 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
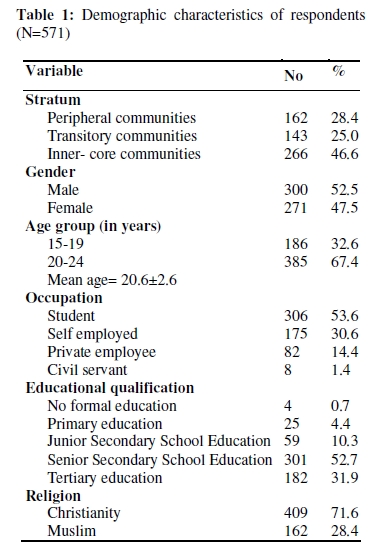
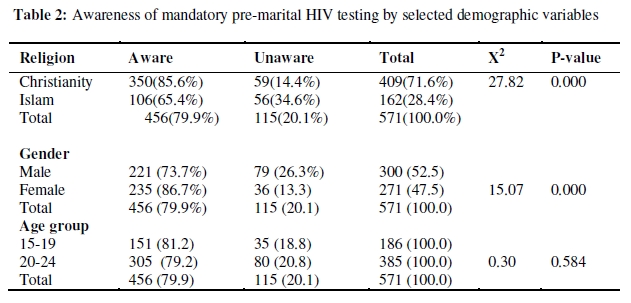
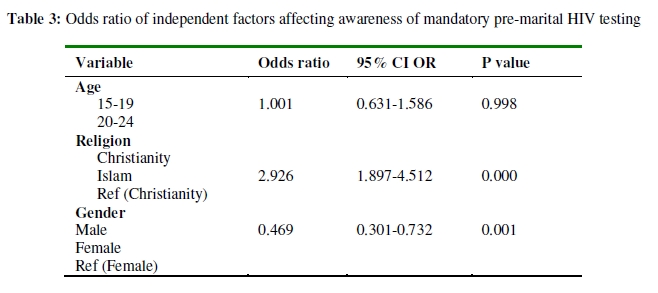
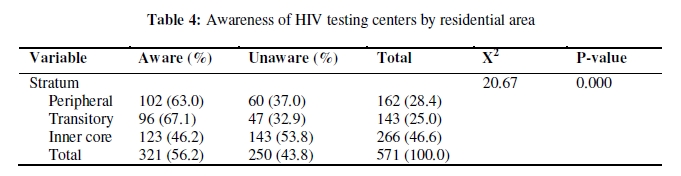
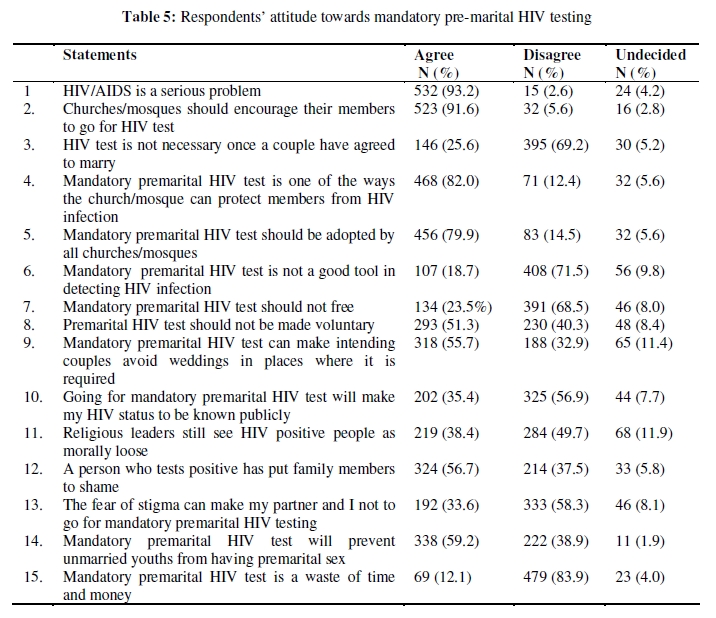
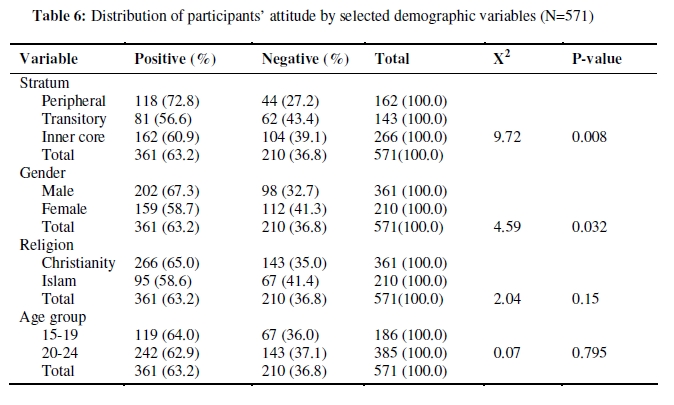
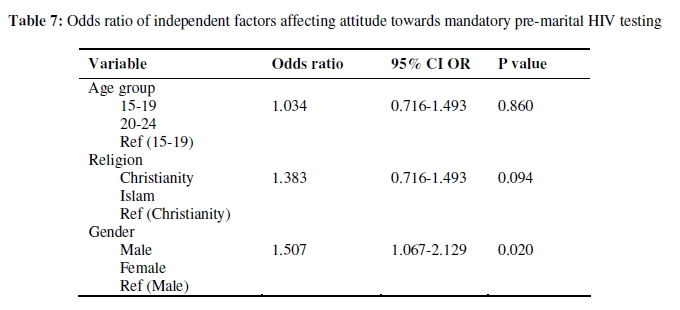
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 83-94 ORIGINAL RESEARCH ARTICLE Attitude Towards Mandatory Pre-Marital HIV Testing Among Unmarried Youths in Ibadan Northwest Local Government Area, Nigeria Oyedunni S Arulogun* and Olumide A Adefioye Department of Health Promotion and Education, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria *For correspondence: Email: omoyisola2002@yahoo.com Tel: 234-805-790-6536 Fax: 234-2411768 ABSTRACT This study assessed the attitude of unmarried youths towards Mandatory Premarital HIV Testing (MPHT) in Ibadan Northwest Local Government Area. A three-stage sampling technique was used to select 571unmarried youths from households. A validated questionnaire was used for the collection of the data. Descriptive, Chi-square statistics and logistics regression were used to analyze the data. Mean age of respondents was 20.6 ± 2.6 years, 52.0% were males and 52.7% had completed their senior secondary education. Though 82.8% believed that MPHT could reduce the spread of HIV, 43.8% stated that it will increase the stigma associated with HIV infection. Attitude towards mandatory pre-marital HIV testing however was positive. Males were about two times more likely to have positive attitude towards mandatory pre-marital HIV testing (OR=1.507, CI=1.067-2.129). Positive attitude towards MPHT among study respondents offers a window of opportunity of undergoing HIV testing before marriage (Afr J Reprod Health 2010; 14[1]:83-94). RĖSUMĖ Attitude envers le test obligatoire pour le vih avant le mariage chez les jeunes celibataires dans l’Administrativement Locale du Nord-ouest d’Ibadan, Nigeria. Cette étude a évalué l’attitude des jeunes célibataires envers le test obligatoire pour le VIH avant le mariage (TOVAM) dans l’administration locale du nordouest d’Ibadan. Nous employé une technique d’échantillonnage à trois étapes pour sélectionner 571 jeunes célibataires venant des familles. Nous avons collecté les données à l’aide d’un questionnaire confirmé. Nous avons analysé les données à l’aide des statistiques descriptives de la méthode de chi2 et la régression logistique. L’âge moyen des enquêtés était 20,6 ± 2.6 ans. 52,0% étaient des mâles et 52,7% avaient terminé leurs études secondaires. Bien que 82,8% aient été convaincus que TOVAM peut réduire la propagation du VIH, 43,8% ont déclaré qu’il augmentera la stigmatisation liée à l’infection du VIH. L’attitude envers le test obligatoire pour le VIH avant le mariage a été pourtant positive. Les mâles avaient deux fois la possibilité d’avoir une attitude positive envers le test obligatoire pour le VIH avant le mariage (OR = 1,507, Cl = 1,067 – 2,129). L’attitude positive envers le TOVAM chez les enquêtés donne la possibilité de faire le test pour le VIH avant le mariage (Afr J Reprod Health 2010; 14[1]:83-94). KEYWORDS: Spread of HIV, stigmatization, HIV testing Introduction One of the biggest health challenges threatening the human race in recent times is the HIV/AIDS pandemic. The disease has continued to be in the front burner for many years now, despite initial denials and cover-ups by some countries. UNAIDS estimated that globally, there were 33 million [30 million–36 million] people living with HIV in 20071. Overall, 2.0 million [1.8 million–2.3 million] people died due to AIDS in 2007, compared with an estimated 1.7 million [1.5 million–2.3 million] in 2001. Sub-Saharan Africa with just over 10 percent of the world’s population has the greatest burden of this disease. It is estimated that close to twothirds of all people living with HIV are in sub-Saharan Africa with South Africa having about 5.3 million people living with HIV/AIDS-the largest in Africa. The HIV/AIDS pandemic has significantly interfered with the gains which has been made in the area of health and development in many African countries over the years and has also reduced the quality of life. According to UNAIDS1 with AIDS claiming so many people’s lives, Nigeria’s life expectancy has declined. In 1991, the average life expectancy was 53.8 years for women and 52.6 years for men 2. In 2007, these figures had fallen to 46 for women and 47 for men. There is therefore a disparity between what ought to be and what is happening presently as regards the situation of HIV/AIDS in Nigeria. The disparity between what should have been and what will exist will worsen further if the HIV prevalence is allowed to rise further and the epidemic is not adequately controlled3. The response to the HIV/AIDS epidemic which was initially characterized by denial and inaction has gained greater recognition in Nigeria. The high point of the response was the establishment of the National Committee for the Control of AIDS (NACA) which has now become a full-fledged agency. The response to HIV/AIDS in Nigeria has not been limited to the government or government agencies alone. Other sectors and non-governmental agencies including religious bodies are also involved. In the early early days of the epidemic, the prevailing view among religious leaders was that God had sent AIDS as a punishment for sexual sins and other moral failings4. This view has changed as many religious bodies in Nigeria are now playing key roles in the fight against HIV/AIDS. As far back as 2002, the inter-faith HIV/AIDS Council was inaugurated with five trustees each from the Christian and Muslim faiths. Many religious organizations, in recognition of the fact that HIV/AIDS knows no religious boundaries have also developed policies to combat the spread of HIV/AIDS in their congregations. According to McCain 5, AIDS is affecting the religious community, as many of the people suffering from AIDS are religious people, members of churches and mosques. Controversies have however trailed the response to combat HIV/AIDS put in place by some religious organizations. A particular response which has attracted a lot of controversies is mandatory pre-marital HIV testing. Mandatory premarital HIV testing refers to the requirement of an HIV test as a condition for entering into marriage. The practice of mandatory pre-marital HIV testing which originated from the states of Louisiana and Illinois in the United States has also been documented in Nigeria, Democratic Republic of Congo (DRC), Ghana, Burundi and Uganda6. The Open Society Institute (2008) stated that in Nigeria in the late 1990s, Orthodox and Pentecostal churches began to require a mandatory premarital HIV test for those who wish to marry in the church. Mandatory premarital HIV testing, in spite of the opposition has continued to gain ground among intending couples. The 2005 National HIV/AIDS and Reproductive Health Survey showed that the number of people who desired HIV testing to fulfill mandatory marriage requirement rose to 3.0%7 from 2.4% in the 2003 survey. Furthermore, a study conducted among health care workers in North-central Nigeria revealed the support for the enforcement of pre-marital HIV testing for intending couples8. Orthodox churches such as The Anglican and the Baptist Churches as well as Pentecostal Churches such as Deeper Life Bible Church and Assemblies of God Church are some of the churches in Nigeria that have instituted mandatory pre-marital HIV testing. While the Baptist Church stated that the intention is to prevent HIV infection, rather than punish those living with the virus, the Anglican Church instituted the test to help couples make more informed choices when choosing marriage partners 9. Similarly, a report by the Center for the Right to Health 10 indicated the position of one the Pentecostal churches where this policy is in place that there was no need to continue marriage with somebody who already has a death sentence. In this case, the HIV infection is the death sentence. The human rights violation inherent in the practice, the limited population it targets as well as the belief that it is not a cost-effective HIV prevention and control measure has generated a lot of concerns particularly among human rights groups, government and nongovernmental organizations who are into HIV/AIDS-related issues.. According to Gruskin, Roseman and Ferguson 11 requiring individuals to submit to a pre-marital HIV test before being allowed to marry raises many of the human rights concerns such as voluntariness, privacy and confidentiality as well as appropriate counseling. Similarly, Uneke et al 12 stated that mandatory pre-marital HIV screening could generate social stigmatization and infringement of the fundamental human rights of infected individuals. Apart from the human rights concerns it has generated, there has also been concerns about the limited population such a strategy would target and the fact that they are not considered a group at risk of HIV infection13 14 . Umeora et al however do not share this view as in a study conducted to determine the prevalence of HIV infection among pre-marital couples in southeast Nigeria recommended that the screening of intending couples could play an important role in HIV detection in the general population. A study in Ghana showed that some religious leaders believed that their mandatory pre-marital HIV testing policy is their genuine way of protecting those who are HIV from becoming infected15 . Previous studies outside Nigeria indicated that in places where mandatory pre-marital HIV testing was instituted, few cases of HIV infection were detected at an enormous cost. For instance a study conducted by Rio et al 16 in Coahuila, Mexico revealed that only one new HIV infected person was diagnosed out of the 9,014 pre-marital tests that were done. This possibly made them conclude that mandatory pre-marital HIV testing is not only a violation of human rights but an expensive public health measure useless in the control of the spread of HIV/AIDS. However in Nigeria, studies conducted to determine the prevalence of HIV infection among intending couples referred from religious organizations for pre-marital HIV testing showed a relatively high HIV prevalence among intending couples12, 17. This may seem to justify the rationale for the institution of mandatory pre-marital HIV testing by some religious organizations. However, while previous studies have been able to determine the prevalence of HIV infection among intending couples, there has been no focus on the disposition of people to this policy. Youths constitute a substantial proportion of the population in Nigeria and have been identified as one of the sub-populations driving the spread of HIV in Nigeria. Furthermore, the issue of mandatory pre-marital HIV testing affects them especially the larger proportion who are unmarried. This study was therefore conducted to assess the awareness of mandatory pre-marital HIV testing among unmarried youths as well as their attitude towards it. Methods Study design The study was a descriptive and cross-sectional survey that assessed the awareness and attitude of unmarried youths aged 15-24 years in Ibadan Northwest Local Government towards mandatory pre-marital HIV testing. Setting and study population Ibadan Northwest Local Government is one of the local governments located in Ibadan metropolis. It has a population of 152,834 people of which 77,523 are females while 75,311 are males18. The inhabitants of Ibadan Northwest are mostly the Yorubas while the main occupation there are trading and working in the civil service. Ibadan Northwest is bounded on the north by Ido Local Government, on the south by Ibadan Southeast Local Government, on the west by Ibadan Southwest Local Government, and on the east by Ibadan Northeast Local Government. There are 11 political wards and 6 primary health centers (government-owned) in the local government19. The settlements in the local government are stratified along inner core (indigenous/slum-like), transitory (developed with little or no space for further development) and peripheral communities (developed with more space for development). The study population was made up of youths aged 15-24 years who were either Christians or Muslims. Sampling procedure A multistage random sampling technique was used to recruit 571 participants for the study. The first stage was the random selection of Ibadan Northwest Local Government from among the five local governments in Ibadan metropolis. This was followed by the stratification of the communities which gave a total of 28 inner core communities, 15 transitory communities and 17 peripheral communities i.e. 28:15:17. This ratio was used to calculate the sample size for each of the stratum thus giving a sample size of 266, 143 and 162 for the inner core, transitory and peripheral communities respectively. Systematic random sampling was used for the selection of communities from each of the three categories (in the ratio 7:4:4) and for selecting houses from the communities. In each selected house, the questionnaire was administered to a youth selected at random. Before the administration of the questionnaire, verbal informed consent was obtained from the respondents as well as parents/guardians/elderly people who were met at home. Trained research assistants administered the questionnaire on consenting youths. Confidentiality was ensured as no identifiers were included in the questionnaire. Interviews were conducted away from the hearing distance of other people while the collected data were stored in a secured place. Instrument for data collection A 43-item semi-structured questionnaire was developed and pre-tested in a location sharing similar characteristics with the study area. It was used to collect information on respondents’ sociodemographic characteristics, perceived severity and vulnerability to HIV/AIDS, awareness of mandatory pre-marital HIV testing as well as attitude towards mandatory pre-marital HIV testing from the respondents. In the attitude section, statements 1, 2, 4, 5 and 14 are positive statements and an affirmative response to each of these statements indicate positive attitude. Statements 3, 6-13 and 15 are negative statements and disagreement with these statements indicate positive attitude. Validity and reliability of instrument To ensure validity of the instrument, a draft of the questionnaire was constructed by consulting relevant literature, subjected to reviews from peers and other experts after which it was translated to Yoruba Language and backtranslated to English Language. The instrument was pre-tested in a location sharing similar characteristics with the study location. The pretested questionnaire was subjected to a reliability test using the Cronbach’s Alpha model. A reliability co-efficient of 0.781, higher than the average correlation coefficient of 0.5 was obtained. Nevertheless, some modifications were made to the instruments as tenses not easily understood were re-phrased and some removed while some of the questions were re-ordered to follow a logical sequence. Trained research assistants who are well-versed in both Yoruba and English languages collected the data for the study. Data analysis Each questionnaire was scrutinized for completeness, coded and entered into the computer. The SPSS Version 14 was used in analyzing the data. Descriptive, chi-square statistics and logistic regression were used for data analysis. All statistical tests were carried out at 5% (or 0.05) level of significance. The attitudinal level was assessed by assigning three points to a response that indicated positive attitude. No mark was given to any response that indicated negative attitude as well as the undecided responses. A 45-point scale was generated and respondents that scored 1-21 points were categorized as having negative attitude while those with 22-45 points were categorized as having positive attitude. Logistic regression analysis was also used to determine the independent factors affecting awareness and attitude towards mandatory pre-marital HIV testing. The dependent variable was coded as ‘1’ if respondent was aware of mandatory pre-marital HIV testing and ‘0’ if unaware. Also, positive attitude towards mandatory pre-marital HIV testing was coded as ‘1’ while negative attitude was coded as ‘0’. Results The socio-demographic characteristics of the respondents are as shown in Table 1. A total of 571 youths in the study site were interviewed. Of this number, 266 (46.6%) were from the inner core communities and 300 (52.5%) were males. The ages of the respondents ranged from 15 to 24 with a mean age of 20.6 ±2.6 years with 385 (67.4%) in the 20-24 age group (Table 1). Most of the respondents were students. The distribution of the respondents by educational qualification showed that 301 (52.7%) had the senior school certificate as their highest qualification while 4 (0.7%) had no formal education. Majority of the respondents 409 (71.6%) were Christians (Table 1). Perception of severity and personal risk of HIV Almost all the participants (95.6%) said HIV could cause diseases leading to death and only 166 (29.1%) reported that they were at personal risk of HIV infection. Eighty-eight (53.0%) of the respondents who agreed they were at risk were males while 78 (47.0%) were females. Awareness of mandatory pre-marital HIV testing Analysis of the respondents’ awareness of mandatory premarital HIV testing showed that 456 (79.9%) of the respondents were aware of mandatory premarital HIV testing while 115 (20.1%) were unaware. More Christians (85.6%) were aware than Muslims (65.4%) (p<0.05). Similarly, there was a significant relationship between gender and awareness of mandatory premarital HIV testing as awareness was more among females (86.7%) than males (73.7%) (p<0.05) (Table 2). Logistics regression of awareness on mandatory pre-marital HIV testing revealed that Christians were almost three times likely to be aware of mandatory pre-marital HIV testing than Muslims (OR=2.926, CI=1.8974.512) (Table 3) Respondents’ awareness of HIV testing centers More than half of the respondents (56.2%) were aware of HIV testing centers. The distribution of respondents’ awareness by their residential location showed that the awareness of HIV testing centers was more among respondents in the peripheral (63.0%) and transitory areas (67.1%) than those in the inner core areas (46.2%) (p<0.05) (Table 4). Respondents’ attitude towards mandatory premarital HIV testing Table 5 shows the attitude of the respondents towards mandatory pre-marital HIV testing. Majority (82.0%) agreed that mandatory premarital HIV testing is one of the ways the church/mosque could use to protect her members from HIV infection. Slightly more than half (51.0%) were of the disposition that premarital HIV test should not be made voluntary while (83.9%) disagreed that mandatory pre-marital HIV testing was a waste of time and resources. However, more than half (56.7%) agreed that a person who tests positive has put the family members to shame while 35.4% also agreed that going for mandatory pre-marital HIV testing would make their status known publicly. Overall mean attitude score was 24.1±5.2 out of 45. Three hundred and sixty-one (63.2%) had positive attitude while 210 (36.8%) had negative attitude. Religion had no significant relationship with attitude (p>0.05). There was a significant relationship between gender and attitude towards mandatory pre-marital HIV testing as more males (67.3%) than females (58.7%) had positive attitude (p<0.05). In addition, more respondents in the peripheral areas (72.8%) had positive attitude than respondents in the transitory (56.6%) and inner core areas (60.9%) (p<0.05) (Table 6). Logistics regression on attitude showed that males were about two times more likely to have positive attitude towards mandatory pre-marital HIV testing (OR=1.507, CI=1.067-2.129) (Table 7). Discussion The 15-24 age range for youths, as specified by the United Nations was used for the study and this explains the studentship status of majority of the study population. The larger number of males than females recorded in the study could also be a reflection of the 2006 population census which showed that there were more males than females in Nigeria18 . According to the 2006 Nigeria population and housing census, the sex ratio was 105 males to 100 females, which shows a slight preponderance of males over females contrary to the long-held belief that the population of females are more. The same trend was observed in Oyo State where the 2006 census figures showed there were more males (2,809,840) than females (2,781,749).18 Going by the 6-3-3-4 education policy in Nigeria, secondary education should have been concluded by 18 years of age hence a simple majority of the respondents had the senior secondary education as their highest level of education. However, the findings that only 31.3% had a tertiary education as their highest level of education could be a reflection of the difficulty in gaining admission into institutions of higher learning in Nigeria due to the fact that there are usually more candidates than institutions of higher learning in Nigeria can cope with or the poor economic situation. Though data on religion was not included in the 2006 census, the upsurge in the establishment of churches especially the Pentecostal breed and other Christian activities such as crusades, teleevangelism and other outreaches has expanded the frontiers of Christianity in Nigeria and has the possibility of increasing the number of the adherents of the Christian faith. This could account for the larger number of Christians than Muslims in the study. Perception of risk The low perception of self-risk of HIV infection among the study participants has also been reported in studies on HIV/AIDS conducted among populations such as intending couples, youths and college students20, 21, 22. This low perception of self-risk could constitute a hindrance to going for premarital HIV testing as it gives a false sense of security. Going by one of the key constructs of the Health Belief Model, perceived susceptibility, people’s beliefs about whether or not they were susceptible to disease, and their perceptions of the benefits of trying to avoid it, influenced their readiness to act.23 Awareness of mandatory pre-marital HIV testing A large majority of the participants were aware of mandatory premarital HIV testing as a wedding criterion by religious institutions. The high level of awareness buttresses the fact that mandatory pre-marital HIV testing has been in existence for quite some time. A documented report indicated that pre-marital HIV testing had started as far as the late 90s in Nigeria when orthodox and Pentecostal churches in Nigeria began to request it from those who wished to marry in the church6. The high level of awareness could also imply that more religious organizations are adopting it as a policy. Some demographic variables were found to have significant influence on awareness. Religion and gender were found to significantly affect awareness, as more Christians than Muslims and more females than males were aware of mandatory pre-marital HIV testing. The reason could be due to the fact that many Christian organizations have put in place various educative programmes on HIV/AIDS targeted at their members and many of the Christian religious organizations have a compulsory counselling session for intending couples which last for months before the marriage is conducted. In these counselling sessions, the intending couples are educated on issues regarding marriage and the home. Again, in most religious places in Nigeria especially in churches, there are usually more women than men. Attitude towards mandatory pre-marital HIV testing The assessment of the attitude of the participants showed a positive attitude towards mandatory pre-marital HIV testing. The agreement by a large majority that mandatory pre-marital HIV testing is one of the ways religious organizations can protect her members from HIV infection is consistent with the findings of the study conducted among religious leaders in Ghana and a report in Nigeria where it was stated that the need to prevent HIV infection was the reason religious organizations promote mandatory premarital HIV testing15,24. A negative view concerning this has however been expressed by some schools of thought. According to the Center for the Right to Health10, mandatory pre-marital HIV testing in the face of intense stigma and discrimination would drive vulnerable people underground and force them to avoid religious weddings completely. This means that people will avoid religious wedding in order to avoid the test, so, HIV infection will continue to spread unnoticed because those infected are unaware of their status and would continue to spread the virus unknowingly. Thus the purpose of instituting the test would have been defeated. This issue of stigma is a crucial one as many still believe HIV infection is brings shame as this study showed. Again, one of the weak points of mandatory premarital HIV testing which critics of the practice have highlighted is the false sense of security it could create. This false sense of security means when the result is negative for either or both couples, they tend to believe that they cannot never be infected with the virus again. According to Nair 25 , this false sense of security would encourage a casual attitude and lead to indulgence in high-risk behaviour without proper precautions. Again, since it is not as if testing negative at the pre-marital stage serves as a lifelong protection, it means the person who is HIV negative could be infected later in life especially if he/she or the partner engages in risk behaviours even inside marriage. This is in line with the position of Kamarulzaman 26 that premarital HIV testing is a one-off test while the risk of acquiring HIV is potentially lifelong.26 Many of the participants agreed premarital HIV testing should not be voluntary. This finding is similar to studies conducted among health workers in North-central Nigeria and religious leaders in Egypt8, 27. The fact that HIV/AIDS is deadly when not detected early and that intending couples may not voluntarily go for the test, as voluntary HIV testing is not common in Nigeria 14 may have influenced respondents’ disposition. Muula and Mfutso-Bengo 28 also hold a similar view. In a study conducted in Malawi, they recommended that since pre-marital HIV testing for couples and mandatory testing before marriage has not been accepted as yet by unmarried and married persons in Malawi, legal provisions should be explored to make such testing mandatory28 . Those opposed to the practice have however maintained that voluntariness, confidentiality and appropriate counseling should be the basis of pre-marital HIV testing. According to the Human Rights Watch 29 , HIV testing practices that were not voluntary, not linked to counseling and care and failed to protect confidentiality effectively discouraged people from seeking care and led to increased stigma and abuse. In this study, the issue of loss of confidentiality of HIV result/status in the context of mandatory pre-marital HIV testing also arose. There is the view that when a couple seeks religious blessings for their marriage, it is already common knowledge to the community of those intending to get married, if it then happens that the church or mosque refuses to bless the marriage after the tests results, then the confidentiality and privacy of the couple would have been breached. This probably made Uneke et al to advocate for voluntary counseling and confidential HIV testing as a basis for pre-marital HIV testing. Though this study revealed that the majority do not see mandatory pre-marital HIV testing as a waste of time and money, some previous studies have concluded that it is not cost-effective. Studies conducted in the United States and Mexico revealed that few cases of HIV infection were detected at enormous costs when pre-marital HIV testing was introduced16, 30. This thus informed their position that the practice was not cost-effective. As intending couples are considered to be a population at low risk of HIV infection, there is the view that subjecting them to HIV testing is a waste of scarce resources, a view not shared by Umeora et al 14 who recommended that screening intending couples-a population not considered at high risk for HIV infection could play an important role in HIV detection in the general population.14 It is also important to note that studies on the prevalence of HIV infection among intending couples referred to HIV testing centers by religious organizations in Nigeria showed a prevalence which ranged from 7.8% to 16.7% 12, 17. Considering that the current HIV prevalence in Nigeria is 3.1%1, the issue of costeffectiveness may not arise. Inspite of the seemingly high prevalence of HIV infection among this group, there is the need to consider the social stigma and other complications that would result especially when either of the couple tests positive and the concerned religious organization cancels or suspends the marriage. As pointed out by Musa et al 31 , who documented that if HIV testing is not well delivered, it could bring about serious complications including stigmatization, irrational decisions, HIV/AIDS spread, fast progression of HIV infection to AIDS and early death. This study also showed that more male respondents had a positive attitude towards mandatory pre-marital HIV testing. HIV infection is more prevalent among the female population as according to UNAIDS 1 women’s share of HIV infections is increasing in several countries. Similarly, HIV prevalence among the 15-24 age group in Nigeria was estimated at 2.3% for the females and 0.8% for the males1. The positive attitude could therefore be due to the belief that since HIV infection is more among women, men should have no fear of testing positive. According to Luginaah et al15, there is an implicit focus on the test results of women since they are perceived as more vulnerable. Some of the previous studies on HIV prevalence among intending couples have however shown a higher HIV prevalence among males 12, 32. Conclusion and Recommendations The study documented a high awareness level and positive attitude towards mandatory pre-marital HIV testing among the respondents. Positive attitude towards MPHT offers a window of opportunity of undergoing HIV testing before marriage. However, the issues of stigma and confidentiality still pose a great challenge as indicated by a substantial proportion of respondents who agreed that going for mandatory pre-marital HIV testing will lead to the loss of confidentiality of their status, that religious leaders still see HIV positive people as morally loose and that testing positive brings shame to the family. This has implications for the continued use of mandatory pre-marital HIV testing by religious organizations as a strategy to curtail the spread of HIV infection. Though the attitude may be positive, if the environment and the prevailing circumstances are not conducive, the positive attitude may not translate into action. The Health Belief Model explains that individuals conduct an internal assessment of the net benefits of changing their behaviour and decide whether to act, that is people are likely to take an action if the perceived benefits outweigh the constraint. In the light of these findings, the following are recommended:
References
The following images related to this document are available:Photo images[rh10007t5.jpg] [rh10007t3.jpg] [rh10007t7.jpg] [rh10007t6.jpg] [rh10007t2.jpg] [rh10007t1.jpg] [rh10007t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}