 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
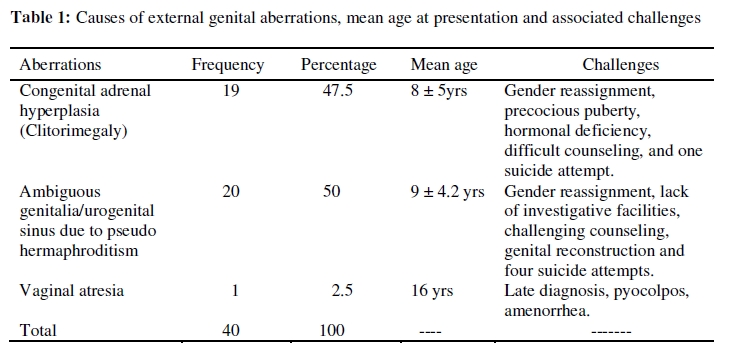
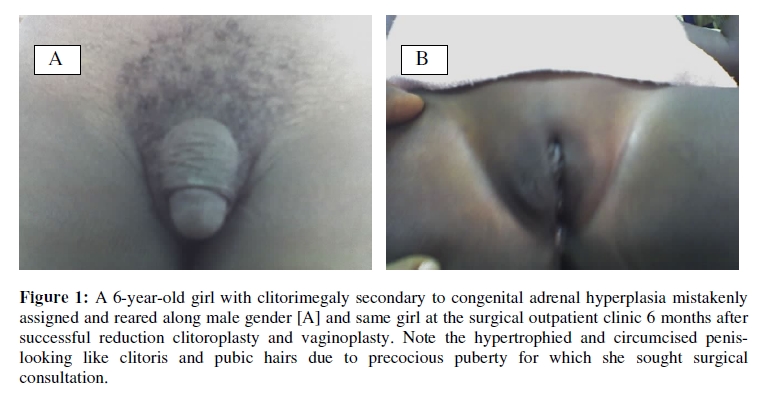
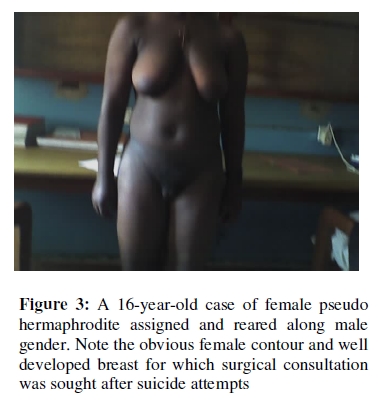
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 129-136 ORIGINAL RESEARCH ARTICLE Female Children with Ambiguous Genitalia in Awareness-Poor Subregion Les filles qui ont des organes génitaux ambigus dans une sous-région peu sensibiliséeOsarumwense D Osifo1* and Taiwo I Amusan1 Pediatric Surgery Unit, Department of Surgery, University of Benin Teaching Hospital, Benin City, Nigeria Code Number: rh09053 ABSTRACT Congenital aberrations of female children’s external genitalia are common worldwide with varied mode of presentation especially in regions with poor awareness. This prospective experience between July 2004 and June 2008 at two Nigerian healthcare facilities is on the mode of presentation and challenges of management of female children with ambiguous genitalia. Congenital adrenal hyperplasia (CAH) 19 (47.5%), female pseudohermaphroditism 20 (50%) and vaginal atresia 1 (2.5%) manifested as aberrations of external genitalia of 40 female children who presented between the ages of 3 months and 16 years (average 9 years). Cultural influence, lack of awareness, inadequate examination of external genitalia at birth and lack of diagnostic facilities resulted in late presentation and diagnosis with all the cases of CAH and pseudohermaphroditism raised as males. Five cases who developed female secondary sexual characteristics at puberty attempted suicide before presentation. Gender reassignment and feminizing genitoplasty were major challenges, but outcomes were encouraging (Afr J Reprod Health 2009; 13[4]:129-136). RĖSUMĖ Les aberrations congénitales des organes génitaux externes chez les filles sont communes partout dans le monde, ayant des divers modes de présentation dans les régions qui sont peu sensibilisées. Cette expérience prospective entre juillet 2004 et juin 2008 dans deux établissements de santé est basée sur le mode de présentation et les défis du traitement des filles qui ont des organes génitaux ambigus. L’hyperplasie surrénale congénitale (HSC) 19 (47,5%) le pseudohermaphrodisme 20 (50%) et l’atrésie vaginale 1 (2,5%) se sont manifestées comme des aberrations des organes génitaux externes des 40 filles qui se sont présentées entre les ages de 3 mois et 16 ans (âge moyen – 9 ans). L’influence culturelle, le manque de conscience, l’insuffisance de l’examen des organes génitaux à la naissance et le manque des établissements d’analyses médicales ont abouti à la présentation et au diagnostic tardifs, ce qui fait que tous les cas de HSC et du pseudohermaphrodisme ont été élevé comme des mâles. Cinq cas qui ont développé des caractéristiques sexuelles secondaires féminines ayant atteint l’âge de puberté ont tenté de se suicider avant de se présenter. La réattribution de sexes et la génioplastie féminisante ont été des défis principaux, mais les résultats ont été encouragements (Afr J Reprod Health 2009; 13[4]: 129-136). KEYWORDS: Congenital aberration, Ambiguous genitalia, Female children Introduction Congenital aberration of external genitalia is common worldwide. Many congenital anomalies following genetic, enzymatic and chromosomal defects may manifest with aberration of external genitalia 1,2 . Although the lesions are benign, early detection is important so as to assign the correct gender at birth and prevent avoidable complications which may occur later in life. In regions where awareness is high and adequate facilities are available, the lesions may be diagnosed in-utero or at birth which make early treatment possible without sequel3-6 . In sub-Saharan Africa, however, late presentation of female patients with aberrations of external genitalia is very common due mainly to lack of awareness 7,8 . In many cases of ambiguous genitalia due to intersex disorder, affected female children are assigned and reared along male gender line even when there is obvious aberration of the ‘penis’ (phallus). This is influenced by the culture which prefers male to female children8 . Treatment of such aberrations of external genitalia after the wrong gender has been assigned and gender identity has occurred can be very challenging. Surgical correction may be possible but the psychological effects may be devastating due to social stigmatization and non acceptance by the community especially in an African setting with communal settlement1,2,7-9 . Even though children with congenital aberration of external genitalia present late and management of the lesions is a major challenge, not many publications have been done on it to increase awareness in this setting 7,8,10 . This is a 4-year prospective experience with the etiology, mode of presentation, challenges and outcome of management of female children with ambiguous genitalia at two healthcare facilities in Nigeria presented to increase awareness. Patients and Methods This 4-year prospective study is on the mode of presentation and challenges of management of female children with ambiguous genitalia who presented at the University of Benin Teaching Hospital, Benin City, and Leadeks Medical Centre both in Edo state, Nigeria, between July 2004 and June 2008. ‘Ambiguous genitalia’ refers to intersex disorders that manifest with aberration of external genitalia in female children. Diagnosis and sex determination were made using a combination of clinical, radiological and laboratory investigations. The age, gender assigned before presentation, mode of presentation, family history of similar lesions, findings on examination and investigations, presence of associated congenital anomaly, treatments, challenges and outcomes were collated on structured form. Also, available parents/caregivers were interviewed to know their socioeconomic status, place of residence and level of education. Thereafter, all the affected children and their parents/caregivers were recruited for counseling by the social workers. Psychologists, psychiatrists, pastors, prophets, priests and traditional rulers were involved in counseling difficult cases. Other causes of aberration like the two cases of extrophy of the bladder which were obvious and diagnosed at birth were excluded from the study. The data obtained is presented as count, frequency and percentage in tables and figures with continuous data expressed as mean/standard deviation. Results A total of 40 female children were seen with congenital aberrations of external genitalia. They were aged at presentation between 3 months and 16 years (average 9 years). As shown in Table 1, common causes were congenital adrenal hyperplasia (CAH) manifesting mainly with clitorimegaly in 19 (47.5%) children (Figure 1) and female pseudohermaphroditism manifesting with ambiguous genitalia in 20 (50%), Figure 2 and Figure 3. A rare cause was vaginal atresia in 1 (1.1%) patient. The majority of parents/caregivers 21 (52.5%) resided in rural areas with their children/wards, 12 (30%) were of middle class in suburban communities while 7 (17.5%) were elite city dwellers. The socioeconomic and educational status did not influence the mode of presentation. Antenatal care and delivery of these babies were by traditional birth attendants 17 (42.5%), paramedical healthcare providers 10 (25%), nursing midwifes 8 (20%) and doctors 5 (12.5%). Poor knowledge of female genital anatomy by 27 (67.5%) birth attendants and failure to carry out thorough examination of the genitalia at birth by 13 (32.5%) contributed to late presentation. Consequently, no case was diagnosed at birth or during neonatal period. Surgical consultations were sought following accidental discovery while examining other lesions in eight children by health workers, precocious puberty in six and development of female secondary sexual characteristics at puberty by five (Figure 3). Those with clitorimegaly due to congenital adrenal hyperplasia were mistakenly raised as males (Figure 1a). Despite obvious abnormality of external genitalia of the 20 female pseudohermaphrodites, wrong gender was assigned. Swollen labioscrotal fold containing ovotestis (Figure 2) mistaken for hernia led to surgical consultation by 14 children. The girl with vaginal atresia was assigned the correct gender but presented due to cyclical lower abdominal pain, increasing suprapubic mass and failure to achieve menarche at age 16 years. Congenital aberration of external genitalia presented diagnostic challenge in these centres owing to nonavailability of diagnostic facilities. Although Giemsa banding karyotype, pelvic ultrasound scan, sinogram and CT scan were helpful, 5 children with CAH and 2 true hermaphrodites required minilaparotomy to visualize the internal genitalia as the results of these investigations were not conclusive. Treatment of CAH included reduction clitoroplasty, Hendren’s vaginoplasty (Figure 1b) and hormone replacement plus the addition of antihypertensive drugs in two children. Surgical treatment of pseudo hermaphrodites included biopsy of ovotestis, correction of external genitalia along the gender of rearing and excision of those of opposite sex. Counseling of patients, parents/caregivers and gender reassignment were most challenging, which resulted in 13 (32.5%) families relocating to other communities. In addition, a girl with CAH and 4 cases of female pseudo hermaphroditism who presented at puberty (Figure 3) attempted suicide due to social stigmatization and lack of acceptance by their communities. The services of pastors, priests, traditional rulers, psychiatrists and psychologists were employed in handling these cases. The one to three years follow-up is yet to determine the sexual and fertility profiles of these cases. Discussion This study recorded a high number of female children with ambiguous genitalia who presented between 3 months and 16 years as neither intrauterine nor neonatal diagnosis were made7 . Although there are marked differences between male and female external genitalia, careful examination may be required to detect some subtle aberrations especially in neonates. In developed countries with high level of awareness, diagnosis inutero or at birth is feasible. This makes early gender assignment and corrective surgery possible before the age of sex identity3-6 . In subregions with poor level of awareness such as Nigeria, many female children with even major aberrations of external genitalia are missed at birth with affected children reared along wrong gender line as seen in this study. This resulted in the challenges of gender reassignment, genitoplasty and the psychological effects of the lesions that were also recorded in similar studies7,8.11.12 . In a survey on secondary school students in this subregion, earlier researchers10 recoded a high prevalence rate (6.8%) of congenital aberrations of external genitalia which were undiscovered either by birth attendants or parents/caregivers. Such affected children would never have sought medical attention unless there was complication or following sexual dysfunction after marriage. This tallied with findings in this study in which the patients presented following accidental discovery, precocious puberty or appearance of female secondary sexual characteristics at puberty. Although the majority of affected children were delivered by birth attendants with poor training and poor knowledge of anatomy of female external genitalia, the numbers undiagnosed at birth by orthodox trained personnel are equally alarming. Many cases in this series were discovered during examination of other pathologies by health workers as also reported in other studies7,8 . Children with aberration who do not developed complications, examined by health workers or whose parents/ caregivers are poor rural dwellers often do not seek medical attention8 . This perhaps explains while only few cases of intersex disorders were seen in this series unlike what was reported in other similar studies in more advanced regions where various types of intersex disorders were encountered1,2,13 . Patients with other forms of intersex disorders may not have presented during the period of this study. This shows the importance of publications and public enlightenment campaign on this lesion in this subregion. Moreover, an average African irrespective of educational status, is subconsciously and remotely influenced by the traditional beliefs which prefer male to female children14,15 . Earlier authors8,14,15 reported that families with many female children and those who wanted a male child as firstborn and head of the family would raise any case of ambiguous genitalia as male. It would not be surprising that many affected female children in this series may have been knowingly raised as male despite obvious aberration of the external genitalia or ‘penis’. Sex determination was very challenging in these centres unlike in developed countries3-6 . This is because in-utero or post natal determination requires highly trained personnel and sophisticated facilities which are not readily available in many developing countries. In view of this, many affected children required mini-laparotomy to directly visualize internal genitalia as Giemsa banding karyotyping was not conclusive and there were no facilities for spectral karyotyping, chromatin mass, Y-fluorescence studies and sophisticated imaging facilities. This approach to confirming or determining the gender to assign in patients raised along wrong gender was also adopted and found helpful by earlier authors in similar low resource regions7,8,16 . Internal genitalia are normal in many cases of intersex disorders such as congenital adrenal hyperplasia. The direct visualization of internal genitalia in other cases is important to ascertain their normalcy for the purpose of sexual functions and reproduction 12,17,18 . Although post repair sexual functions and genital sensitivity as done in other studies12,17-19 were not feasible, anatomical correction of all cases of aberrations were achieved in this series. No immediate post operative complication and/or during follow-up has been recorded. On the other, the psychological effects on the patients, parents/caregivers which was similar to the experiences of other authors1,8,11,20 was much. This resulted in many families relocating to other communities with their children as they could not cope with the social stigmatization and poor acceptance by their communities. Consequently, five cases of suicide attempts were recorded among patients who presented at puberty. Adequate counselling by pastors, priests, traditional rulers, psychiatrists and psychologists were rewarding as no true suicide was recorded after presentation and treatment. Many affected families and children were successfully reintegrated back in their communities during follow-up. Conclusion Although female children with ambiguous genitalia were many, none was diagnosed in-utero or at birth with the majority of cases diagnosed following accidental discovery, precocious puberty or appearance of secondary sexual characteristics at puberty. Cultural influence, lack of awareness, inadequate examination of external genitalia at birth and lack of facilities required for intrauterine and neonatal screening resulted in late diagnosis. Genitoplasty, gender reassignment and counselling were very challenging with five cases of suicide attempts. Public enlightenment program, campaign and advocacy which will result in thorough examination of external genitalia of babies at birth, and provision of basic facilities for diagnosis and treatment are advocated. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09053f1.jpg] [rh09053f2.jpg] [rh09053t1.jpg] [rh09053f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}