 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
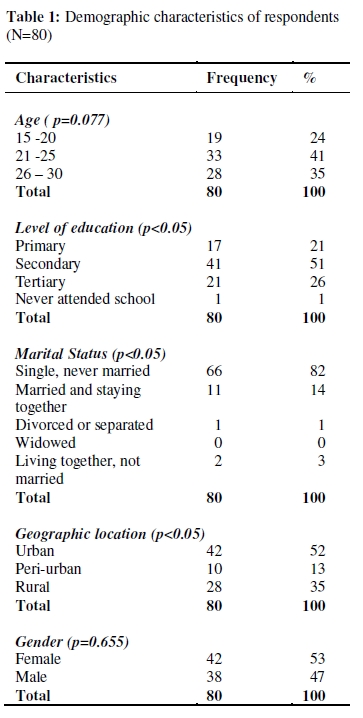
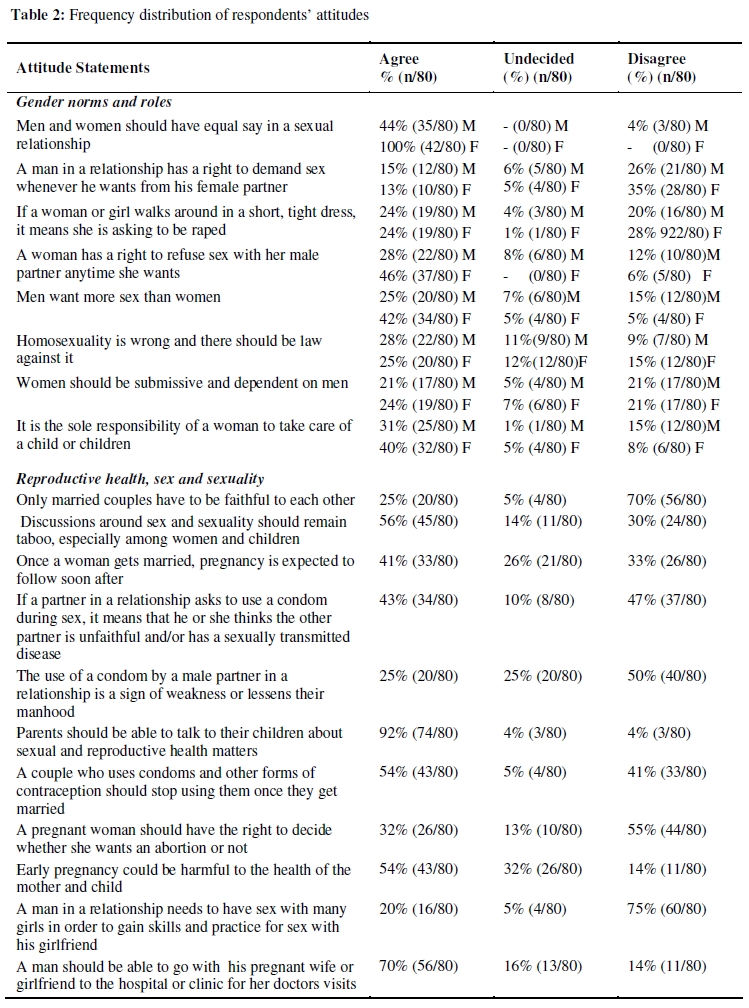
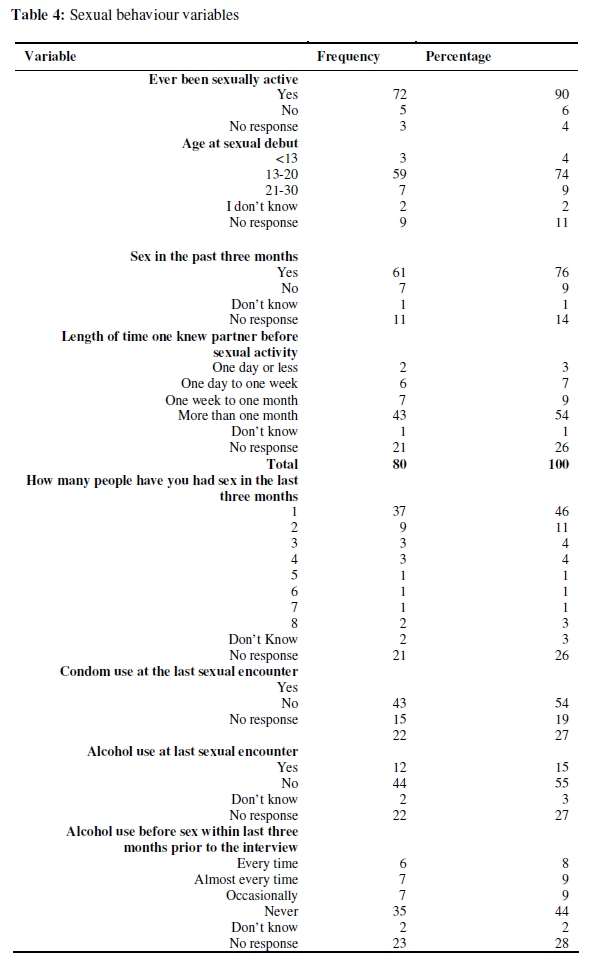
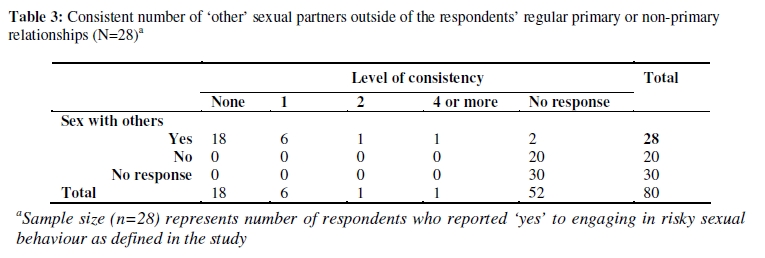
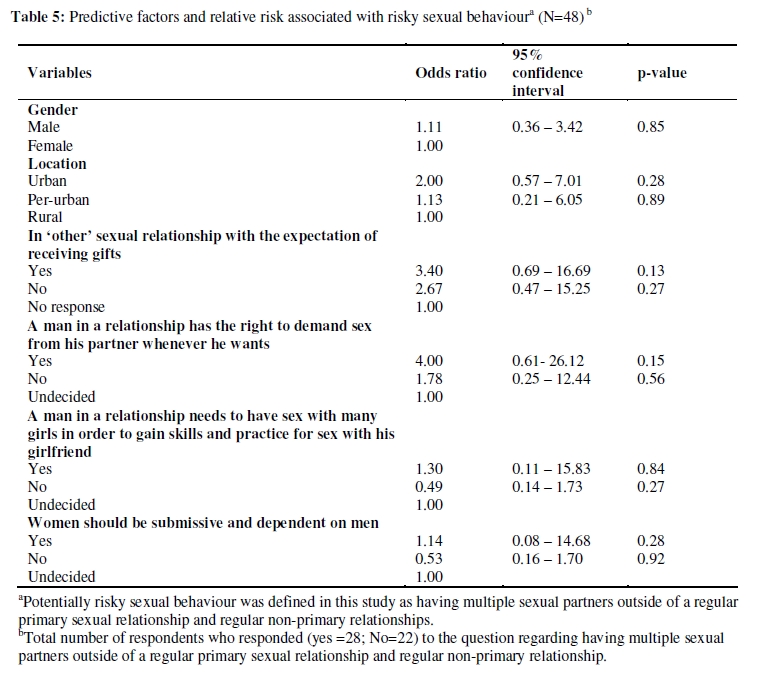
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 55-69 ORIGINAL RESEARCH ARTICLE Factors that Influence Attitudes and Sexual Behavior among Constituency Youth Workers in Oshana Region, Namibia Olusheyi O Lawoyin1* and Ruth M Kanthula2 1Oshana Health Regional Office, Private Bag 5538, Oshakati, Namibia; 2Ben Gurion School of the Negev, Faculty of the Health Sciences, Medical School for International Health, P.O. Box 653, Beer-Sheva, Israel 84105 *For correspondence: Email: slawoyin@gmail.com Tel: 001-2023-447-241 Fax: 001-4103-812-994 ABSTRACT This survey was carried out to assess attitudes and behaviour among youth within four constituencies in Oshana region, Namibia and to understand to how certain social and cultural factors inform attitudes and influence sexual behaviour among the population of young people surveyed. Using a structured questionnaire, data were collected from a random sample of eighty young men and women between the ages of 15-30 years from four constituencies in Oshana region. Survey outcomes revealed attitudes and certain factors that are linked to sexual risk behaviour such as multiple sexual partnerships. Outcomes also reveal an influence of established socio-cultural norms on gender dynamics within relationships and a culture of reserve around discussions of sex and sexuality among young people. Stakeholder interventions should be directed towards incorporating approaches that address these factors as part of efforts to curb the incidence of HIV among young people in Namibia (Afr J Reprod Health 2010; 14[1]:55-69). RĖSUMĖ Facteurs qui influent sur les attitudes et le comportement sexuel chez les travailleurs dans la circonscription electorale de la jeunesse dans la region d’Oshana, Namibie. Nous avons entrepris cette étude pour évaluer les attitudes et le comportement dans quatre circonscriptions, électorales dans la région d’Oshana, en Nambie et pour comprendre comment certains facteurs soucieux et culturels affectent des attitudes et influencent sur le comportement sexuel chez la population des jeunes gens enquêtés. A l’aide d’un questionnaire structuré nous avons recueilli des données d’un échantillon au hasard de la part de quatre-vingt jeunes hommes et jeunes femmes âgés de 15 – 30 ans qui venaient de quatre circonscriptions électorales dans la région d’Oshana en Namibie. Les résultats de l’enquête ont révélé des attitudes et certains facteurs qui sont liés au comportement des risques sexuels tel le fait d’avoir des partenaires sexuels multiples. Les résultats ont révélé également une influence des normes socioculturelles établies sur les dynamiques de sexe au sein des rapports et une culture de réserve autour des discussions sur le sexe et la sexualité parmi les jeunes gens. Les interventions des intéressés devraient être dirigées vers l’incorporation des approches qui abordent ces facteurs comme faisant partie des efforts pour réduire l’incidence du VIH chez les jeunes gens en Namibie (Afr J Reprod Health 2010; 14[1]:55-69). KEYWORDS: Sexual risk behaviour, Gender, HIV prevention, Sexual and reproductive health Introduction Tulongeni Youth Service suppliers (TYSS), a non government youth development organization in Oshakati, Namibia launched a six month youth HIV/AIDS and education project. It focused on behaviour change communication and community mobilization activities with a view to addressing social and cultural factors that influence HIV transmission among a target population of young people from Oshakati East, Ompundja, Oshakati West and Ondangwa constituencies, who volunteer their time and services to the organization. The project comprised of three components including a survey assessing attitudes and behaviour, a training of trainers workshop for youth on behaviour change communication strategies and a male engagement in HIV prevention and gender norms symposium. The TYSS staff conducted a survey of youth constituency workers who were elected to serve as youth representatives in their respective communities and also actively volunteered their time at TYSS. Preliminary results of the survey were used to inform the training workshop and the youth symposium and to further guide the organization’s capacity to develop, implement and prioritize HIV prevention interventions. This article presents an analysis of the results of this survey as it pertains to health among youth volunteers with TYSS. Namibia a country with an estimated 2.1 million people remains one of the countries in sub-Saharan Africa largely affected by the HIV epidemic, with an estimated number at 200,000 people infected with HIV/AIDS and adults ages 15 years and older representing 90% of those infected1. The Caprivi, Oshana, Khomas and Erongo regions have been hit hardest by the AIDS/HIV epidemic2. In Oshana Region, the prevalence rates are particularly high among the youth aged 15-24 with a prevalence rate at 20%2. Oshana Region is the smallest and the most densely populated of the thirteen regions in Namibia with an estimated population at 177,0223. It is situated in the central northwest and is bordered by Oshikoto to the east, Omusati to the Northwest, Ohangwena to the north and Kunene to the south3. Most of the population resides in rural areas that rely on subsistence farming including cattle farming and maize crops as their main source of household income4. The total population of youth in the region is estimated at 50,357, which is 31% of the total population of Oshana Region4. The epidemic remains a challenge to the region’s large youthful population as the value of young people’s capacity to effectively contribute to the development of the region and country as a whole is undermined by the high transmission of HIV and other STIs and early pregnancy. Drivers of the epidemic in Namibia include factors that may be tied directly or indirectly to established cultural and societal norms that influence negative or unhealthy attitudes and behaviours that are not perceived as high risk. Some of these include a cultural aversion to the use of condoms, cultural taboo on an open discussion of sex and the subordinate socio-economic status of women5. Social and cultural context in Namibia It is often not enough to talk about sex and reducing HIV/AIDS without understanding the context of cultures and traditions. Across the various cultural groups within the country, a wide gap exists in the social and economic condition between men and women that are defined by social institutions including the family, church, schools6. Women are generally seen as subordinate to men and are socialized to be obedient and tend to their families6. In addition to this, violence against women, adolescent girls and young children is prevalent, a problem that is compounded by the status of women in society which more often than not leaves them with little or no negotiating power on matters related to their sexual health. It is important to also consider the gender imbalance that exists when trying to understand HIV transmission among young people in the country. Socio-cultural factors and HIV/AIDS A sizeable body of evidence exists on social and cultural factors that influence HIV transmission among young people in the Southern African region. The findings from a review of sexual behaviour among young people between the ages of 14 and 35 in a South African study, illustrate the strong influence of social norms on unsafe sexual behaviour7. Certain cultural and social patterns have also been shown to account for high HIV prevalence rates in countries like Botswana and Zambia 8,9 . A study conducted in Kwazulu-Natal, South Africa examined the relationship between gender, gender roles and the social impact on adolescent child bearing, revealing that such factors were grounded in negative cultural and social traits that placed them at risk for early pregnancy as well as other sexual and reproductive challenges10, 11. Pettifor et alproposed, based on study findings, that gender power inequalities are key to the transmission of HIV as they affect a woman’s power in a sexual relationship, especially in negotiating condom use. In Namibia, there is a sense of awareness of the influence of certain social and cultural norms on the transmission of HIV among at risk populations including young people. According to the Namibia Country Strategic Plan 2004 – 2010 on Gender Assessment, it was reported that a linkage has been recognized between the transmission of HIV/AIDS and other STIs and a prevailing situation of an implied acceptance of stereotypical views of gender roles, including a passive tolerance for male dominance, aggression and promiscuity. Further more, it addresses the fact that the epidemic develops within certain social, cultural and historical contexts, perpetrating certain expectations and beliefs that contribute to the vulnerability of individuals and communities6. For example, a commonly accepted view among young men is that violence against women is socially sanctioned as a legitimate expression of male authority12. Another widely held view, shared by some women and frequently used to justify sexual violence, including rape, is that male sexual urges are uncontrollable and should be acted upon as part of the social norm for the male to be sexually dominant12 . In a knowledge, attitudes and practices study that was conducted in different parts of the country including two towns in Northern Namibia, it was found that having two or more sexual partners, a behaviour that was common in the study sites due to cultural norms, posed a strong risk of HIV transmission13 . Findings from a study 14 that examined structural influences of HIV/AIDS progression indicated that gender inequality is a social structural factor that places women at a greater risk of HIV infection due to their inability to lower risk-taking behaviour as a result of prevailing cultural practices, social norms towards women, and gender inequalities. In many cases, issues pertaining to male involvement in HIV prevention have been relevant to addressing certain social and cultural norms that drive the HIV epidemic in Namibia. An earlier study among Ovambo men and women suggest linkages between masculinity, as defined by the culture and society, and AIDS and suggest options for providing alternative indicators of masculinity in HIV prevention efforts15. While the influences of these social and cultural factors on HIV transmission is prevalent as evidenced by these reports, data on the influence of certain social and cultural factors on HIV transmission among young people in Northern Namibia, particularly in Oshana Region remains limited, especially in a region with one of the highest rates of HIV/AIDS in the country2. Addressing HIV prevention among the large population of young people in Oshana region, Namibia is an issue that can be strengthened by implementing approaches that fit the contextual needs of members of this population across the age spectrum. Further data collection will be useful in helping to better understand new approaches to HIV prevention among young people within the region, with a view to designing interventions and strategies that have an influence on prevailing attitudes and behaviour while promoting healthier behaviours and lifestyle choices. To this end, this survey was conducted to assess prevailing attitudes and sexual behavior among a sample of young people in order to understand behavioral and contextual factors that increase the vulnerability of this population to HIV acquisition. Results of which will contribute to the development and implementation of appropriate interventions that will serve the needs of youth. Methods Survey sample The sample size consisted of eighty constituency youth workers between 15-30 of years age who served at TYSS as volunteers and were from four constituencies in Oshana Region that were primarily represented at TYSS: Oshakati West, Oshakati East, Ompundja and Ondangwa. Sampling from these four constituencies was done due to time and financial constraints, and because preliminary results of this cross sectional survey would be used to design interventions specifically targeted towards young people from these particular constituencies. The youth constituency workers were selected to participate in the survey because they were recognized as leaders within their respective communities and their attitudes and behaviours will likely be reflected by their peers. As they serve in a position where their attitudes and behaviours might be reflected by their peers, it is within reason to select them as our sample for this survey. However, it should be noted that the respondents do not make up a representative sample of the general youth population within Namibia or Oshana region. Respondents were selected from the four main constituencies that were highly represented at TYSS, who remained the target population of future programs that were implemented as a result of the preliminary findings from this survey. Questionnaire and field collection Face to face interviews were conducted by a team of five trained youth community volunteers, who were fluent in both English and the local language, to administer the survey over a ten day period, using a structured questionnaire for data collection. The data depended primarily on quantitative data collected in the field. Qualitative data was also collected by the interviewers to complement quantitative data and provide substance to the raw data as necessary. The survey included an informal discussion around the responses to the questions, which were also recorded by the interviewers. The questionnaire was written in English and an important part of the training included a discussion on the appropriate wording to use for translating certain questions into the local language, especially for participants who were not fluent in the English language. It included questions on demographic characteristics, attitudes towards gender norms and roles and sexual and reproductive health as well as sexual behaviour. Verbal informed consent was obtained from respondents before interviews. Anonymity was maintained and particpants’ names were not required. Permission to carry out the study was obtained from the Oshana Regional Council and constituency councillors for each of their constituencies that were represented in the survey. Data analysis Checks for errors and inconsistencies were carried out before data entry. Survey responses were recorded using a coded system and subsequently entered into a computer’s database system using SPSS version 11.5.1 for windows. The data was further analyzed using the SPSS software, where tests of association between certain variables were based on the chi-square test or fisher’s test as appropriate. Attitude was measured on a 3-point Likert-type scale to allow for agreement, neutrality and disagreement to questions on gender roles and norms and sexual and reproductive health. A score of 1 was given to agree response, 2 to neutral response and 3 to a disagree response. The scores were reversed for positively framed questions and a composite attitude score was computed for each respondent. It is expected that responses to each likert item (question) on the scale will evaluate the participants attitudes according to any kind of subjective or objective criteria they hold as influenced by socio-cultural context. The questions on gender roles and norms were scored separately with a score range of 8 to 24 for both. Scores above 17 indicated positive attitude. Questions on sexual and reproductive health was on a score range of 11 to 33. Scores above 24 indicated a positive attitude. Predictive factors related to risky sexual behaviour, were tested for association using logistic regression analysis. Summary and frequency tables were produced and cross tabulations were performed to compare certain variables. Results Demographic characteristics Age distribution: The ages of the survey respondents ranged from a reported 17 to 30 years old with a mean age of 23.84 (± 3.7) (Table 1). Education level: Many of the respondents (51%) had secondary education while 26% (n = 21) had tertiary education. The rest of the respondents had primary education, 21% (n=17) and one person had never attended a formal institution of learning. Marital status: Eighty-two percent (n=66) of the respondents reported being single and never married, fourteen percent (n=11) were married and living together with their partners. Three percent (n=2) were living together but not married while 1% (n=1) was divorced or separated from their spouse. Geographic area: Fifty-two percent of the study respondents (n=42) resided in urban areas, 13% (n=10) in peri-urban and the remainder at 35% resided in rural areas. Gender: Forty-seven percent (n=38) of the respondents were male, while 53% (n=42) were female. Attitude Gender norms and roles Female youth When asked whether men and women have an equal say in relationships, 100% of respondents disagreed with this statement. Forty-two percent (n=34) agreed that men want more sex than women. Twenty-three percent (n=19) agreed that women should be submissive to men; although it is important to also note that twenty-one percent (n=17) disagreed with this same statement. Forty percent (n=32) were of the belief that it is the sole responsibility of the women to take care of a child or children in the home and only six percent (n=5) disagreed that a woman in a relationship has a right to refuse sex whenever she wants (Table 2). Male youth Forty-four percent of male participants agreed that men and women should have equal say in relationships and twenty-eight percent (n=22) agreed that a woman has a right to refuse sex whenever she wants in a sexual relationship. Many, 28%, also agreed that a law should be instituted against homosexuality and 31% (n= 25) agreed that it is the sole responsibility of a woman to take care of a child or children in a relationship. Twenty-six percent (n=21) of the male respondents disagreed that a man has the right to demand sex from his female partner whenever he wanted (Table 2). Sexual and reproductive health When it comes to discussions around sex and sexuality, the majority of male and female participants agreed that it should remain a taboo topic especially around women and children. Seventy percent (n=56) of the respondents disagreed with the statement that only married couples have to be faithful to each other. When asked whether to agree or disagree with the statement that ‘a couple should stop using condoms and other forms of contraception once they get married’, fifty-four percent (n=43) agreed with this statement. Fifty-five percent (n=44) of all respondents disagreed that a pregnant woman should have the right to decide whether she wants an abortion or not. In regards to pregnancy after marriage, many 41% (n=33) agreed that once a woman gets married, pregnancy is expected to follow soon after. Ninety-two percent (n=74) of the respondents agreed that parents should be able to talk to their children about sexual and reproductive health matters. However, while fifty-four percent (n=43) agreed that early pregnancy in regards to young maternal age can be harmful to the health of the mother and child, a large number at thirty-two percent (n=26) remained undecided in their response to this statement. Seventy percent (n=56) agreed that a man should be able to go with his pregnant wife or girlfriend to the hospital or clinic for prenatal care. Sexual Behaviour Sexual Behaviour and age at sexual onset Ninety percent (n=72) respondents reported ever having sexual intercourse. The reported range for age at sexual onset among the respondents was from 12 to 30 years (Table 4). Sexual activity within the last three months Seventy-six percent (n=61) respondents reported sexual activity over the past three months prior to the date of their interview with as many as one to eight individuals, including married, non-married and non-regular sex partners. Twenty-six percent (n=21) respondents did not respond to the question while 3 %( n=2) of the respondents reported that they did not know how many individuals they had been with over that time period (Table 4). Of those that engaged in sexual activity over the past three months, fifty-four percent (n=43) reported that they had known their regular primary sexual partner over a month before they had sex with them, 3% (n=2) reported knowing their sexual partners at one day or less, 7% (n=6) of them from one day to a week and 9% (n=7) of them knew their sexual partner from one week to a month prior to sexual contact (Table 4). Three percent (n=2) of the respondents reported that they did not know how many people they engaged in sexual activity, while twenty-six percent (n=21) of the respondents did not respond to the question (Table 4). Of the total number of participants who responded to the question (n=48), 42% (n=20) reported no ‘other’ sexual relationship outside of their regular primary or regular non-primary sexual partners, while 58% (n=28) reported multiple sexual relationships with individuals outside their reported regular primary sexual relationship or regular non-primary sexual partners during the three month period. Of these 28 respondents, 23% (n=18) reported that the ‘other’ individuals that they had sexual relations with were not consistent, 8% (n=6) reported consistent sexual activity with one other person, 1% (n=1) with two other people and 1% (n=1) with four or more other people (Table 3). Twelve out of the twenty-eight respondents reported that they were sure their ‘other’ sexual partners were having sexual relationships with other people, while 20% (n=16) were not sure. Condom use Over half of the respondents, 54% (n=43) reported condom use at the time of their last sexual activity, 19% (n=15) reported no condom use while 27% (n=22) provided no response to the question (Table 4). Reasons for condom use included ‘wanted to prevent HIV/STD and pregnancy 20%, wanted to prevent pregnancy 5%, wanted to prevent HIV/STD 4% and 5% had other reasons for using condoms. Of those that reported no condom use at the time of their last sexual activity, four percent (n=3) of those who responded didn’t think it was necessary to use one. When asked the number of times in which a male or a female condom was used over the past six months prior to the interview by all the respondents, 16% (n=13) reported consistent use while 56% (n=45) provided no response to the question. Reasons for no use included not available 6%, he or she refused 4% and was offered something not to use 6%. Alcohol use Fifteen percent (n=12) of the survey respondents reported alcohol use at their last sexual encounter while fifty percent (n=44) of the respondents reported that they did not drink alcohol prior to last sexual encounter. Twenty-seven percent of the respondents provided no response to the question (Table 4). Within the past three months prior to the interview date, 8% (n=6) of all survey respondents reported alcohol use every time, 9% almost every time, 9% reported occasional use and 44% (n=35) reported never drinking alcohol before having sex with their sexual partner at the time (Table 4). Mean attitude scores Gender roles and norms Gender attitudes scores were further calculated by sex, and were considered low for each subpopulation, where the score for females were 16.7 (± 2.7) while the score for males were 16.3 (± 4.1). Both male and female respondents responded to similar questions. Sexual and Reproductive health The overall mean attitude scores for sexual and reproductive health were 24.5 (± 4.1) on a scale of 11 to 33, which was high and was considered generally positive. Risk factors and risky sexual behaviour Risky sexual behaviour is defined in this survey as having multiple sexual partners outside of a regular primary sexual relationship or regular non-primary relationship. In this survey, out of 48 respondents who responded to the question, fiftyeight percent (n=28) reported having ‘other’ multiple sexual partners outside of their regular primary sexual relationship or regular nonprimary relationships (Table 3). The relative risk (odds ratio) of this type of behaviour occurring among this sample size was associated by logistic regression analysis with living in urban areas, having ‘other’ sexual partners with expectation of receiving gifts, agreement to attitude statements including ‘a man has a right to demand sex whenever he wants’, ‘a man in a relationship needs to have plenty of sex with others in order to practice for his girlfriend’ and ‘women should be submissive to men in a relationship’ (Table 5). Discussion This survey was initiated in order to assess the prevailing attitudes regarding sex, sexuality, HIV/AIDS and other STIs, gender, and sexual and reproductive health and sexual behaviour of youth constituency workers from four constituencies who actively served at Tulongeni Youth Service Suppliers (TYSS), a nongovernment youth development organization within Oshana Region. This study identified factors that may influence prevailing attitudes and sexual behaviour which may be linked to the respondents perception of what is and what is not socially and/or culturally acceptable and how they can potentially impact the transmission of HIV. According to the Namibia Demographic Health Survey, almost two-thirds of all youth have comprehensive knowledge of HIV/AIDS, including knowledge on ways to avoid HIV infection16 . However, in spite of relatively high knowledge levels, it has been shown that knowledge itself is insufficient in preventing HIV transmission17, as reasons for persistence in high risk behaviour occur for a variety of reasons apart from individual knowledge and subject to external influences that need to be understood. Fifty-six percent (n=45) of the survey respondents (Table 2), a majority of whom, 53% (n=24) were from urban areas, believe that discussions around sex are inappropriate around women and children. These results are comparable to those of a focus group discussion that was conducted in Madagascar18 which also showed that discussions around sex and sexuality were taboo, and strictly forbidden, in reflection of the local culture; where people from urban areas were more reluctant to talk freely to one another about sex than their counterparts in rural areas, citing that formal education and westernization may have contributed to this reserve. This culture of reserve around sexual issues may have a negative impact on the spread of the epidemic especially among young people19. In 2007, it was found that women in the sub-Saharan Africa region comprised of 61% or more of HIV infected adults from the age of 16 years and above, with the highest prevalence among women 20 . If the general attitude towards empowering women and children, especially young girls to understand their bodies and the right that they have over them is negative, then it exacerbates and may continue to increase their risk of HIV infection. The survey data further reveals that of the fortyfive respondents who agreed with this statement, females exceeded the males in their response by a ratio of 24:21. This is in concurrence with studies that reveal where in some cultures, discussions on sex are seen by women as ‘inappropriate’ or ‘unbecoming’ of a young woman21, 22. In a society where men are encouraged to be sexually aggressive, it is easier for men to talk freely about sex but usually as a means of affirming their masculinity among their peers 23 . In informal discussions with the male respondents, it was confirmed by a majority that when men talk about sex with one another, it is usually an expression of masculinity. Ninety-two percent of the survey respondents agreed that parents should be able to talk to their children about sex (Table 2). While this was the majority response, many of the respondents concluded in informal discussion, that while they agreed with this statement, parents or adults still find it very difficult to talk about it because it is not socially acceptable for adults to talk to their children about sex and so ignore the issue completely or give biased information. These types of discussions should be encouraged as studies show a strong influence of parent-child communication about sex and HIV/AIDS on youth sexual behaviour, where the children of parents who were able to have discussions about this issue were less likely to engage in risky sexual behaviour24,25,26. In regards to attitudes on gender ideologies, some interesting variances are seen when one compares the response of men to women. In this survey, all the women (n=42) disagreed that men and women do have an equal say in a relationship. This response begs for a further understanding of the rationale behind how the way women under certain cultural and social contexts generally perceive their gender and their role in sexual relationships, which in many cases puts them in a position where they are unable to assert themselves or negotiate safer sex practices in a sexual relationship; behaviours which have been linked to an increase in vulnerability for HIV infection among women 27,28,29. Through informal discussion, many female respondents expressed that even though they wished to have equal say in their relationships, they felt obligated out of respect to their culture to be submissive and obey their male partners. A study conducted in Zimbabwe among university students also found that while women acknowledged genderbased cultural attitudes towards sexual decision making and respect their ‘gender roles’ in their relationship, as determined by their society and culture, they were much more likely to support women's rights to sexual expression30 . On attitudes towards condom use, the majority at (54%) felt that couples should stop the use of condoms and other contraceptives once they got married (Table 2). Informal responses to this suggest that condom use should stop, as it was socially unacceptable to use them and that agreeing to marry one another creates an assurance and trust that partners would not ‘intentionally’ hurt one another. However, while this may be perceived to be a social norm within marriages, studies show that married women in sub-Saharan Africa are considered a high-risk population where in some cases, more than fourfifths of new infections in young women occur in marriage or in long-term relationships with primary partners31 . Results from a study done in Ghana showed that married women are almost three times more likely to be living with HIV than women who had never been married32 . Sexual behaviour plays a very important role in curbing the HIV/AIDS epidemic among young people, especially when it is controlled and presents little or no risk to the individual or other sexual partners. Most respondents in this survey are sexually active, with (90%) reporting to ever having sexual intercourse, and the youngest age of sexual onset at twelve years. Studies show that compared to years ago, young people are initiating sexual activities at a much younger age and more specifically before the age of thirteen years 33 . A debatable topic, but while there have been proponents of abstinence only education, especially among adolescents34 , this result is indicative of the need to continue provide youth and adolescents at a much younger age with a more comprehensive sexual education that will empower them to choose and in the process remain safe, whether they decide to be abstinent or engage in sexual activity. This is also in concurrence with studies that recommend the benefit of policies and programs targeted towards adolescents and youth that provide a more comprehensive education, where abstinence is provided as an option of several behavioural goals as a means to prevent HIV and others STIs as well as unwanted pregnancy35,36. Our findings show that twenty-eight (35%) respondents reported sexual activity with partners outside of their primary sexual relationships and other regular non-primary relationships. This pattern appears to be the norm in this region of the world. A comparative study that was conducted by the World Health Organization (WHO), reported that 18%, 22% and 55% of men in the countries of Tanzania, Zambia and Lesotho respectively, reported having two or more regular, ongoing sexual relationships prior to the year of the study, as compared to only 3% and 2% of men in both Thailand and Sri Lanka, while 9%, 11% and 39% respectively of African women in these same countries reported two or more regular sexual relationships in the previous year compared to 0.2% and 1% of women in Thailand and Sri Lanka37 . Reasons for the high case of multiple or concurrent partners by both men and women include poverty and gender expectations. While more than half of the survey respondents (54%) agreed that the use of condoms should stop with a long-term sexual partner, more than a third (28%) who were already in regular primary sexual relationships or with non-regular primary sexual partners reported having multiple sexual partners within the past three months prior to the interview. With a combination of this type of prevailing attitude and sexual behaviour, the risk of HIV transmission is critical, especially in a situation where one or both partners in the relationship is unaware of the other partner’s sexual activity outside of their primary relationship and where both are not aware of the dangers of this practice, especially in a community where this type of risky behaviour is so prevalent due to societal norms that encourage multiple sexual partners38 . Limitations There are a couple limitations to this survey. Firstly, discussions around sex and sexuality are quite sensitive in most parts of Namibia, and therefore accurate information on these issues are relatively difficult to obtain. As the responses were self-reported, it was expected that respondents might deliberately conceal responses or might provide responses that are subject to limited recall. While measures were taken to reduce these inaccuracies including carefully selected and trained interviewers to administer the surveys and assurance of anonymity, it is likely that the proportion of respondents that engaged in high risk activities is actually higher than what was reported in the surveys. Secondly, while the survey administrators were fluent in both English and the local language, there might have been instances where questions asked could be misinterpreted by respondents upon translation. Nevertheless, this study makes important observations of relevance to youth sexual health and implications for programming and interventions throughout Namibia and much of Southern Africa. Conclusion Certain programs and interventions can be recommended for development and implementtation within a framework of empowering young people to make informed decisions about their health as they learn to understand social and cultural influences on HIV transmission. Advocating a complete change in long established cultures and traditions may appear insensitive and inappropriate. It is possible to allow young people to perceive the impact that certain cultural and social norms have on negative attitudes and risky behaviours that may increase the transmission of HIV and other STIs, and thus enable them make healthier and more informed decisions. Better and more unique comprehensive programs should be structured to address the cultural, social and historical context in which men and women relate to one another within the communities that they live in and how certain practices may exacerbate the spread of HIV. Stakeholders in youth health and HIV prevention may want to consider the following, within a framework of promoting healthier and more positive attitudes and sexual behaviours: Health providers and services Health providers serve as frontline responders in public health and therefore play an important role in meeting the sexual health needs of youth. Due to socio-cultural sensitivities around sexual health, it is vital that health providers acknowledge the importance of sexual health as part of the overall health needs of the today’s youth. Such recognition will encourage youth to take responsibility for their sexual health. Clinic or hospital staff including nurses and doctors can contribute to changing negative attitudes and sexual risk behaviours by encouraging interaction between themselves and young people who come in for visits and refraining from judgment or shying away from potential discussions around sexual and reproductive health, HIV/AIDS/STIs and sex. Providers may need to be specifically trained on providing youth friendly sexual health services with a view to dispelling harmful gender ideologies and practices that increase the risk of HIV infection. Government Government leaders, policy makers and authority figures in civic society and organizations that engage in youth and adolescent health can contribute towards developing and implementing policies and programs that encourage male involvement in sexual health while empowering young men and women to think and act outside ‘societal and cultural’ boxes in efforts to advance healthier sexual and reproductive health behaviours and encourage healthier attitudes. Leaders must adopt policies and enact legislation against harmful traditional practices that increase vulnerability to HIV and take measures to prevent violence against women and sexual minorities. Educators Educators possess the ability to shape the minds of young people from an early age to embrace a comprehensive understanding of sexual health in a way that will make discussion around sex and sexuality more acceptable in the society. Within the education sector, health education curriculum and programs must be developed to include a view of cultural and social approaches to improved health behaviours and attitudes in regards to sexual health, especially among young learners in schools. HIV education programs in schools must focus on greater sensitization on the traditions and cultural practices that increase the risk of HIV infection. There is a need for teachers to be adequately trained in providing HIV/AIDS education to young people in schools that underscores the challenges of promoting HIV prevention within their socio-cultural context and how they can be addressed. Parents and caregivers Parents and caregivers serve as gatekeepers in the home and are usually the first point of contact for information within a child’s community. As such, they should be in a position to provide pertinent sexual health information to their children as part of their development and growth. Parents can be encouraged to help dispel myths and stigma related to HIV/AIDS by educating their children from a suitable age on sexual health matters as this may allow for an early acceptance of and comfort with their sexuality so it becomes a healthy norm, and taboos against such discussions are broken. Parents and caregivers are also in a position to embrace positive gender ideologies, and put them into practice as they interact with one another within the home, breaking down stereotypes that are associated with sexual risk taking behaviour. Health providers should be able to work with parents in discussing sexual and reproductive health issues with their children. Youth The active involvement of youth in HIV prevention activities will ensure opportunities for young people to make meaningful contributions to the development, implementation and sustainability of interventions, policies and programs that promote sexual health within their sociocultural environment. Youth participation serves as a catalyst for engendering positive attitudes and promoting practices that embrace positive and more progressive gender ideologies. For young people out of school, avenues of youth participation through forums and workshops should continue to be organised for youth training of trainers that would allow for peer to peer education and discussions that would create a sustained capacity for youth to promote and adopt healthier lifestyles. Researchers Despite high rates of HIV/AIDS in Namibia and prevalence of sexual risk behaviours, very little published literature exists on underlying factors within the environment that influences the transmission of HIV. More research into the social-cultural and psychological factors that contribute to the HIV epidemic needs to be carried out. This will also serve to develop policies that are driven both by evidence and the reality on the ground and in the lives of youth. Acknowledgements This survey was made possible through funding by USAID/PEPFAR grants. While USAID supports policies, programs and projects to promote international health and development as a part of its objective, the views and opinions expressed in this paper are those of the authors alone. We are also grateful for support of Tulongeni Youth Service Suppliers (TYSS), a youth in development organization in Oshakati, Namibia and the respective constituencies that allowed the survey to be carried out. References
The following images related to this document are available:Photo images[rh10005t4.jpg] [rh10005t2.jpg] [rh10005t5.jpg] [rh10005t1.jpg] [rh10005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}