 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
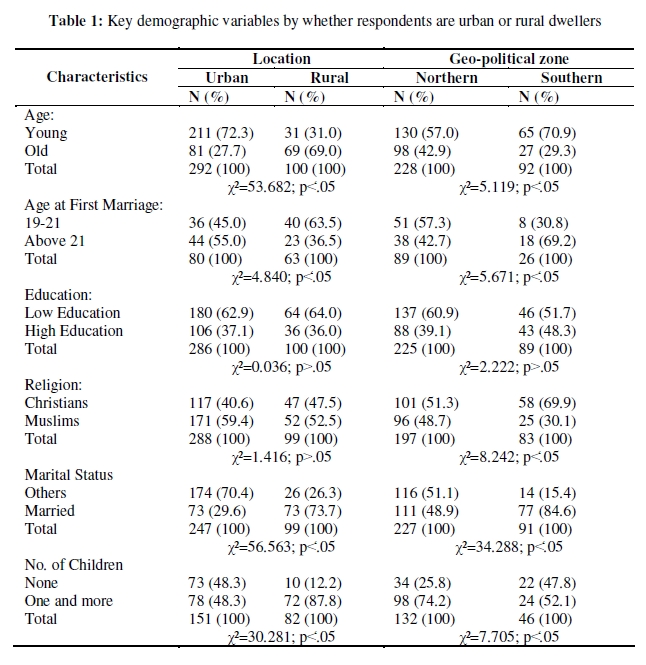
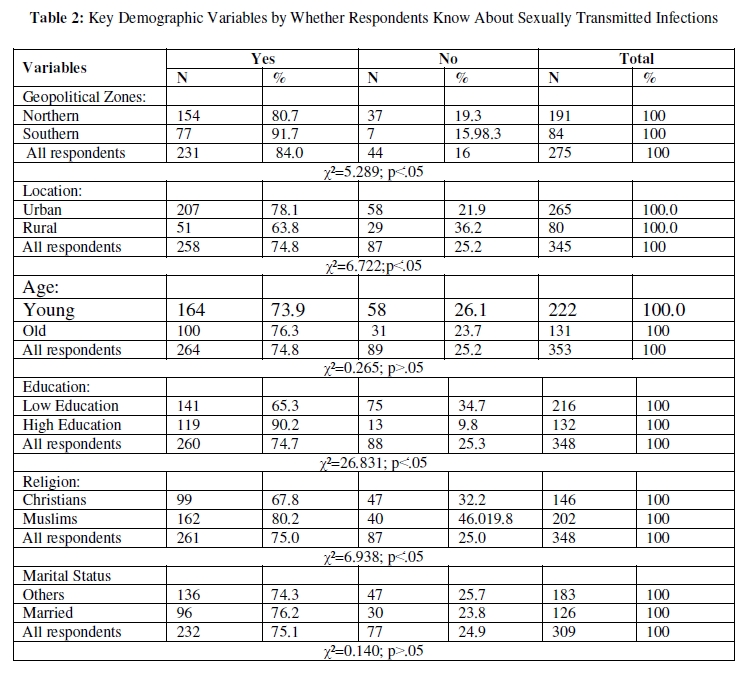
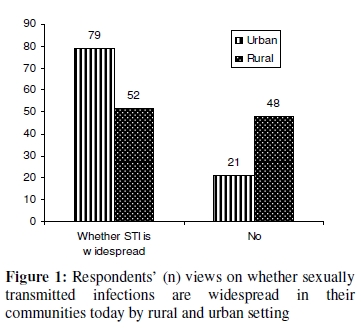
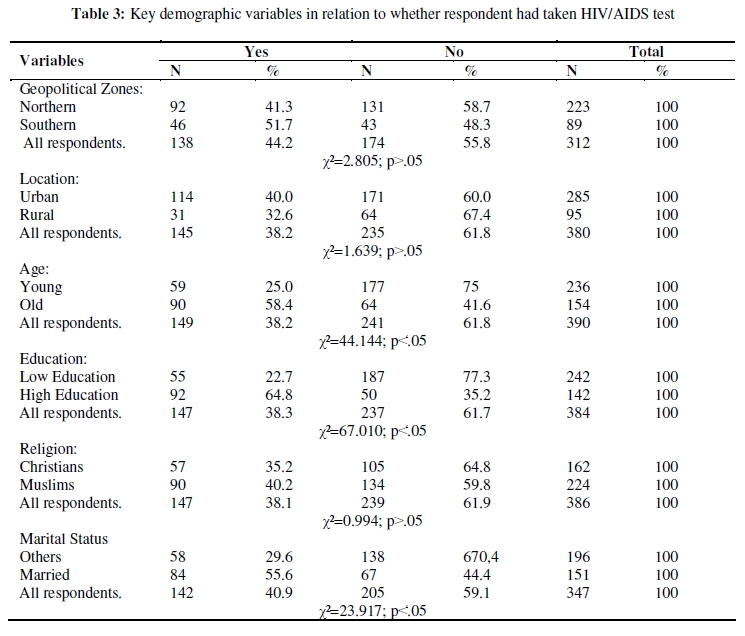
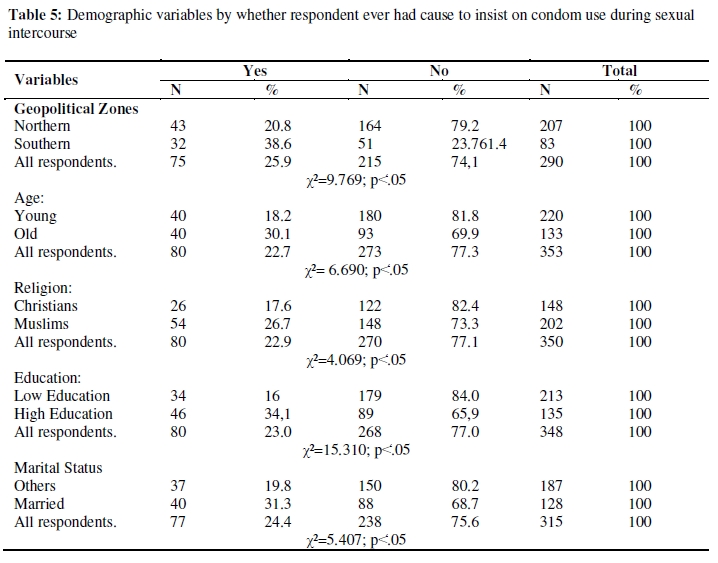
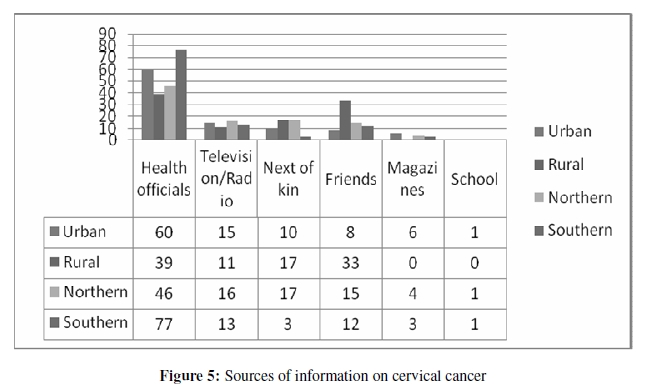
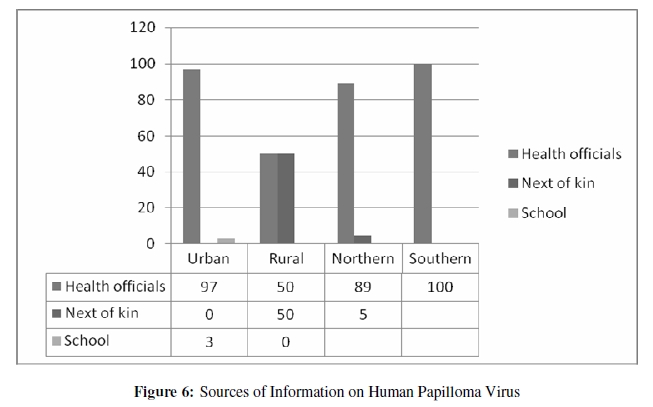
African Journal of Reproductive Health, Vol. 14, No. 1, March, 2010, pp. 95-108 ORIGINAL RESEARCH ARTICLE Knowledge and Attitudes towards Cervical Cancer and Human Papillomavirus: A Nigerian Pilot Study Connaissance et attitude envers le cancer du col et le virus du papillome humain : Une etude pilote Nigeriane Obiageli Nnodu1, Layi Erinosho2, Mustapha Jamda1, O Olaniyi3, Rabi Adelaiye1, Lovett Lawson1, Folakemi Odedina4, Fatima Shuaibu5, Theresa Odumuh6, Nnenaya Isu7, Hauwa Imam6, Olumide Owolabi8, Nuhu Yaqub9 and Andrew Zamani10 1Department of Haematology, College of Health Sciences, University of Abuja; 2Olabisi Onabanjo University, Ago-Iwoye; 3Department of Economics, University of Abuja; 4 Moffitt Cancer Institute, Florida, USA; 5Faculty of Education, University of Abuja; 6Institute of Education, University of Abuja; 7Faculty of Biological Sciences & Postgraduate School, University of Abuja; 8Computer Centre, University of Abuja; 9Formerly, Office of the Vice Chancellor, University of Abuja; 10 University of Abuja Teaching Hospital, Abuja. *For correspondence: Email: oennodu@gmail.com ABSTRACT This study aimed to ascertain the knowledge and attitudes of urban and rural dwellers to cervical cancer and HPV in Gwagwalada Area Council of Nigeria. 400 participants aged 15-45 years were selected from Gwagwalada town and the adjourning Giri village to respond to a multi-choice–free response questionnaire designed to obtain information on respondents’ biodata, knowledge of STIs, human papilloma virus and cervical cancer, health and communication resources in their communities. This was supplemented by focus group discussions among religious and tribal groups within the urban and rural communities. We found a low level of awareness about HPV and cervical cancer which majority felt could not be prevented. Although awareness of STDs was high in both urban and rural dwellers, condom use was low. The study underscores the need for a well planned and implemented health communication and education program on STIs, HPV and cervical cancer in Nigeria (Afr J Reprod Health 2010; 14[1]:95-108). RĖSUMĖ Cette étude avait pour objectif de vérifier la connaissance et les attitudes des citadins et des villageois à l’égard du cancer du col et du VPH dans l’arrondissement de Gwagwalada au Nigéria. On a sélectionne 400 participants âgés de 15 – 45 ans venant de Gwagwalada et le village venant de Giri, pour répondre à un questionnaire libre aux choix multiples qui a été conçu pour obtenir les renseignements sur les données sur la vie des enquêtés, leur connaissance des ISTs, le virus du papillome humain et le cancer du col, la santé et les ressources de la communication dans leurs communautés. Nous avons eu des discussions à groupe cible auprès des groupes ethniques et religieux au sein des communautés urbaines et rurales. Nous avons découvert un niveau bas de conscience par rapport au VPH et au cancer du col dont la majorité ont cru qu’on ne pouvait pas empêcher. Bien que le niveau de connaissance des ISTs soit élevé chez les citadins et les ruraux le niveau d’emploi des préservatifs était bas. L’étude met en évidence la nécessité d’avoir un programme de la communication de l’hygiène bien planifié qui porte sur les ISTs, le VPH et le cancer du dol au Nigéria (Afr J Reprod Health 2010; 14[1]:95-108). KEYWORDS: Human papilloma virus, cervical cancer, knowledge Introduction Cancer is a term used for malignant uncontrolled growth of cells and tissues. Cancer begins with irreparable damage to one or more genes controlling cellular growth, proliferation and apoptosis in a single cell which results in further genetic damage leading to abnormal cellular proliferation and evasion of the body’s immune system. The process by which a normal cell becomes cancerous may take many years. Initially, cancer cells are localized to a site or region of the body but eventually cancer cells acquire the ability to spread to other parts of the body. The risk factors for cancer are modifiable factors such as tobacco use, unhealthy diet, infectious agents like human papilloma virus, hepatitis B virus, helicobacter pylori bacterium, ultra violet radiation, physical inactivity, occupational exposures, food contaminants e.g. aflatoxin, ionizing radiation, obesity. Nonmodifiable risk factors include ageing, ethnicity, heredity, sex, immunosuppression and reproductive factors. According to the American Cancer Society (2006), 1.9 million (i.e. 17.8% ) of the cases of cancer worldwide were caused by infections and about 1.4 million (i.e. 73.7%) of these occur in developing countries.1 There were estimated 11 million new cancer diagnoses and 7 million cancer deaths throughout the world in 2002. Moreover, the number of new cases of cancer and deaths that occur due to the disease are expected to rise to 16 million and 10 million respectively by 2020 with close to 70% of the deaths in developing nations (UICC World Cancer Congress, 2006) 2 Estimated cancer incidence in Africa is 70/100,000-100/100,000 population. The commonest cancer in men is Kaposi sarcoma (15.5%) with cancer of the cervix representing 22.2% of all cancers among women. Most cases present at advanced stages when curative measures may be unsuccessful.3 The incidence rate of cervical cancer in Nigeria is 25/100,000 while the reported prevalence rates for HPV in the general population and HPV in women with cervical cancer are 26.3% and 24.8% respectively. High risk HPV types 16, 31, 35, 56 were found with infections involving more than one HPV type and high prevalence of HPV in all age groups 4-5 . There is a high burden of cervical cancer with mean age of patients of 52.4 years within the Federal Capital Territory, (FCT). Age at first confinement in affected women was between 12-19 years, with an average age of 15 years and 86% of patients presenting late6. Knowledge about cervical cancer and Pap smear tests was very poor from studies conducted across the country7-11. This is reflective of the situation in most of Africa where low level of awareness about cancer among policy makers and the general public, high illiteracy rate among the general population, the HIV/AIDS epidemic with its virus–associated cancers, and dwindling health allocation to non-HIV diseases have been cited as part of the problems encountered in cancer control.5 Cancer control describes the totality of activities and interventions that are intended to reduce the burden of cancer in a population either by reducing cancer incidence or mortality or by alleviating the suffering of people with cancer. Prevention, early detection, diagnosis, treatment, psychosocial support, and palliative care are components of cancer control that can reduce the cancer burden.12 Nigeria’s Cancer Control Plan 2008-2013 is aimed at providing information and education through outreach services nationwide. Cervical cancer is one of the greatest threats to women’s lives. In 2005, 260,000 women died from it globally, nearly 95% of them in developing countries. The primary cause of cervical cancer is infection with one or more types of high risk human papilloma virus (HPV) which is transmitted by sexual contact. Although most new HPV infections resolve spontaneously, persistent infection can lead to the development of pre-cancer and subsequent cancer over many years. Experience from developed countries has shown that well planned and organized screening programs with high coverage of the “at risk” group could significantly reduce the number of new cases with cervical cancer and the mortality rate associated with it. This is also achievable in developing countries as exemplified by a recent report where a single round of HPV testing was associated with a significant reduction in the numbers of advanced cervical cancers and deaths from cervical cancer in rural India.13 In general, awareness about cervical cancer, availability of effective screening programmes and improvement of existing health services could reduce its burden among women. One of the main reasons for the huge difference in its incidence and mortality between developed and developing countries is this lack of awareness among the population, health care providers, and policy makers in the latter.14 Thus, the transmission of information and acquisition of knowledge on the etiology and how the disease can be prevented could reduce exposure to known risk factors. Although cervical cancer had not received as much attention as it deserves from the health authorities, there is a present move to increase, educate, and disseminate cancer information through outreach services nationwide as reflected in the 2008-2013 National Cancer Control Plan of Nigeria. This is more so now with the availability in 2006 of a prophylactic vaccine that protects against four major HPV types as high level of awareness is essential for the success of any large scale prevention program. It is against the backdrop of the foregoing remarks that a pilot study to ascertain the knowledge and attitudes of urban and rural dwellers in Nigeria to cervical cancer and HPV was conceived. It is envisaged that the outcomes of the study will provide the basis for a nationwide cross-sectional study followed by educational and other interventions for the prevention of cervical cancer in Nigeria. Methods Setting The study was conducted in Gwagwalada, a rapidly growing satellite town of the Federal Capital Territory (FCT) Abuja which is about sixty kilometers from the Capital City. Giri village is located between the Capital City and Gwagwalada and is within twelve kilometers of the latter. Gwagwalada is a university town which also draws its residents from civil servants who work in the FCT. Sample and Sampling Female respondents from the age of 15 to 49 years who either were in-school and out-of-school were targeted in these communities. Respondents from urban (300) and rural (100) areas were selected by purposive random sampling after a series of focus group discussions among teachers, nurses, patent drug dealers and members of the communities. Data Collection Two strategies were adopted in the course of data collection. First, a series of focus group discussions were conducted among key health workers and community members in order to ascertain how to proceed with the study (Appendix I). This was with a view to exploring the local words and/or expressions for the diseases that are to be studied. Another reason was to gauge reaction to study on such sensitive issue and find how best to pose questions concerning their personal life in the context of sexuality and sexual mores that are likely to arouse concern, hostility, and possibly negative reactions from them. Two groups were constituted in the village and four in the urban centres. The researchers took into consideration the distinct attributes of those who were invited and brought those who shared fairly similar attributes into each group in order to ensure unfettered interaction among participants. The discussions were conducted in local languages and the outcomes provided ample data for design of the instrument that was administered. Secondly, a questionnaire which was administered in local languages was designed to gather the following data from the respondents:
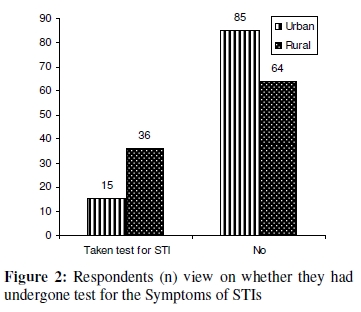
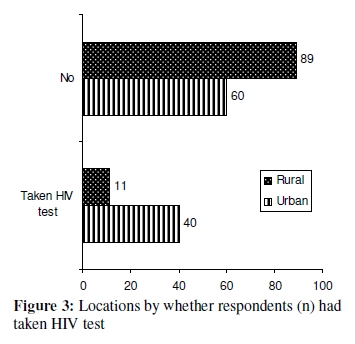
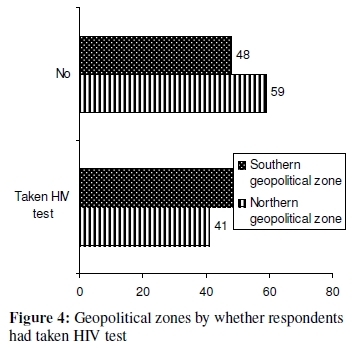
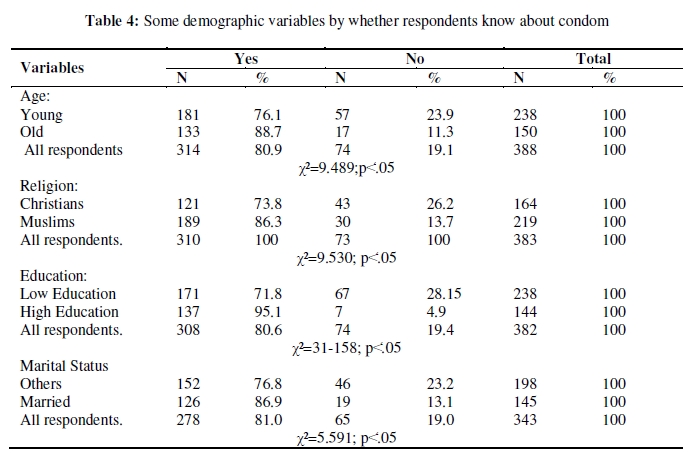
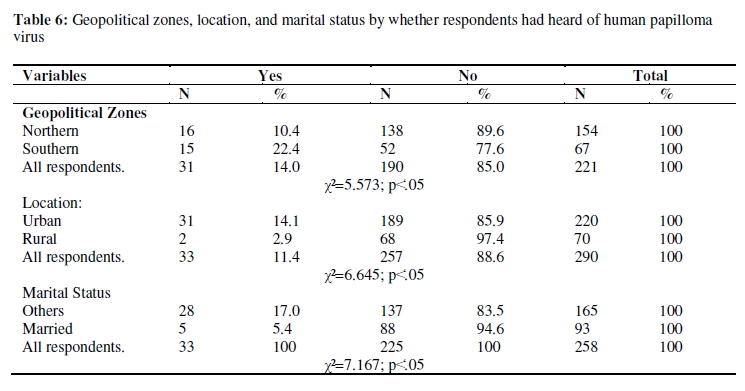
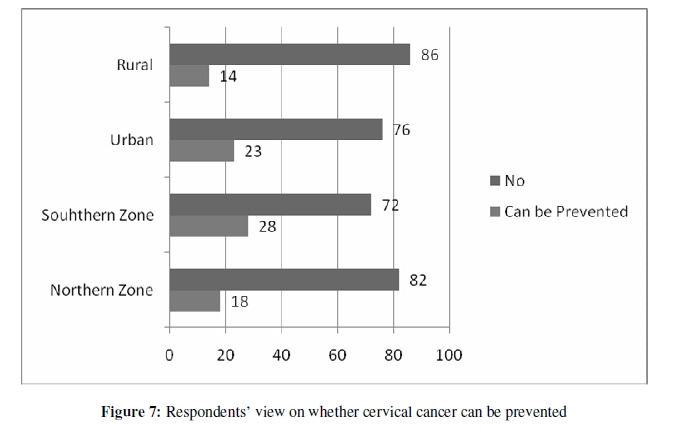
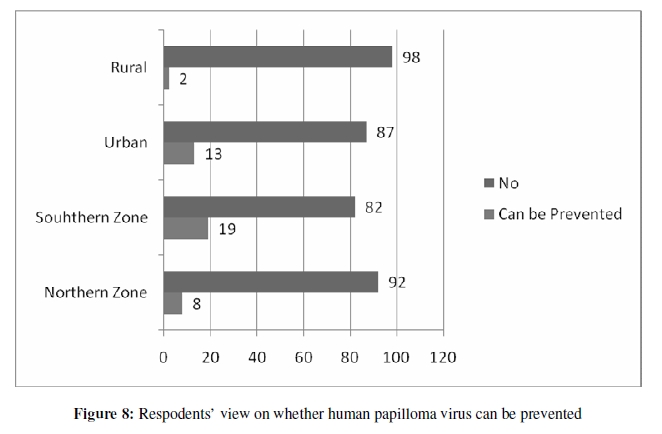
The initial plan for the survey was to administer the study instruments on secondary school students in their schools. Disruption of school calendar by the nationwide teachers’ strike however necessitated a change of plan and the students were eventually seen in their homes. In each case, parental consent was obtained prior to the administration of questionnaire. Ethical Considerations There was no physical risk to the respondents except for the occasional discomfort participants felt regarding the sexual themes during the interview which was minimized by ensuring that the interviews were conducted privately. The respondents were approached after sensitization visits to schools and permission obtained to conduct the study. Informed consent was sought from the school authorities, parents and students as appropriate. At the community levels permission was obtained from village heads/male and female community leaders, and consent was sought from individuals that participated in the study after study details were disclosed to them. Informed consent was granted either by thumbprints for illiterates or by the signing of informed consent form. Consent was also obtained from participants to record focus group discussions on tape. Respondents were assured of confidentiality for their individual responses, which was achieved through the use of non–biographical identification codes. Participants were assured that information obtained from their respective communities would be shared with them to enable them participate in a meaningful way in the intervention programs to be implemented thereafter. The guides for the focus group discussions among key subgroups and summary of findings can be seen in appendices. Data Analysis The Focus group discussions were transcribed soon after each session from tape recordings, analyzed by identifying important themes, proportions and summarized in a table. Data obtained were entered into the computer and manually checked for errors while SPSS was used to analyze them. To achieve the objectives of this study, both descriptive and inferential statistics were used to analyze the data. In particular, chi-square statistics were used to estimate the degree of correlation between the variables in the study. This was preferred over multi-variate regression analysis which may be prone to the problems of multicoliniarity and or heterodasticity due to the nature of the independent variables in this study. P values less than 0.05 were considered significant. Results Table 1 indicates the characteristics of the respondents in the two communities. The variables were re-grouped for ease of analysis. Age was grouped into young and old using the mean age of 24 years as dividing line; 24 years and below as young while above 24 are grouped as old. Those who completed primary school were in the low education subgroup in contrast to those with high education which incorporated all respondents who attained the educational level that was higher than primary school. The married were compared to ‘others’ subgroup which incorporates a few who were divorced, separated, and widowed in the sample. The proportions in the table indicates that the respondents from the two communities were similar in some respects and not in others judging by the chi-square results. One could surmise that younger respondents were drawn from the urban than the rural (χ²= ̒53.682; ˂.05) while more of those whose age at the first marriage was between 19 and 21 years were from the rural than in the urban setting (χ² = 4.840; p˂̒.05). A larger number among the “Others” in marital status category was from the rural than the urban (χ² = 56.563;p˂̒.05). The table also shows that a greater proportion of respondents with one or more children were from the rural than the urban setting (χ²= ̒30.281; ˂.05). However, the proportions of those who were selected from the two groups in the context of education and religion were similar. The sample was sub-divided into whether the respondents were from the Northern or Southern geopolitical zones into which Nigeria is administratively sub-divided. The aim was to ascertain similarities or dissimilarities in the proportions of the respondents. The outcomes are also shown in Table 1 when some demographic variables were used in the analysis. It appears that there were larger proportions of young and married respondents from the southern than the northern zones (χ²=5.119; p ˂̒̒.05) and χ²= 8.242; p ˂.05) respectively. The northern and southern respondents differ on the basis of religion and number of children. More of the respondents of northern zones origin had more children than those from the southern while more of the respondents of southern zone origin were Muslims (χ²=7.705; ˂.̒05 and χ²= 8.242;p˂̒.05;). The fact that Christians more were among the respondents from the north is not consistent with the geographical distribution of the adherents of Christianity and Islam in Nigeria. However, the FCT where the study was conducted is located in the North Central zone which is home to many Christians. The chi-square result in the context of education is not statistically significant (χ²= 2.222; p˃.05). Outcomes The outcomes are subdivided into two broad areas: first an attempt was made to discuss those which deal with knowledge about aspects of reproductive health and their consequences including those on condom, followed by those on cervical cancer and human papillomavirus. The respondents were asked a series of questions on knowledge of sexually transmitted diseases and their prevalence in their communities including whether they had ever undergone test for symptoms of Sexually Transmitted Infections (STIs) and HIV/AIDS test. Other questions focused on condom use and whether they felt that its use is widespread today. Table 2 shows the relationship between a number of demographic variables and knowledge about sexually transmitted diseases. Majority of the respondents were aware of STIs. The proportion of the group that had knowledge from the Southern Zone was greater than in the Northern (χ²=5.289; p˂̒.05) while more from the urban than rural (χ²=6.722; p˂̒.05); high than low education subgroup (χ²=26.831; p˂̒.05); and Muslims than Christians (χ²=6.938; p˂̒.05) had. By and large, the outcomes on age and marital status are not statistically significant (χ²=0.265; p˃.05 and χ²=0.140; p˃.05 respectively). Significant proportions among the respondents in urban and rural setting (χ² = 16.13 p < 0.00005), supplemented by data from focal group discussions showed that sexually transmitted infections were widespread in their communities (Figure 1 & Appendix II). Table 3 and Figure 2, Figure 3 and Figure 4 show interesting outcomes on respondents who had undergone test for HIV/AIDS including STIs. Even though large proportions of the respondents in the different locations (urban and rural as well geopolitical zones) had never taken a test, a close look at the table shows some statistically significant results on age, education and marital status. More respondents among the young than old, those with low education than high, northern than southern, Muslims than Christians had not taken tests for HIV/AIDS ((χ²=44.144; p˂̒.05; χ²=67.010; p˂̒̒.05; χ²=23.917; p˂.05 respectively). Overall, more know about condom while larger proportions among the old than the young, Muslims than Christians; those with high education than low, the married than the others know about condom as shown by the Chi-square results in Table 4. More among the old respondents than young; those with high education than low are inclined to use condom during sexual intercourse though there was general failure to insist on condom use during sexual intercourse across all peoples from all political zones, age groups, religion educational and marital status. (χ²=9.769; p < 0.05, χ²=6.690; p < 0.05, χ²=4.069; p < 0.05, χ²=15.310; p < 0.05, χ²=5.407; p < 0.05 respectively in Table 6). This was buttressed by these remarks from FGD participants: “Even if we know that our men are going outside, we are helpless to protect ourselves”…“They even beat women who want them to use condom” Knowledge of Cervical Cancer and Human Papilloma Virus As previously indicated, the respondents were asked if they know of cervical cancer and human papilloma virus and the outcomes indicate that very small proportions know about these diseases (Table 5). However, a close analysis indicates that more among the old (X2=17.793; p < .05) and those with high education (X2=23.049; p < .05) had heard about cervical cancer while more among the southern, urban and the ‘Others subgroups’ in the sample in contrast to those among the northern, rural and married ones have heard of human papilloma Virus (X2=5.573; p<.05, X2=6.645; p<.05, X2=7.167; p<.05 respectively in Table 6). Sources of Information The sources of information for cervical cancer include health officials, television, next of kin, friends, magazines, and school almost in the order of importance in the geopolitical zones and locations whereas sources for human papilloma virus are confined to health officials and the school. Health officials appear to be the most important source of information on these diseases (Figure 5 and Figure 6). Prevention An overwhelming majority of the respondents said that cervical cancer and human papilloma virus could not be prevented and this is much more so among the latter judging by Figure 7 and Figure 8. However, a close review of the figures indicates that slightly more among the urban and southern zone respondents than in the rural and northern zones who felt that these conditions could be prevented. Analysis of the open ended responses reveal that large proportions of the respondents know about sexually transmitted infections and could describe some of the symptoms of a few very clearly and correctly .They also acknowledged that they are widespread in their communities. However, only very small proportions among them had undergone test for STIs and HIV/AIDS. Closer analyses show differences between sub-groups with reference to young vis-à-vis the old; between those with low and high education and the married and others. Besides, the outcomes suggest that large proportions in the sample know about condom while about a quarter ever had cause to insist on it use during sexual intercourse. There are also significant differences between respondents from the northern and southern geopolitical zones into which the country is adminsitratively subdivided; young and old, respondents, religious subgroups and also between those with low and high education and the married and “Others”. Generally nearly two-thirds of the respondents observed that many Nigerians are inclined to condom use today even though in practice many would not insist on condom use (Table 5). Only 26 per cent of those who responded in the study had heard of cervical cancer and fewer still about human papilloma virus (14 per cent in Table 6) while health workers are the most important sources for information on these diseases, followed by the media and next of kin. Finally, very small proprtion of the respondents felt that these conditions could be prevented. Discussion The low level of awareness about the human papilloma virus and cervical cancer in our study population is consistent with that of previous authors both within and outside the country11, 15, 17. These studies had examined the knowledge, attitudes, beliefs within the community, among college students, adults attending general out patients but our study was done in both an urban as well as rural setting where health personnel were identified as the most important source of information on these diseases followed by the media and the next of kin. One strength of our study is the use of both quantitative and qualitative methods which have shown a low level of condom use despite the high incidence of STDs in the community. The number of respondents was 400 but this was supplemented by focus group discussions among the various community groups. The information from the focus group discussions high lighted what we found in the quantitative survey namely, that people were not aware about HPV and cervical cancer but expressed a willingness to know more and to avail themselves of any preventive interventions. This low level of awareness of HPV and cervical cancer in contrast to the high level of awareness about STI in the respondents and low insistence on condom use during intercourse shows a knowledge practice disconnect which can be fuelling the transmission of sexually transmitted diseases within the community. It establishes a strong case for education awareness and other interventions in the community against HPV infections, especially the pathogenic strains which cause cancer. Concluding Remarks There is a window of opportunity for a much bigger study than this pilot study in the FCT area. This is because the experience gained from data collection would be useful in the development of a nationwide project. More importantly, the outcomes underscore the need for health education aimed at helping the community to appreciate the etiology of these conditions and also preventing STIs and HIV/AIDS. Acknowledgments We acknowledge the generous grant from Zankli Medical Centre that made this study possible, the support and cooperation of the traditional rulers, council community leaders, traditional healers and birth attendants of Bassa, Gbari and Hausa communities in Gwagwalada and Giri village for the mobilization for the focus group discussions. We are also grateful to Community Health Officer for help in reaching the community resource persons in Giri village. We also thank the Principals of the secondary schools for granting access to the students as well as the clerics who facilitated access to the Muslim and Christian communities in Gwagwalada. Appendix 1 The guides for the discussions among the key subgroups FGD with Key Health Workers: What are the known sexually transmitted diseases in Gwagwalada and its environs? What are the local expressions for the various sexually transmitted diseases? What would the members of the community find offensive in work on sexually transmitted diseases? Are participants acquainted with cervical cancer and human papailomavirus? In what ways can researcher pose questions in order to ascertain knowledge, beliefs and attitudes to cervical cancer and papillomavirus in the targeted communities? FGD Guide with Members of the Communities: What are the major reproductive health problems that the respondents know about in the community? Are they aware of sexually transmitted diseases and its incidence in their communities? Which are the most commonly known among the STIs? What the beliefs about these diseases and how can they be prevented? What is the most effective means of educating the members of the communities on sex and sexually transmitted diseases? Have they heard about cervical cancer and human papillomavirus? Would they like to know about them? How best can members of their community be educated on cervical cancer and human papillomavirus? References
The following images related to this document are available:Photo images[rh10008t1.jpg] [rh10008f2.jpg] [rh10008f8.jpg] [rh10008t3.jpg] [rh10008f3.jpg] [rh10008t6.jpg] [rh10008f1.jpg] [rh10008f5.jpg] [rh10008t5.jpg] [rh10008f7.jpg] [rh10008f4.jpg] [rh10008t4.jpg] [rh10008t2.jpg] [rh10008f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}