually done by minilaparotomy under local anaesthesia for postpartum (usually within 48 hours after delivery) and interval (done six weeks or more after delivery) procedures. This objective of this study is to assess the uptake of female sterilization by minilaparotomy and acceptor characteristics at the University of Nigeria Teaching Hospital, Enugu, a major centre offering Family Planning and reproductive health services in South-East Nigeria, and to examine the changes in trend of utilization. Methods The case-records of clients who accepted female sterilization at the University of Nigeria Teaching Hospital, Enugu, Southeast Nigeria, between January 1999 and December 2006 were retrieved and reviewed. The zone of Southeast Nigeria is mostly made up of the Ibo ethnic group. The age, parity, religion, occupation, numbers of living children, level of education were extracted. In addition, occupational social class, previous contraceptive practices, source of information about contraception, time interval between delivery and sterilization. Duration of sterilization, type of anaesthesia, and complications of the procedure were also studied to assess safety and quality of care. Occupational social class was classified as: I. Professionals (e.g. doctors, lawyers, senior business executives); II. Other professionals (e.g. lecturers, teachers, nurses); III. Skilled non-manual workers (e.g. secretarial and clerical staff, skilled technicians); IV. Semi-skilled workers (e.g. machine operators, farm workers); and V. Unskilled workers (e.g. labourers, cleaners, domestic workers, petty traders). Female sterilization is either a postpartum or an interval procedure. Postpartum procedures are usually done within 48 hours after delivery. Results There were 20,485 new contraceptive acceptors during the study period. Two hundred and twelve of them choose female sterilization giving an acceptance of 1.0%. Table 1 shows the trend in acceptance of various methods during the study period. Table 2 shows the various characteristics of the acceptors. All the women had at least one living son, with only one woman having a minimum of two living children. All acceptors were Christians. Table 3 shows the occupational social class of the acceptors. The last contraceptive method used by the acceptors was intrauterine contraceptive device (IUCD) in 40 women (18.9%), male condom in 21 women (9.9%), rhythm method/periodic abstinence in 15 women (7.1%), injectables in 11 women (5.2%), withdrawal method in 9 women (4.2%), oral contraceptive pills in 8 women (3.8%), implants in 2 women (0.9%). 106 women (50.0%) did not practice any form of family planning before the procedure. One hundred and eighty four women (86.8%) had interval sterilization and 28 women (13.2%) had postpartum sterilization. The procedure lasted less than 30 minutes in 141 women (66.5%), and between 30 and 60 minutes in 71 women (33.5%). None lasted more than 60 minutes. Local anaesthesia was used in 209 women (98.6%) and local anaesthesia with sedation in three women (1.4%). There were no post-operative complications. Two women (0.9%) requested for reversal and there was no record of failure. Discussion During the study period, there were 20,485 clients. Injectables were the most widely used method (43.7%), followed by intrauterine contraceptive devices (31.3%) and oral contraceptive pills (18.1%). Other methods were much less popular. Injectables showed a sustained rise in uptake from 24.4% to 55.8% during the study period, except for a dip from 52.4% to 41.2% from 2001 to 2002. This may be because this method can be used covertly without the partner being aware5 and only requires a single injection shot every 2-3 months. Uptake of intrauterine contraceptive devices dropped from 67.1% to 33.5% at the end of the study period. The need for insertion by a health worker intravaginally and follow ups also requiring vaginal examinations compared to the injectables may also have affected uptake. The oral contraceptive pills showed increased uptake till 2003 and then a steep decline in uptake. While the reason for the steep decline in uptake are not immediately clear, the need to remember to take tablets daily and the possibility of anyone seeing the drug pack knowing you are on the pill may have been contributory. The need for a minor surgical procedure by a doctor may also have affected uptake of implants, as clients may be reluctant to undergo the procedure. The period 2002 to 2004 witnessed a general increase in number of people accepting all contraceptive methods. During this period there was a donor funded project that subsidized services, thus cost may be an important barrier for women to access services. Acceptance of tubal sterilization remains low within our practice environment in southeast Nigeria. There was an initial rise in acceptance from 0.4% in 1999 to 3.0% in 2004, then a decline. The acceptance of 1.0% in this study was a decline in the 8.0% found in an earlier study from this centre. 6 Another study from Nnewi, southeast Nigeria had found an acceptance of 2.5%.7 This is in contrast to the rising trend in Latin America, 8 and studies from other parts of Nigeria showing a high acceptance rate or increasing acceptance. 9-11 Omu and Akagbosu 12,13 found that the desire for more children, fear of opposition, reincarnation, husband’s objection and aversion to surgery made Nigerian women choose reversible methods. Inadequate facilities, shortage of trained personnel, high infant and childhood mortality, cultural and religious factors are other factors responsible for low acceptance of female sterilization. 14,15 Majority of our clients (50.9%) were in the 35 to 39 year age group and majority were found to have been grandmultiparous women with a large family size of five or more children. These findings are similar to findings of similar studies.8,11,12,15 This shows the high premium placed on children as they are seen as a source of support in old age. Thus, women who seek sterilization are likely to be those who have completed their families. Most of the women had either a secondary (32.5%) or higher education (35.9%), unlike the findings from Jos, North central Nigeria, where an overwhelming majority of the women (74.87%) had no education at all. 15 Leite et al 8 in a cross-national study of four Latin American countries (Brazil, Columbia, the Dominican Republic, and Peru) found acceptors of female sterilization to be more educated women. Thus, sterilization in southeast Nigeria is not skewed towards less educated women. Health workers are efficient sources of information and were the main source of information about the procedure. Thus, utilization of health workers in community health education and mobilization programs will greatly improve acceptance as they have the knowledge to not only provide accurate information, but also clear any myths and fears about the procedure. The use of the media as a tool to reach a larger population should be exploited. Innovative messages explaining the procedure and addressing long held myths within the society about sterilization may boost uptake. Female sterilization is usually chosen by those who have completed their family size. Similar to findings from other studies. 8,15,16 Thus, sterilization provides these women who have had the desired number of children a safe and effective form of long term contraception that is not dependent on coitus. Health reasons were also cited as the next most important reason especially the desire not to have any more caesarean sections. Women in occupational social class 3 (56.6%) formed the bulk of the acceptors followed by those in occupational social class 4 (20.8%) . It may be that women in the highest occupational social class may have been exposed to family planning earlier and may have been using satisfactorily other reversible long-term methods. They may also prefer to access services in specialist private clinics rather than in public health institutions. Those in the lower occupational social class are likely to have had less access to family planning services. They are also likely to find the services in public health institutions more affordable. Half of the women (50.0%) did not practice any form of family planning prior to the procedure showing the huge unmet need for family planning services in our community. Every opportunity to enlighten the public about available family planning services and its benefit to the family should be exploited. The political will to fund services and bring the facilities closer to the communities is also essential. Ignorance, low level of education, cultural and religious beliefs, as well as unavailability of materials, supplies, and trained manpower are also barriers to increased acceptance of modern contraceptive methods. 9,13 Most women (86.8%) had interval sterilization under local anaesthesia, and the procedure lasted less than 30 minutes in majority of the women (66.5%). This is similar to other studies. 8,9,10,15 No complications were recorded. Thus, the procedure is simple and safe to perform with little risk of complications. In this study, only two clients requested for reversal, citing religious reasons. The importance of counselling the patients properly before the procedure cannot be over-emphasized with the permanent nature of the procedure stressed. They should be counselled on all contraceptive options available to them, to enable them choose a method that is appropriate to their family planning needs. 17 This is a facility based study and may not capture all the segments of the population. Thus, a population survey may be needed to further explore reasons for low uptake of female sterilization in our family planning clinics in the southeast region of Nigeria. Increased advocacy and public education will help inform the target population about the service and where to access it. Integrating family planning and reproductive health services into the primary health care system and building capacity by training of more personnel in the procedure especially using minilaparotomy with local anaesthesia will bring the service closer to the people at the community level, as services are presently concentrated in the major urban centres. In conclusion, the acceptance of female sterilization by women counselled for family planning at our family planning clinic is low, with a downward trend in recent years. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09051t3.jpg] [rh09051t2.jpg] [rh09051t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}