 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
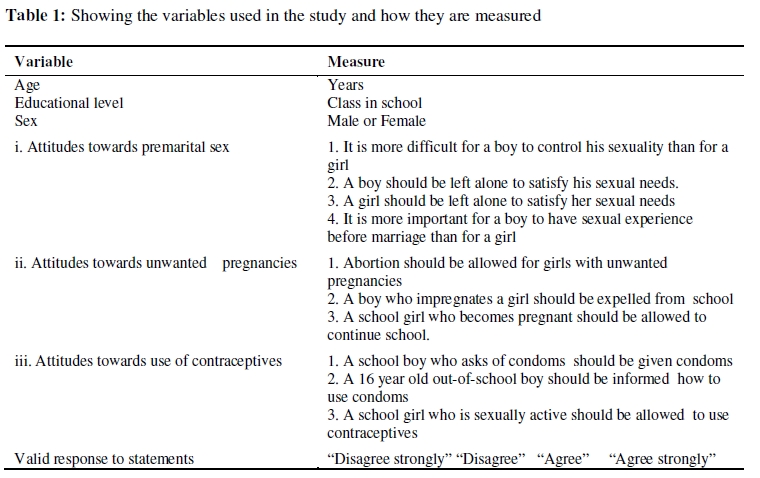
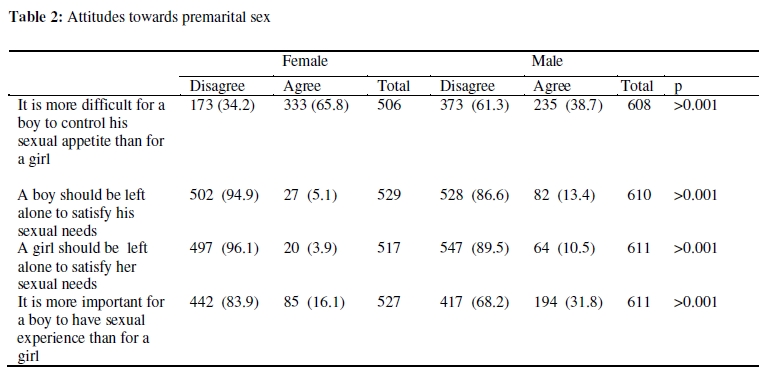
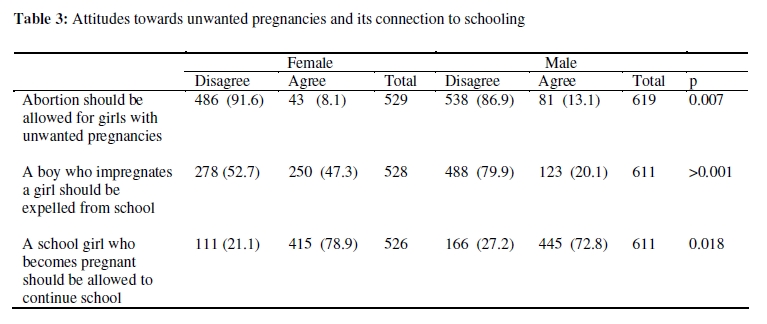
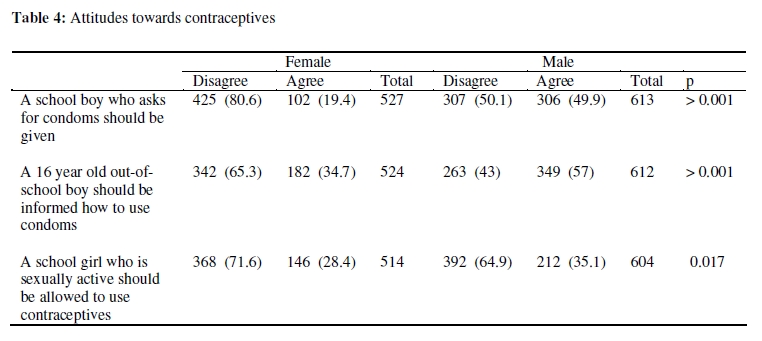
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 33-41 ORIGINAL RESEARCH ARTICLE The Attitudes of Kenyan In-School Adolescents Toward Sexual Autonomy Sunday E Adaji1*, Linnea U Warenius1, Antony A Ong'any2 and Elisabeth A Faxelid1 1Division of International Health, IHCAR, Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden; 2Department of Nursing Sciences, University of Nairobi, Kenya. *For correspondence: Email: sonnyadaji@gmail.com Tel: +234 8052 58 777 1 ABSTRACT This was a cross-sectional study to examine the attitudes of Kenyan in-school adolescents towards premarital sex, unwanted pregnancies/abortions and contraception. Data collection was undertaken using a structured questionnaire. Kenyan in-school adolescents have conservative attitudes toward premarital sex, disagreeing that adolescent boy and girls should be left alone to satisfy their sexual needs. The girls had the view that boys have uncontrollable sexual appetites. With regards to unwanted pregnancies, the majority of the respondents disagreed with allowing abortions for pregnant school girls while they agreed that a pregnant school girl should be allowed to return to school. However, the majority of the girls held the view that a school boy who had impregnated a school girl should be expelled from school. The attitudes of the respondents to contraception were also largely conservative. The conservative attitudes of the respondents conflicts with the findings of high levels of unsafe sex and reproductive ill-health among Kenyan adolescents. There is need to help Kenyan in-school adolescents to develop more realistic attitudes toward sexuality in order to improve their reproductive health (Afr J Reprod Health 2010; 14[1]:33-41). RĖSUMĖ Attitudes des adolescentes Kenyanne qui sont encore etudiantes envers l’autonomie sexuelle. Il s’agissait d’une étude transversale destinée à étudier les attitudes des adolescentes Kenyannes qui sont encore étudiantes envers le sexe avant le mariage, les grossesses non voulues/l’avortement et la contraception. Nous avons collectionné les données à l’aide d’un questionnaire structuré. Les adolescentes Kenyanne qui sont encore étudiantes ont des attitudes conservatrices envers le sexe avant le mariage, n’étant pas d’accord que les adolescents et les adolescentes devraient être libres à satisfaire leurs besoins sexuels. Les filles avaient l’impression que les garçons avaient des appétits sexuels irrépressible. En ce qui concerne les grossesses non voulues, la majorité des enquêtés n’étaient pas d’accord que les étudiantes enceintes aient recours à l’avortement alors qu’ils sont d’accord que les filles enceintes peuvent retourner a l’école. Pourtant, la majorité des filles avaient l’impression que l’étudiante qui est responsable pour la grossesse doit être renvoyé de l’école. Les attitudes des enquêtés envers la contraception étaient aussi en grande partie conservatrices. Les attitudes conservatrices des enquêtés ne correspondent pas aux niveaux élevés du sexe dangereux et la mauvaise santé de la reproduction chez les adolescents Kenyanne. Il est nécessaire d’aider les adolescents kenyans qui sont encore étudiants à manifester des attitudes plus réalistes envers la sexualité afin d’améliorer leur santé de la reproduction (Afr J Reprod Health 2010; 14[1]:33-41). KEYWORDS: Sexual autonomy, Unwanted pregnancies, Premarital sex, Contraceptives, In-school adolescents, Kenya Introduction Globally, the negative effects of sexuality like early and unwanted pregnancy, unsafe abortion and sexually transmitted infections (STIs) including HIV/AIDS threaten the health and social life of adolescents (10-19 years of age) more than any other age group1. These negative reproductive health outcomes are prevalent among the present generation of adolescents in sub-Saharan Africa who were born into the era of HIV/AIDS, widespread poverty, social conflicts and rapid societal changes 2, 3 . Adolescent fertility and sexuality is a major public health issue in Kenya where adolescents constitute about 26 percent of the population. Sexual activity begins early, with 42 percent of girls aged 15-19 years having ever had sexual intercourse and 17 percent currently being sexually active5. The median age of first intercourse rose from 16.8 years in 1998 to 17.8 years in 20035. Marriage, however, takes place later and in 1998 the difference between the median age at first sex and first marriage was estimated to be three years. This gap between the median age of first sex and marriage was found to be wider in boys compared to girls6. In 2001, a study in Kisumu (where this study was carried out) showed that, by 14.5 years of age, a quarter of both boys and girls had already experienced sex while at 17 years, half of both sexes would already have had sex. The median age of first marriage was, however, about 19.6 years for women and 25.5 years for men7. The widened gap between the age of sexual debut and the age at first marriage means that many young people in Kenya may be exposed to a prolonged period of premarital sex. Furthermore, many young people have sex with multiple partners and one study from Kenya showed that boys were seven times more likely than girls to have multiple partner sex 8. Despite pre-marital sex and multiple sexual partners among Kenyan adolescents, the use of contraceptives including condoms is low 5, 9, 10. Studies have shown that even though adolescent boys may have knowledge about condom use and the protection it offers against unwanted pregnancies and STIs including HIV/AIDS, male norms favouring sexual experience without condoms often prevents them from using condoms correctly and consistently 11 . Furthermore, prevalent societal norms limit young women’s access to and use of contraceptives 12 . Paradoxically, such norms emphasize sexual submissiveness and weaken young women’s ability to negotiate the use of contraceptives 13, 14. As a result, unwanted pregnancies and abortions are reported to be prevalent among Kenyan in-school girls. In the 1990s, teenage pregnancy rates (i.e. the percentage of pregnancies occurring in adolescence) were reported to be 10.5 and 13.5 percent in two large hospitals in Nairobi respectively15. Results from another study showed that 42 percent of pregnancies among secondary school girls resulted in induced abortions 16. It has also been reported that adolescent girls aged 15 – 19 years accounted for 19 percent of abortion related complications in Kenyan hospitals in 200317 . As seen in the above literature review, sexual autonomy for women and girls, especially as it applies to premarital sex, prevention and termination of unwanted pregnancies remains a highly contentious issue in Kenya 13, 49. As the population of adolescents in Kenya increases, the debates about adolescent sexuality, school girl pregnancy and its consequences become fiercer in the medical and lay press. This is because of concerns that sex education and distribution of contraceptives including condoms could erode moral and traditional values and norms18. Yet, the perspectives of adolescents and their voices on these issues remain largely unheard. It is imperative to understand attitudes of Kenyan adolescents towards premarital sex and unwanted pregnancies in order to design appropriate sexual and reproductive health interventions for adolescents. This study seeks to investigate the attitudes of in-school adolescents in Kenya toward sexual autonomy in order to gain insights that could be used to address their sexual and reproductive health needs. Methods This was a cross-sectional, descriptive survey carried out among in-school adolescents in Kenya in 2002. Ethical clearance was obtained from the ethical review boards in Stockholm, Sweden, and the Ministry of Education, Science and Technology /Office of the President, Kenya. Permission to administer the questionnaires was obtained from the principals of the schools involved in the study. The nature and purpose of the study were explained to the students and verbal consent was obtained. The study was carried out in Kisumu, a port city on Lake Victoria, the world’s second largest fresh water body. With a population of about 500 000, Kisumu is Kenya’s third largest city, and situated about 400 kilometers northwest of Nairobi. Kisumu is the capital of Nyanza Province, and is considered Western Kenya's most important urban area with the majority ethnic group being the Luos, the third largest in Kenya. Other ethnic groups are also well represented. Kisumu is served by a number of public schools (including one university and two colleges / polytechnics). The primary school gross enrolment rate is 69.7 percent but the secondary school enrolment rate is only 19 percent 19. Seven schools which were within 30 minutes walking distance of an identified health center were randomly selected for the study. These consisted of 4 single sex schools (2 for boys and 2 for girls) and 3 mixed schools. In each of the schools one arm of a class from Forms 1 -VI with approximately 40 to 50 students in each class was randomly selected and entered into the study. A total of 1202 students were in the selected classes. The data was collected in each school by a team of trained senior nursing staff from government hospitals. The instrument used a modified Likert Scale which consisted of 10 positively and negatively worded statements written in the English language (which was the language of instruction in the schools) intended to evaluate attitudes towards premarital sex and unwanted pregnancies and pregnancy prevention as outlined in Table 1. A four-point response format was used (disagree completely, disagree, agree and agree completely) to enable the respondents to specify their level of agreement to each statement. Each student was given a questionnaire and instructions on how to respond. SPSS version 10 for Windows was used for statistical analysis. The data was reduced to nominal level by categorizing all the responses in the four-point scale into two categories of “Disagree” and “Agree”. This was done in order to get a clear picture of the participants’ attitudes. Numeric data (age) was described using median and range and nominal data was described using frequency distribution tables and crosstabulations. Chi-square test was used to compare proportions with 0.05 set as the level of statistical significance. Analysis was also done with respect to sex of the respondents. Results A total of 1159 students who completed their questionnaires according to instructions had their data analyzed. The rest (43) of the students returned their questionnaires uncompleted and these not analyzed. Of 1159 study subjects, there were a total of 533 girls constituting 46 percent of the respondents and their age ranged from 13 – 19 years with a median of 16 years. There were 626 boys (54 %) whose age ranged from 13 – 19 with a median of 17 years. Attitudes towards premarital sex Table 2 shows the response of the students to the 4 questions related to premarital by sex. In all the responses there was statistically significant difference between the responses of the female and male students. Attitudes towards Unwanted Pregnancies and Induced Abortions The three statements related to attitudes towards unwanted pregnancies, induced abortions and the connection to schooling are, and the responses of the students are shown in the Table 3. Even though most of them expressed conservative views, there was statistically significant difference in the responses along gender lines. Attitudes towards contraceptives As shown in Table 4 below, the views of the respondents to the statements related to contraceptives were largely conservative. These views varied along gender lines. Discussion Our findings show that Kenyan in-school adolescents have conservative attitudes towards premarital sex. This conservative attitude to sex may not, however, translate to practice and contrasts sharply with the level of unsafe sex that has been described among adolescents in Kenyan society12, 20. Strong religious influence and deeprooted cultural values in Kenya prohibit premarital sex. But faced with social and biological pressures to engage in sex, adolescents find it difficult to match their attitudes with their practice 21. Such strongly conservative attitudes could hinder adolescents from accessing useful sexual and reproductive health information and services, which they need in reality. Gender differences in attitudes towards sexual behaviour were also portrayed in this study. For example, the majority of the adolescent girls perceived it more difficult for boys to exert sexual control compared to girls. This attitude may be grounded in societal stereotyping of uncontrolled sexual appetite as an expression of maleness. Girls are not expected to question this notion of maleness, rather they are taught to be submissive and accept it. Boys are expected to be dominant in relationships with girls and they earn respectability by sexual conquests22, 23. Interestingly, in this study, the majority of the boys disagreed with this perception of uncontrollable male sexual appetite. This attitude of male adolescents may be the reality or a deception in an attempt to please the investigators. Girls’ perception of uncontrollable male sexual appetite could lead to unsafe sex as it might encourage sexual submissiveness to boys in resignation and forgo protective sexual practices24, 25. For example, girls may still tolerate their male partners having unsafe sex with other sexual partners because of their acceptance of the notion that boys have uncontrollable sexual urge. Also with regards to unwanted pregnancy and abortion among school girls, the attitudes of the respondents were largely conservative. The majority of the respondents disagreed with allowing induced abortion for school girls with unwanted pregnancies. Their negative attitude is, however, in conflict with the high rates of abortions among in-school adolescent girls reported in several studies from Kenya16. The pervasive influence of the church could be one reason for this negative attitude to induced abortion. In Kenya, over 300 000 women undergo unsafe abortions each year and 30 percent of maternal deaths are blamed on unsafe abortions, yet, a recent attempt to liberalize abortion laws met stiff opposition spear-headed by the Church26 . School girl pregnancy and its connection to school drop-outs is a concern both in Kenya and in other sub-Saharan African countries28, 29. Our study showed that most of the Kenyan girls and boys agreed that girls who become pregnant should be allowed to continue school. Most also agreed that a boy who impregnates a girl should continue school. This attitude is, however, in conflict with that of many Kenyan teachers. An earlier study in Kenya revealed that teachers (including female teachers) favored forcing pregnant girls out of school. Most of the teachers even felt that such girls should be disallowed from coming back to the same school after they delivered their babies28. In the same study, only a small proportion of the teachers favored asking boys who impregnated girls to leave school28 . This is despite the fact that Kenya has had a school reentry policy after pregnancy and childbirth since 199430 . Some gender differences in the responses of the students are noteworthy. For example, there were significant gender differences in the response to the statement that a boy who impregnates a girl should be expelled from school. More girls than boys favored expulsion of such boys from school. On the other hand the majority of the boys were of the view that pregnant girls should be allowed to continue their studies. This study did not explore the reasons for the positive disposition of the girls towards expulsion of boys. However, it may be speculated that the girls were agitating for equal treatment for female and male adolescents who are implicated in schoolgirl pregnancy. The positive disposition of Kenyan teachers towards expulsion of pregnant school girls as documented in the literature28 , and that of the girls towards boys responsible for impregnating girls as seen in our study, could be an evidence of tensions in gender relationships in the school environment. Lloyd and colleagues argued that these gender tensions and the double standards in favour of boys in schools could account for school dropouts for girls even for other reasons than pregnancy31 . With regards to contraceptives, in-school adolescents in this study also displayed conservative attitudes. This was more among the female adolescents compared to the boys. This is worrying because of the fact that pregnancy prevention is often considered the responsibility of the girl 11, 23. In the event of pregnancy, girls face the health and social consequences while the male partners tend to deny responsibility 3, 23. The conservative attitudes of the respondents to the use of condoms are particularly worrying. Because of the dual protection that condoms offer, they are considered ideal for school aged adolescents and their distribution has been a feature of many adolescent programs. The negative stance of the Catholic Church (which is a significant social and moral force in Kenya) towards condoms could be responsible for this finding18. Many Kenyans also worry that easy access to condoms could encourage sexual promiscuity among adolescents21 . There is therefore a need to invest more in showing the health and social benefits of easy access to condoms among Kenyan adolescents and dispelling the myths and perception surrounding contraceptive services to adolescents. Our findings locate Kenyan in-school adolescents as having conservative attitudes rooted in cultural norms and moral values, which could jeopardize their sexual and reproductive health. Enhancing access to reproductive health information and services for in-school adolescents could change this conservative stance, but may be a difficult task in Kenya. The application of the rights based approach to sexual and reproductive health could help to change how adolescent sexual and reproductive health services are offered and utilized in Kenya. Under the rights-based approach, states have obligations to respect, protect and fulfill the sexual and reproductive rights of adolescents 32-34. The rights perspective in schools has many benefits. Rights education can for instance empower adolescent boys and girls of all ages and the community by instilling a sense of entitlement and establishing new social norms 35 . A rightsbased approach could help school teachers and reproductive health providers to clarify their values and provide an ethical framework for them to deliver their services36 . At the national level, governments are put under pressure to adequately address the sexual and reproductive health needs of adolescents37 . Furthermore, a rights-based approach helps governments to understand the social determinants of attitudes and behaviour related to sexuality and reproductive health outcomes, for example, gender inequalities. In this way, interventions can reach beyond the health sector to address these determinants38, 39. Methodological Issues A questionnaire based survey such as this, may only have made a spot evaluation of the attitudes of the respondents without further exploration of the motivations behind the attitudes portrayed. Furthermore, although the statements in the questionnaire were crafted to make them nonjudgmental, the responses may have been swayed by the presence of the researchers whom the respondents may want to please. Sex-related terms could conflict with moral inclinations and also influence the responses obtained. However, the use of questionnaire-based cross-sectional studies of this sort in sexual and reproductive health is not new. For example, Kiragu and Zabin used it to survey attitudes to contraceptive use among high school students in Kenya49 , and Eggleston and colleagues used it in a study of sexual attitudes and behaviour among young adolescents in Jamaica50 . Becker and colleagues also used it to evaluate the knowledge and opinions of Mexican youth to abortions and abortion law in Mexico51. In all these situations, the findings provided useful insights into the sexual and reproductive health of the groups that were studied. Furthermore, this study was carried out in only seven schools in Kenya and the findings may not totally represent the views of all in-school adolescents in Kenya, as adolescents are not the same everywhere. In addition, out of school adolescents were not involved in this study and their attitudes might be different. Despite this, the application of the rights-based approach could be of benefits to all adolescents Conclusion As shown in our study, Kenyan in-school adolescents portray strong conservative values which could hide their true sexual behavior, thereby increasing their vulnerability to reproductive ill-health. The findings of this study which gives insight into adolescent attitudes towards sexual and reproductive health however needs to be complemented by further studies using qualitative methods. Such a study will help to explain the conflicts between the conservative attitudes of adolescents towards sexual autonomy and the poor adolescent sexual and reproductive health indicators in countries like Kenya. References
The following images related to this document are available:Photo images[rh10003t2.jpg] [rh10003t4.jpg] [rh10003t1.jpg] [rh10003t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}