 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
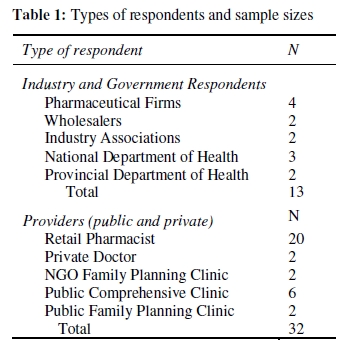
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 9-20 ORIGINAL RESEARCH ARTICLE Promoting and Prioritising Reproductive Health Commodities: Understanding the Emergency Contraception Value Chain in South Africa Promouvoir et identifier les priorites des produits de la sante de la reproduction: Comprendre la valeur de chaine de la contraception d’urgence en Afrique du sud Michael Rogan1* , Priya Nanda2 and Pranitha Maharaj1 1School of Development Studies, University of KwaZulu-Natal; 2International Center for Research on Women (ICRW), India For correspondence: Email: rogan@ukzn.ac.za Code Number: rh10001 ABSTRACT Use of emergency contraception is low in South Africa despite high rates of unplanned and unwanted pregnancies. Existing studies have demonstrated that women access emergency contraception from commercial pharmacies rather than from public health facilities at no charge. Research has also demonstrated that awareness of emergency contraception is a key barrier to improving uptake, especially in the public health sector. This study investigates the low use of emergency contraception in South Africa and employs a qualitative value chain analysis to explore the role of market and regulatory structures in creating an enabling environment for the supply and promotion of emergency contraception. The results suggest that there are several ‘market imperfections’ and information barriers impacting on the effective supply of emergency contraception to women who are dependent on the public health sector for their health care. Balancing commercial interests with reproductive health needs, it is argued, may form a crucial part of the solution to the low uptake of emergency contraception in South Africa (Afr J Reprod Health 2010; 14[1]:9-20). RĖSUMĖ On n’emploie pas beaucoup de la contraception d’urgence en Afrique du sud malgré les taux élevés des grossesses non prévues et non voulues. Les études qui ont été déjà faites ont montré que les femmes ont accès à la contraception d’urgence dans les pharmacies commerciales plutôt que gratuitement dans les établissements de santé publique. La recherche a montré également que la conscience de la contraception d’urgence est un obstacle important qui empêche la fixation surtout dans le secteur de la santé publique. Cette étude examine l’emploi insuffisant de la contraception d’urgence en Afrique du sud et se sert d’une analyse de la chaîne de valeur qualitative pour explorer le rôle du marché et du structures réglementaires dans la création d’un milieu qui favorise l’approvisionnement et la promotion de la contraception d’urgence. Les résultats montrent qu’il y a beaucoup d’imperfections au niveau du marché ainsi que des obstacles à l’égard des informations qui influent sur l’approvisionnement efficace de la contraception d’urgence aux femmes qui dépendent du secteur de la santé publique pour leurs services médicaux. Les gens ont proposé que si l’on met les intérêts commerciaux et les besoins de la santé de la reproduction sur le même pied d’égalité, cela constituera une partie cruciale de la solution au problème du faible accès à la contraception d’urgence en Afrique du Sud (Afr J Reprod Health 2010; 14[1]:9-20). KEYWORDS: Emergency contraception, Reproductive health, Contraception, Value chain Introduction Improving access to and knowledge of new reproductive health technologies is crucial to improving women’s control over their reproduction 1 2. While reproductive health rights have enjoyed increased attention worldwide since the International Conference on Population and Development in 1994 and the Fourth World Conference on Women in Beijing in 1995, barriers to accessing both products and services have limited the impact of these calls to action 3. Emerging reproductive health commodities that can improve women’s control over their reproductive lives often require new and innovative ways of promotion and supply, especially in resource-constrained settings. In South Africa, emergency contraception (EC) is one such product and is defined as the use of a drug or device as an emergency measure to prevent, or reduce the risk of an unwanted pregnancy after unprotected intercourse 4 5. Emergency contraception, also known as postcoital contraception or the morning-after pill, can be used up to five days (120 hours) after unprotected sex and is currently the only contraception method that can be used postcoitally4. The efficacy of emergency contraception depends on when during the menstrual cycle the pill is taken and on what type of regimen is taken 6. The most effective regimen is a single dose of 0.75mg of levogestrinol, although the off-label use of combined oral contraceptive (COC) pills following the Yuzpe Regimen is also effective 4. Contraceptive use in South Africa is high compared to other sub-Saharan African countries. More than 65% of sexually active women currently use any contraceptive method, with most women using modern method 7. High levels of contraceptive use notwithstanding, rates of adolescent and unintended pregnancy remain high. Of all recent births in South Africa, half were unwanted at the time and, among young women aged 19 and younger, 79% were unplanned and 34% were not wanted at all 7. Young women between ages 15-24 have the highest unintended pregnancy rate and the highest unmet need for family planning 7. As a result, there is an urgent need to increase the awareness and use of emergency contraception among this age group in particular 7-9 . Demographic and Health Survey (DHS) data suggest that, although 19.6% of women aged 15-49 are aware of emergency contraception, its use remains very low. Sexually active women aged 15-24 report the lowest use of emergency contraception of any age group, with only 0.2% of sexually active 15-19 year olds and no sexually active women aged 20-24 reporting ever having used emergency contraception 7. Emergency contraception is important to women if they have, as many women in developing countries do, limited control over their sexual or reproductive lives. For those women experiencing sexual violence and coercion, emergency contraception forms an important part of the treatment regime for survivors of sexual violence. A female-controlled product like emergency contraception enhances reproductive choice and is especially useful for women who may have limited control over their sexual lives or are victims of sexual violence 10. In South Africa, as in other developing country settings, rape and other forms of sexual coercion are, unfortunately, very common 11, 12. The high incidence of unplanned and unwanted pregnancies, coupled with sexual violence is occurring in the context of a high prevalence of sexually transmitted infections (STIs). South Africa is currently experiencing one of the most rapidly progressing HIV/AIDS epidemics in the world. According to a 2007 survey, 28% of women attending state antenatal clinics were HIV positive 13. By the end of 2007, there were roughly 5.4 million people living with HIV/AIDS in South Africa 14. Emergency contraception is an important back-up method to the male condom in contexts of high HIV prevalence 15. The promotion of condoms amidst efforts to reduce the spread of the epidemic between sexual partners and the prevention of mother to child transmission have created an important place for emergency contraception as a backup method 16 . Within this context, emergency contraception has the potential to impact on women’s reproductive lives. However, because emergency contraception use remains low in South Africa, identifying the factors inhibiting its use is essential, especially among women with few other means to control their reproductive lives. To date, relatively little attention has been paid to the influence of the market, commercial interests, and regulatory structures on the supply and provision of emergency contraception. In this paper, we employ a value chain analysis to determine how existing supply channels, market structures, and regulatory frameworks enable or inhibit the supply and provision of emergency contraception products in South Africa. In the following section, we describe the emergency contraception value chain as well as our methodological approach to investigating emergency contraception in South Africa. The next section describes the findings, and the last section includes a discussion of how existing supply, regulation, and promotion mechanisms affect the accessibility and use of emergency contraception in South Africa. The emergency contraception value chain Availability of emergency contraception in South Africa In South Africa, the state is currently the main supplier of contraceptives and contraceptive services and all pharmaceutical products are purchased directly from manufacturers in a competitive tender system. Contraceptive services, including methods, are offered free of charge to patients in the public health sector. The majority of women (83%) obtain their contraceptives from public sector clinics and health facilities while the remainder obtain them from private doctors, gynecologists, private hospitals, and pharmacists7 17 18. Public-sector clinics also provide emergency contraception at no charge; it is largely supplied as the off-label use of combined oral contraceptives. Smit et al19 note that emergency contraception course is typically cut up and pre-packaged by dispensary staff and is seldom accompanied by written instructions for users. A dedicated combined estrogen/progestin product has been available in South Africa since 1999 and a dedicated levonorgestrel-only product was registered and made available in 2001. However, these dedicated products are too expensive for most public sector facilities to offer and, consequently, are largely limited to private sector pharmacies 9 19 . Policy support for integrating emergency contraception into the contraception method mix available in public health facilities is strong. In the Department of Health’s Framework for the National Contraception Policy Guidelines 2003, emergency contraception is rated as a core contraceptive option that should be more actively promoted, especially among adolescents, together with condoms for dual protection against pregnancy and STIs (including HIV) 20 21. Policy changes have also impacted on the supply of emergency contraception in the private sector. In 2000, all hormonal products for emergency postcoital contraception were classified by the Medical Control Council as Schedule 2 medicines 20 ; this means that any hormonal contraceptive product, when used as emergency contraception, can be obtained directly from a pharmacist without a doctor’s prescription 20 . In both private and public health sectors, providers are influential in facilitating access to scheduled medicines like emergency contraception. The classification of emergency contraception products as Schedule 2 commodities introduces some specific restrictions to its promotion and provision. As a controlled commodity in South Africa, brand names for emergency contraception products cannot be advertised to consumers. Thus, providers become the main targets for emergency contraception promotion by industry and become particularly important "gatekeepers" of information and access to emergency contraception. This type of market dynamic is especially pertinent to the provision of emergency contraception as the discretion of providers is critical to access 15 22 . As such, the intersection between the manufacturers and suppliers and the providers of emergency contraception is a critical point of investigation. Analytical framework To investigate the supply and promotion of emergency contraception, we adopt an analytical framework based on work by van der Geest and colleagues 23 . They introduce an approach they refer to as a ‘biography of pharmaceuticals’. The authors argue that medical commodities have ‘social lives’ and that by tracing a product from its production to its end consumption, the researcher is able to understand the inherent or constructed value of a pharmaceutical product at each stage of its distribution 23 24. We adapted this framework by adding several methodological components from a value chain analysis in order to obtain a clear documentation of the physical flow of the commodity from production to consumption and to capture the values or factors that are most important to the commercial viability or ‘desirability’ of emergency contraception products at each level of the value chain 25 . Methods Data for the study come from in-depth and semistructured interviews with emergency contraception clients, providers, industry respondents and national and provincial government stakeholders1. The number of respondents from each source is displayed in Table 1. Since only two manufacturers of the most commonly prescribed emergency contraception pills (both dedicated and off-label) operate in South Africa, we sampled pharmaceutical industry association representa-tives and all manufacturers or importers of hormonal contraception that have been awarded tenders with the National Department of Health. Firms were identified through the publicly available tender list for fiscal year 2006-7 and through membership in one of South Africa’s three registered pharmaceutical industry associations. Industry interviews attempted to understand the firm-level perspectives of the potential market for emergency contraception in South Africa. Using a value chain framework, firms were asked to describe and rank the most important factors for the production or distribution of either a dedicated or off-label emergency contraception pill. Respondents were also asked to discuss existing barriers to introducing a new product to the South African market. Types of government intervention were also discussed to determine both the enabling factors and potential interventions to facilitate the increased supply and improved promotion of emergency contraception. Providers of emergency contraception were drawn from a sample area defined as the Durban (eThekwini) central business district in the province of KwaZulu-Natal. The study site was selected due to its location as a major urban transport hub in the province with the greatest range of EC products available. Several South African studies 9 20 have suggested that EC use and awareness is likely to be higher in urban areas. The choice of study site was designed to ensure the greatest possible number of participants in light of the difficulties that other local studies have encountered in identifying users of EC 19 . As such, EC use is expected to be considerably higher within the sample area compared with other parts of South Africaespecially rural areas. Within the sample area, a list of registered pharmacies and dispensaries was drawn from existing databases. The list contained a total of 52 pharmacies and dispensaries located within the sample area. Of these 52 facilities, only three were public health clinics—the rest were commercial pharmacies or private clinics. The main reasons given for refusing to participate in the study included: no time for an interview, did not supply emergency contraception products (for either ethical or commercial reasons), and limited experience in supplying emergency contraception. Interviews with providers were semistructured and were designed to investigate perceptions on the use of emergency contraception products as well as to probe the types of interactions that occur between government, manufacturers and consumers. 1 Data from interviews with users of emergency contraception are being analysed separately. Results Emergency contraception in the public sector Most emergency contraception clients obtain the products from retail pharmacists rather than from public health facilities at no charge 19 . This is somewhat surprising as roughly 80% of South Africans rely entirely on the public health sector for their health care 26 . Most stakeholders suggested that the lack of a dedicated emergency contraception product on the government’s essential drug list signified that emergency contraception is not a public sector priority. In particular, limited resources and a high disease burden were cited as reasons for the ‘crowding out’ of family planning as a whole. As one industry respondent argued, ‘There are so many other public health problems, I can’t see emergency contraception becoming a priority in the public sector. Contraception as a whole might not even feature in the top 20 in terms of government’s priority—with emergency contraception coming even further behind.’ (Industry Respondent #4) Apart from a general lack of emphasis on family planning, however, several attributes of emergency contraception appear to contribute to its relative de-prioritisation by government. In particular, the supply and promotion of dedicated products in the public sector seem to be stymied by their higher cost. A respondent from the National Department of Health, referring to a dedicated product no longer available in South Africa, suggested that the high cost of dedicated products directly contributes to their absence on the tender list and the resulting predominance of off-label products in public health facilities. ‘The reason that we don’t have a separate EC product is cost-this is partially due to a relatively low level of innovation by firms,[i.e.,] simply repackaging and then raising the costs. On the whole, our system—the public sector doesn’t really cater for emergency contraception, so access by pharmacy is perhaps more appropriate.’ (NDoH Respondent) Several industry respondents countered this claim, suggesting that firms are willing to provide dedicated products to government at a preferential price. However, both government and firm respondents noted that communication between government and industry is often lacking and that there is no clear procedure for endorsing particular treatment regimes. With respect to motivating for the placement of a dedicated product on the essential drug list, government respondents claimed that the department of health would not be willing to approach commercial firms to encourage tender applications or to discuss tender specifications, implying that this was the role of industry. Conversely, industry respondents suggested that it was not the place of manufacturers to motivate new entries on the national tender list. Even with the availability of a dedicated product on national tender, however, respondents emphasised that provincial governments play a major role in the implementation and enforcement of treatment protocols and in allocating discretionary funds in their health care budgets for the purchase of emergency contraception products. Such discretionary budgets are controlled by provincial health departments and are typically used to address provincial-specific public health needs. Consequently, they noted, the higher cost of dedicated emergency contraception products is also likely to influence the availability of dedicated products in provincial and district health facilities. As a provincial health department respondent suggested, ‘With respect to promoting a dedicated EC product, cost seems to be a barrier and it is difficult to convince stakeholders of its importance… it is easy to see how this reluctance or indifference trickles down to the level of the provider.’ (Provincial Health Respondent) The same respondent also noted that monitoring and evaluation systems are relatively weak and that the provincial health department does not monitor emergency contraception use. The department currently monitors a large number of health indicators and does not have resources available to expand its database. Without a particularly strong motivation, the respondent suggested, this situation is unlikely to change. Consequently, the actual use of emergency contraception in provincial health facilities will remain unknown. In addition to the cost barrier, several respondents noted several structural barriers inhibiting the promotion and provision of a dedicated product in the public health sector. In KwaZulu-Natal, academic and policy stakeholders have successfully motivated for the purchase of dedicated emergency contraception pills through the province’s discretionary health budget. However, the impact of this on the actual use of emergency contraception appears to be limited; several respondents suggested that attitudinal barriers among both policy makers and providers have prevented the effective promotion and provision of the product. Respondents also recalled that a dedicated product was donated to the Western Cape provincial health department by its manufacturer, but that use was so low that the bulk of the consignment expired and had to be destroyed. Despite the clinical advantages of the dedicated product, respondents explained, treatment protocols were not in place to promote the product or service adequately to public sector patients. In the context of the high prevalence of HIV/AIDS in South Africa, government and industry respondents suggested that emergency contraception has received less attention from public health sector providers because it is a nonbarrier method. They noted that some providers fear that promoting emergency contraception will discourage condom use—perhaps because they perceive clients to be less motivated to prevent HIV than pregnancy—with a consequent increase in the risk of HIV infection. In addition, some providers worry that emergency contraception will discourage abstinence or feel that promoting both abstinence and emergency contraception is contradictory. This perception was echoed by most stakeholders and one industry respondent observed that, In many rural areas, traditional leaders are opposed to EC as it is associated with promiscuity. In many respects, the promotion of EC is tied to the abstinence debate that still surrounds the design and implementation of ‘life skills’ and HIV/AIDS prevention campaigns. (Industry Respondent #4) This concern that emergency contraception promotes promiscuity was also evident among both public and private sector providers. Many public sector providers were concerned that emergency contraception might be perceived as a substitute for condoms, especially among young people. As one provider explained, ‘Sometimes you won’t even mention [EC], like say you look at the client and she is 18 years old—so you’d rather not mention it because you are trying to make them use a condom so that they won’t come back with HIV. So you’re going to not mention it—mention the condom so that they will be protected from STIs and HIV. Because once they know that there is [EC], they just relax and act anyhow. There is an abuse there. I think it's their mentality—they are young and so you try and make them play safer. For the adult person though—you can just say whatever.’ (Public Clinic Provider #3) Providers in the public health sector also noted that very few of their clients requested emergency contraception. They explained this was likely the result of long waiting times at public facilities and the greater accessibility of emergency contraception at pharmacies. As a result, most of the respondents from public health facilities had never provided emergency contraception or did so only several times in a year. Moreover, few of these providers knew that a dedicated emergency contraception product was available in South Africa and none of the facilities in which they worked provided a dedicated product; off-label formulations were all that were available. Market characteristics of emergency contraception Provider roles and creating awareness In light of the resistance and the barriers to the promotion of a dedicated emergency contraception product in the public health sector, the flow of information about emergency contraception products and the creation of awareness are of particular interest. Accessing information about emergency contraception is critical to the improved uptake of emergency contraception products 19 22 27. Almost all respondents suggested that providers play a crucial role in promoting emergency contraception, generating demand, and ensuring awareness among potential users. As one industry respondent relayed, ‘The latent demand for EC and the low awareness of EC products places an emphasis on the importance of providers. While the contraception market is consumer driven, the marketing of emergency contraception would need to be aimed at health care workers. On the whole, for something like [a new EC product] to be successful, the cooperation of nurses, doctors and pharmacists is absolutely critical. No firm, nobody, speaks to the [nursing] sisters themselves. This is partially the domain of government, though-speaking to the sisters on the ground is one thing, getting government to listen to them is another.’ (Industry Respondent #3) Pharmacists, public health workers, and family planning nurses all agreed that word of mouth is likely the most common source of information among users about emergency contraception. However, other providers did note that information about EC is available in public health facilities and that this is important for emergency contraception. As one public health provider explained, A lot of clients will come here because they get information from us. You know-we help them make an informed decision whereas at the pharmacies it’s a matter of ‘here’s my money’ and ‘here’s the product.’ Whereas it is different here in that we counsel them and that’s the part that I think they do appreciate. I think when they come to the clinic they need to get information about [EC]. I think people should know of it. If people are not well-informed then it is likely that they will abuse it. They need proper information about it. Health professionals have an important role to play in getting information to people. (Public Clinic Provider #10) Despite the importance of providers to ensuring that adequate and appropriate information about EC is available and accessible to clients, several attitudinal barriers to EC provision are evident. Government stakeholders were able to point towards ‘misinformation’ that is particularly prevalent in public sector facilities. In particular, a provincial government respondent observed that many providers still perceive emergency contraception to be an abortificient. In KwaZulu-Natal, EC is not always promoted. It seems to be a somewhat emotional topic for many people and there is still a perception that it is abortive rather than contraceptive. Perceptions of promiscuity associated with the use of EC, especially by providers, is also still an issue that needs to be addressed. (Provincial Health Respondent) These associations between emergency contraception, promiscuity, and abortion appear to be rife among providers in both sectors. A significant number of providers were opposed to promoting emergency contraception within their health facilities, although they were not always able to articulate their objections to it. As one retail pharmacist explained, ‘[EC] is basically an abortifacient, there’s no way down the line. If a husband is considering [pregnancy] and says, “Sorry we did make a mistake-please go and see the doctor (for a pregnancy test) or the pharmacist’-this is what he’ll understand is happening, but the word trust comes now and if she [secretly purchases EC] then it becomes a problem and that’s one of my grouses.’ (Retail Pharmacist #4) Thus, despite the important role that providers (both public health workers and retail pharmacists) could play in the promotion of emergency contraception, most respondents argued that emergency contraception is not adequately promoted and that clients rarely receive information about it. Moreover, industry respondents, government stakeholders, and providers themselves described a palpable reluctance among some health care workers to provide both dedicated and off-label EC products. Effective demand and market segmentation As a result of the often prohibitive cost of emergency contraception for consumers in private sector pharmacies and the perceived cost barrier to either supplying a dedicated product in the public health sector or further promoting the offlabel regimens, commercial interest in emergency contraception is typically reserved for markets where there is a proven effective (commercially viable) demand for it. As one industry respondent explains, ‘Norlevo [a dedicated emergency contraception product] is only distributed to the private sector—where it does appear in the public sector, it is not because of the public tender process. The main reason for this is that levonorgestrel is not on the government’s essential drug list so there is not a real attempt to understand demand in the public sector—this is the domain of the health department.’ (Industry Respondent #1) Other respondents added that the total ‘effective’ market for emergency contraception in South Africa is likely to be satisfied by the existing product range. Market research for Schedule 2 products is based primarily on pharmacy and private hospital demand. Industry respondents who worked extensively with the contraception market in South Africa explained that a ‘latent’ (potential) demand for emergency contraception is not evident despite high rates of adolescent and unwanted pregnancies. Moreover, the firm that produces the most commonly used off-label EC product in South Africa noted that it does not measure the off-label use of its product separately from its intended use and has no interest in either measuring EC use or promoting its product as an EC formulation. Thus, neither the public nor the private sectors understand either the effective or the latent demand for a more affordable dedicated or off-label product. The clear demarcation between public and private sector markets was highlighted by a number of respondents as being a significant feature of the market for emergency contraception. Another respondent added that the characteristics of the private sector market for emergency contraception were distinctly different from the public sector and included women who were educated, desired smaller families, and who were employed and more aware of their contraceptive options. In light of the perceived resistance to emergency contraception and its association with promiscuity in some areas and among some providers, industry approaches to marketing emergency contraception have been adjusted. As one industry respondent explains, ‘There are certainly conservative communities and groups in South Africa, but overall demand [for EC] remains high. The way around the ‘ethical’ issues is to identify where demand is high and target places (pharmacies) where ethical resistance is not an issue…. In general, efforts are directed to reach these types of professionals in places like university clinics or anywhere demand for EC is likely to be high ’ (Industry Respondent #1) Industry respondents indicated that the scope for expanding the emergency contraception market is currently limited and that, without a structured intervention, the availability of emergency contraception in the public health sector will remain poor. This is due, at least in part, to a perceived reluctance on the part of government to adequately promote emergency contraception and generate awareness among public sector clients. Within the existing system for tendering for government pharmaceutical contracts, industry respondents viewed the public sector pharmaceutical market as being completely the domain of government. Within the public sector, the promotion and provision also appears to be somewhat disjointed. The integration of overall reproductive health services within the comprehensive primary health care model has, according to some commentators, crowded out family planning to some degree. In particular, service integration may indeed exacerbate the segmentation of the market for emergency contraception along public and private lines. According to a provincial health respondent, ‘I was recently training health care providers in the use of post-exposure HIV prophylaxis for sexual assault survivors and I noticed that none of the health care workers had previously heard of EC. These were health care providers that should have been trained in EC provision, but had not been because they were considered to be working outside of ‘contraception provision’ (Provincial Health Respondent) The respondent further intimated that the consequence of this constraint is that the target group for emergency contraception is limited to users of longer-term methods of contraception. The obvious problem with this, as emphasised by several respondents, is that contraception users may not have the highest demand for emergency contraception and potential emergency contraception users may well fall outside of the traditional contraception market. Moreover, public sector providers reported that emergency contraception is only discussed with patients when they present for a contraceptive method for the first time. The vast majority of respondents reported that emergency contraception is not discussed or promoted outside of an initial contraception consultation. Other industry respondents also indicated that private sector providers or even hospital managers in urban and more affluent areas are the main targets of their promotion strategies. These providers, they argued, are motivated by an existing effective demand for emergency contraception despite a lack of promotion to end consumers. Thus, according most respondents, the promotion of emergency contraception appears to be targeted primarily to private health sector consumers and, to a very limited extent, to contraception clients in public health facilities. Discussion While the findings presented here are not necessarily representative of South African industry, government, and provider perspectives, the study addresses some of the possible reasons for the low use of emergency contraception observed in other studies. In light of the limited empirical data on the actual use of EC and the recent finding that sexually active young women very rarely use emergency contraception 7, the determinants of EC use have been estimated largely from anecdotal accounts and from microstudies of particular risk groups. One contribution of this study is a better understanding of some of the supply side mechanisms that are likely to impact on the use of emergency contraception. A key finding is that fiscal and structural barriers may impede the provision of emergency contraception in both public and private sector health facilities. On the fiscal side, the reluctance of both national and provincial health departments to allocate additional resources to supplying a dedicated product or to improving awareness of existing (off-label) products among public sector clients is an important limitation. Compounding this problem are the likely impacts of what Craddock 30 terms ‘medical capitalism,’ the profit-driven prioritisation of the pharmaceutical industry that ignores the health needs of patients with limited purchasing power. The reluctance of the main off-label manufacturer of emergency contraception in South Africa to market its product as an emergency contraception regimen is a case in point. Similarly, the relative lack of interest of potential market entrants in producing or supplying a dedicated product in South Africa is also significant. This limited commercial interest should be juxtaposed against the fact that half of all recent pregnancies in South Africa were unplanned 7. That these women do not constitute an effective market for emergency contraception clearly pinpoints one of the challenges to improving the promotion of emergency contraception within the current context. Ellerston et al.22 argue that more research focusing on the unmet need for emergency contraception is a likely first step in identifying appropriate markets and for creating demand for dedicated products. Fiscal resources, however, are only part of the explanation for the low use of emergency contraception in South Africa. The study has also identified several structural barriers to its effective provision. The fact that a dedicated emergency contraception product has been available in some public sector health facilities (Western Cape and KwaZulu-Natal provinces) but that use remained low suggests that the physical availability of products is an important but not sufficient condition for improving use. This conclusion is somewhat surprising as policy and service implementation guidelines in South Africa clearly emphasize the role of the public health sector in incorporating emergency contraception into the existing contraception method mix. The implementation of these guidelines, however, has been impeded by a number of health system constraints—some of these related to an overall reluctance to prioritise emergency contraception at the national and provincial levels. One key constraint identified by this study is the reluctance of many providers to supply emergency contraception; this corroborates findings from other local studies 28 29 . This reluctance may stem, in part, from the tension that often exists between the larger public health concern of unwanted pregnancies and the nature of individual contraception consultations as described by Ziebland in a study of EC providers in the United Kingdom and the United States 30 . Within these provider-client interactions, Ziebland 30 argues, EC is often contrasted with other ‘normal’ or ‘proper’ methods of contraception, especially when providers may be misinformed about EC or its perceived impact on sexual behaviour. Some important lessons for improving emergency contraception use in South Africa and in other resource-constrained countries can be taken from the present study. In the South African context, there appears to be a mismatch between the supply of and the latent demand for emergency contraception that is overshadowed by the effective (tangible) market demand for emergency contraception in the private sector. This suggests that commercial interest in emergency contraception is likely to remain focused on existing markets among higherincome groups, while public sector markets are underserved and under-resourced. Much of the available international literature has suggested that creating an enabling policy environment, improving pharmacy access, and registering dedicated emergency contraception products will improve the use of EC among women with limited control over their sexual and reproductive lives 22 31. The results of this study challenge this finding and suggest that commercial interests should not be ignored in attempts to improve EC use, particularly in resource constrained settings. The experiences of the International Consortium for Emergency Contraception in a number of countries have demonstrated that commercial interests and public health interests can be effectively combined in the context of expanding emergency contraception use 32, by, for example, working with pharmaceutical firms to introduce appropriate EC products and to assist them with packaging and marketing. The exact channels through which this might occur are likely to differ from country to country, but one tentative conclusion from the present study is that engaging commercial interest in emergency contraception is likely to be an important step, especially in resource-constrained settings. Improving communication between government and industry is one obvious area for intervention to improve the promotion of emergency contraception in the public health sector. The fact that neither government nor the firms themselves felt they were able to motivate for the inclusion of emergency contraception on the national tender and essential drug lists is an important finding. Significantly, neither party was opposed to providing a dedicated product in the public sector and, in fact, several firms expressed interest in supplying such a product to government, even at a preferential price. An intervention to bridge commercial interests with government’s policy objective to include emergency contraception in the method mix available to public sector clients would be particularly useful. Such an intervention, however, should not ignore the structural constraints that have impeded past efforts to improve emergency contraception use in public sector facilities. Some international evidence suggests that the long-term availability of dedicated products together with educational efforts can generate awareness of and demand for emergency contraception and help providers to view it as a more legitimate method 32-35. Alternatively, other models for including commercial marketing and promotional efforts in public sector facilities could be employed and these do not need to be complex or costly 33. The scope for a public-private partnership in this enterprise, however, appears to be quite limited, at least in South Africa. Conclusion Overall, a value chain analysis has offered a useful tool for investigating the supply side constraints to addressing the latent demand for emergency contraception in South Africa. The results of the study suggest that progressive policy and the availability of emergency contraception products are only the first steps in improving the use of EC, and that market and systems constraints can exacerbate the low awareness and use of emergency contraception. In order for emergency contraception to realise its full potential, South African women, and particularly those who access health services exclusively in the public sector, must be aware of emergency contraception, know where it is available, and must be able to access it free of charge or be able to afford it in the private sector. Effective interventions to achieve this end must address the market and systems constraints identified in this study. Acknowledgements The study was funded by the Ford Foundation, New York through the International Center for Research on Women (ICRW). We would like to thank all of the health care providers, government stakeholders and industry representatives that gave us their valuable time. We are also grateful to colleagues at ICRW (Washington D.C. and Delhi) for comments on earlier drafts of this paper. References
The following images related to this document are available:Photo images[rh10001t1.jpg] |
| |||||||||

{kind=link}