 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
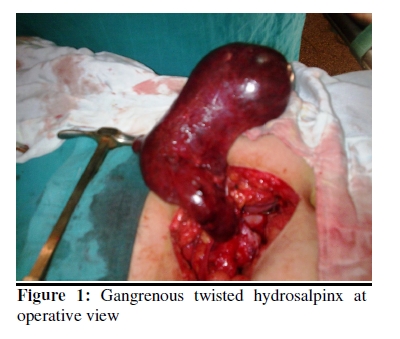
African Journal of Reproductive Health, Vol. 13, No. 3, Dec, 2009, pp. 147-150 CASE REPORT Uncommon Cause of Acute Pelvic Pain: Isolated Torsion of Hydrosalpinx La cause peu fréquente de la douleur pelvienne aiguë : la torsion de l’hydrosalpinx isolée. Ait Benkaddour Y1*, Bennani R1, Aboulfalah A1 and Abbassi H1 Department of Obstetrics and gynecology, University Hospital of Marrakesh, Cadi Ayyad University, Marrakesh, Morrocco. Code Number: rh09055 ABSTRACT Isolated torsion of hydrosalpinx is a rare cause of acute pelvic pain. Pre-operative diagnosis is very difficult because of non specific clinical presentation. Definitive diagnosis is always made at surgical exploration performed for suspected adnexal torsion and salpingectomy is performed in the majority of cases. A 34-year-old woman was admitted for acute pelvic pain with nausea and vomiting. Vaginal examination revealed a right adnexal tender mass and ultrasound revealed a well circumscribed right adnexal cystic mass. Surgical exploration has revealed torsion of a right hydrosalpinx and right salpingectomy was performed. Differential diagnosis between adnexal and tubal torsion is very difficult, however both should be managed by rapid surgical exploration which an allow precocious diagnosis and conservative treatment (Afr J Reprod Health 2009; 13[4]:147-150). RĖSUMĖ La torsion de l’hydrosalpinx isolée est un cause rare de la douleur pelvienne aiguë. Le diagnostic préchirurgical est très difficile à cause d’une absence d’une présentation clinique spécifique. On fait un diagnostic définitif pendant l’exploration chirurgicale pratiquée pour détecter une torsion annexielle et pour la majorité des cas c’est la salpingectomie qui est pratiquée. Une femme âgée de 34 ans a été admise à l’hôpital à cause d’une douleur pelvienne aiguë accompagnée de la nausée et du vomissement. Un examen vaginal a révèle une masse sensible d’annexiel droit et l’ultrason a révélé une masse Kystique de l’annexiel droit bien circonscrite. Une exploration chirurgicale a révèle une torsion de l’hydrosalpinx droit et nous avons pratiqué la salpingectonie. Le diagnostic différentiel entre l’annexiel et la torsion tubaire est très difficile, néanmoins il faut traiter les deux à travers l’exploration chirurgicale rapide qui peut permettre un diagnostic précoce et un traitement conservateur (Afr J Reprod Health 2009; 13[4]:147-150). KEYWORDS: Tubal torsion, Hydrosalpinx, acute pelvic pain, ultrasonography, surgery. Introduction Torsion of the Fallopian tube is a rare cause of acute pelvic pain which has never been diagnosed pre-operatively. Its incidence is estimated at one in 1, 500,0001 . Clinical presentation is non specific and the diagnosis is usually made at surgical exploration by laparoscopy or laparotomy. Being aware of this complication can help clinicians to suspect it pre-operatively and to make precocious diagnosis which can allow more conservative treatment. Case Report A 34-year-old, single, gravida 0, para 0, with history of sexually transmitted infection. She experienced 6 hours before her admission a severe pelvic pain with nausea and vomiting without vaginal discharge or bleeding. Her blood pressure measured 110/70 mmHg and her temperature was 36.8°C. Abdominal palpation revealed a tenderness of the right iliac fossa. Vaginal examination was very painful and revealed a right adnexal tender mass. Ultrasound revealed a well circumscribed right adnexal cystic mass measuring 82/ 45/ 38 mm without septations. The right ovary has not been identified and the left ovary was normal. White blood count was 9,200/ml; C reactive protein was negative. Ectopic pregnancy was eliminated by negative serum HCG. The patient was suspected to have a pelvic inflammatory disease or an adnexal torsion. She has been admitted and received IV antibiotics and analgesia. Two hours later, the patient had still pain and she was admitted to the operating room. The laparotomy revealed torsion of a right hysrosalpinx with hemorrhage and necrosis. Uterus and ovaries were normal. Right salpingectomy was performed. Postoperative course was uncomplicated and the patient was discharged at the 3rd day. (Figure 1) Discussion Isolated torsion of the Fallopian tube is a rare event, and usually occurs in premenopausal women, rarely in adolescent and postmenopausal women2 . Anatomically, Fallopian tube can be divided to 2 portions. The proximal (intramural segment and isthmus) is fixed to the uterus and have little mobility. The distal portion (ampulla and infundibulum) have a large mobility and have closed relations with ovary. Fallopian tubes and ovaries constitute a real functional and anatomical unit so that isolated torsion of one of them is rarely reported and adnexal torsion occurs more frequently. Many risk factors for isolated tubal torsion have been reported. Shukla3 have collected risk factors reported in the literature and proposed an etiologic classification: (a) anatomical abnormalities (long mesosalpinx, tubal abnormalities, haematosalpinx, hydrosalpinx, hydatids of Morgagni); (b) physiological abnormalities (abnormal peristalsis or hypermotility of tube, tubal spasm and intestinal peristalsis); (c) haemodynamic abnormalities (venous congestion in the mesosalpinx); (d) Sellheim theory (sudden body position changes); (e) trauma, previous surgery or disease (tubal ligation, pelvic inflammatory disease); (f) gravid uterus. Hydrosalpinx is a common long term result of pelvic inflammatory disease. The majority hydrosalpinges are not complicated by torsion because of the high frequency of pelvic adhesions which limits the pelvic organs mobility and prevent torsion. Isolated tubal torsion often occurs in the right side like our case, this can be explained by the presence of the sigmoid colon on the left side which can limit the torsion mechanism4 . Clinical presentation of isolated tubal torsion is non specific. The most constant symptom is acute pelvic pain frequently associated with nausea and vomiting. Vaginal discharge and bleeding have been reported in some cases [5]. Clinical differentiation between adnexal and isolated tube torsion is theoretically impossible. Visualization of elongated cystic mass separate from the ovaries by ultrasound should suggest the diagnosis2 . With Doppler evaluation, the finding of a normal ovarian flow may also be indicative of diagnosis. The differential diagnosis of isolated tube torsion includes adnexal torsion, acute appendicitis, ectopic pregnancy, pelvic inflammatory disease, and torsion of sub-serous degenerative leiomyoma3 . Surgery by laparoscopy or laparotomy is the standard treatment of isolated tubal torsion, it also makes the definitive diagnosis. At the best of our knowledge there has been no preoperative diagnosis of tubal torsion. Surgical management depends on the per-operative aspect of the Fallopian tube, if it is not gangrenous and well vascularized after detorsion the tube may be conserved. A fixation of the tube may be proposed for preventing the recurrence risk and preserving fertility5 . If the tube is gangrenous or damaged by the hydrosalpinx, salpingectomy should be performed. Preventive controlateral tubal fixation is performed systematically or if there is risk factors for torsion6 . Conclusion Isolated tubal torsion is an extremely rare cause of acute pelvic pain. Hydrosalpinx is one of risk factors for this condition. Clinical presentation is non specific and neither imaging nor biology can confirm the diagnosis pre-operatively. Surgery has a diagnostic and therapeutic role. References
Copyright 2009 - Women's Health and Action Research Centre, Benin City, Nigeria The following images related to this document are available:Photo images[rh09055f1.jpg] |
| |||||||||

{kind=link}